
Abstract
Background:
Increased weight gain in children during the COVID-19 pandemic has been reported. Changes in weight in children with asthma during this period have not been well described.
Methods:
Retrospective review of children with asthma, 6–18 years of age, seen in 2019 and 2020. Mean monthly rates of change in body mass index (BMI) were compared between years. Demographic and asthma-related factors were examined.
Results:
Two hundred sixty-seven patients were enrolled. BMI increased by 0.128 ± 0.283 kg/m2/month during the pandemic year as compared with 0.084 ± 0.160 kg/m2/month during the previous year (P = 0.03). Patients with baseline overweight or obesity trended toward higher rates of BMI increase than those starting with normal weight, with the greatest BMI increase occurring in the severely obese.
Conclusions:
In this single-site study of children with asthma, there was a greater monthly rate of BMI gain during the early pandemic as compared with that observed in the previous year.
Introduction
Pediatric obesity is an epidemic in the United States, with >35% of children and adolescents classified as overweight or obese. 1 In school-aged children, a pattern of increased weight gain is seen during summer breaks.2,3 Early in the COVID-19 pandemic, schools remained closed across the country in efforts to contain viral spread. In New York State, schools were closed in late March and remained closed for the final 3 months of the academic year. Stay-at-home orders were in place until June 8, 2020. After this time, phased reopening occurred gradually over the next 2 months, although many families, including those with children with chronic respiratory illnesses, chose to remain home.
In September 2020, some students returned for part-time in-person learning, while others opted for online learning. There were early concerns that extended school closures with decreased access to sports and structured activities would exacerbate risk factors for obesity, including sedentary lifestyle, increased screen time, increased caloric intake, and food insecurity. 4 Our objective was to assess the impact of these closures on weight changes in a high-risk group of children with asthma.
Obesity in children and adolescents is associated with greater risk of cardiovascular disease and diabetes in adulthood.5,6 Overweight status is a risk factor for development of asthma in school-aged children 7 and a disease modifier associated with poorer control, more frequent and severe exacerbations, and reduced response to therapy.8–10 Accelerated weight gain in children with asthma therefore has sequelae beyond the health effects of obesity in the general population. We hypothesized that children and adolescents with asthma would have a greater rate of increase in body mass index (BMI) in the first year of the pandemic, when schools were closed for an extended period, compared with the previous year.
Methods
A retrospective chart review was performed on patients 6–18 years of age with asthma seen at a predominantly suburban, pediatric pulmonology practice, in New York during 4 periods: January–April 2019, July–October 2019, January–April 2020, and July–October 2020. Periods were selected to capture differences before and after the extended school closure during the first year of the pandemic. The Institutional Review Board approved the study, including a waiver of informed consent. Patients were included if they had in-person visits, with height and weight, during all 4 periods. Patients with chronic respiratory illnesses other than asthma were excluded. Other excluded diagnoses included neuromuscular disorders, genetic syndromes, cerebral palsy, failure to thrive, and gastrointestinal disease.
For each visit, height, weight, asthma medications, and exacerbations requiring systemic corticosteroids in the preceding 3 months were recorded. BMI and BMI percentile for age were calculated using the Centers for Disease Control's online tool. 11 Patients were categorized by percentile as underweight (<5th), normal weight (5th to <85th), overweight (85th to <95th), or obese (≥95th). Patients were classified as severely obese if the BMI was ≥120% of the 95th percentile for age and sex. 12 Asthma severity was classified as Step 1, 2, or 3 or Steps 4 and 5 per Global Initiative for Asthma guidelines. 13
Means and standard deviations are reported. Proportions were compared using chi-square tests; means were compared using paired and unpaired t-tests. Prevalence of overweight and obesity and mean monthly rates of change in BMI before and during the pandemic were compared. Two-tailed P-values of <0.05 were considered statistically significant.
Results
Table 1 summarizes baseline patient characteristics. A significantly higher proportion of overweight/obese patients were Black (P = 0.03) or Hispanic (P = 0.03) compared with normal weight patients. A significantly higher proportion of overweight/obese patients had state-funded insurance (P = 0.02) compared with normal weight patients. Asthma severity was classified as moderate or severe in 54% of the cohort, with no differences between weight categories.
Patient Characteristics by Weight Category at Start of Study
One hundred thirty-six patients (51%) were overweight or obese by the end of 2020 compared with 47% in the prepandemic year (P = 0.34). Over the study period, the prevalence of normal weight decreased while the prevalence of overweight and overweight/obese increased.
The overall rate of BMI increase was 0.128 ± 0.282 kg/m2/month during the pandemic year compared with 0.084 ± 0.160 kg/m2/month in the previous year (P = 0.03). Although patients in all weight categories demonstrated higher rates of BMI increase during the pandemic compared with the prepandemic year, only those who were severely obese at baseline had a statistically significant change (Table 2).
Rate of Change in Body Mass Index Before and During the Pandemic
BMI of ≥85th percentile.
BMI of ≥95th percentile.
BMI, body mass index.
BMI steadily increased for children in all weight categories over the study period, with the smallest increase occurring in those with baseline normal weight. Severely obese patients had the greatest increase in absolute BMI and fastest rate of rise in BMI during the pandemic (Fig. 1), representing ∼24 pounds gained during the study period. There were no differences in height change across weight categories, so increases in BMI were driven by changes in weight alone.
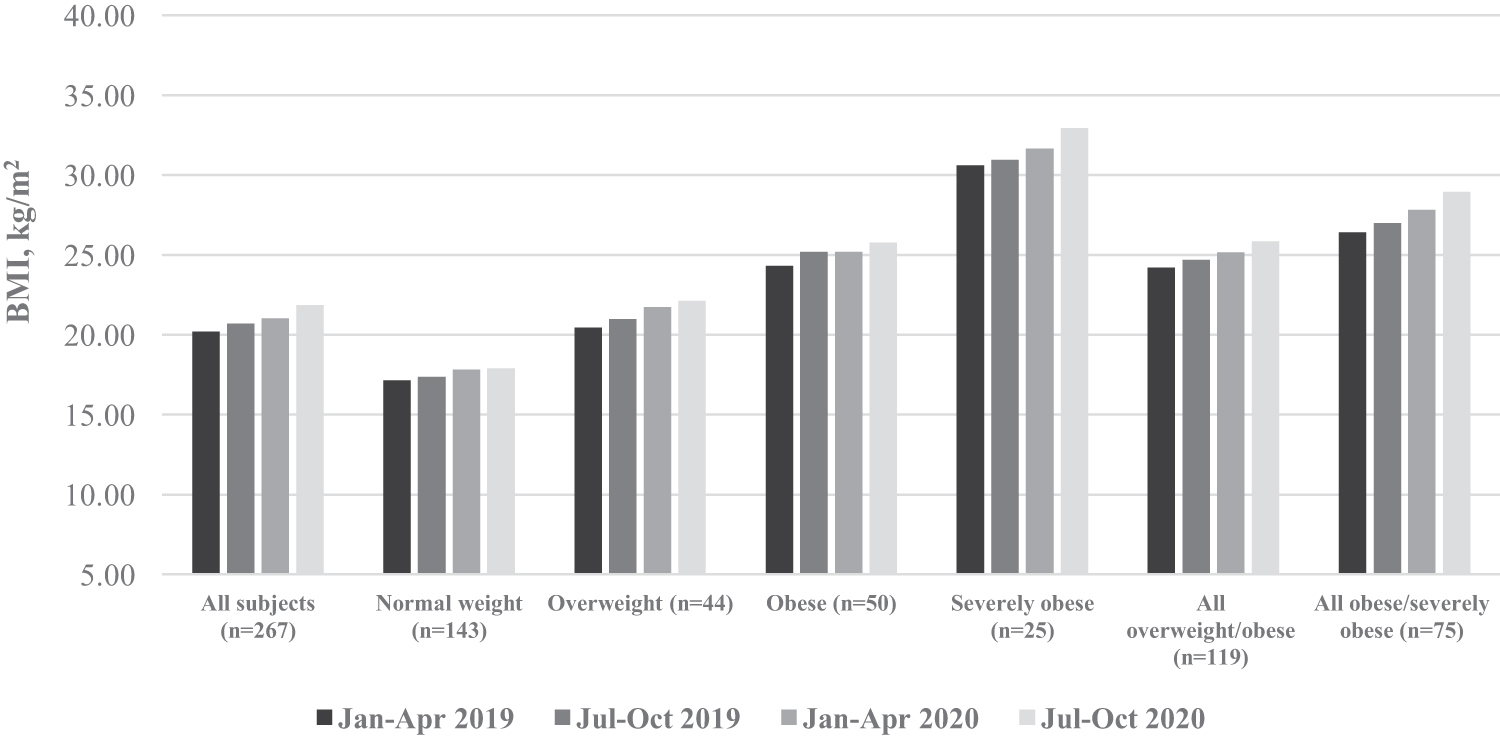
Change in BMI across weight categories over time. BMI, body mass index.
Hispanic patients had a greater increase in BMI rate of change (0.184 ± 0.285 kg/m2/month) during the pandemic relative to the year before (0.085 ± 0.139 kg/m2/month, P = 0.01) compared with non-Hispanic patients (0.083 ± 0.168 kg/m2/month versus 0.105 ± 0.278 kg/m2/month, P = 0.37). Children aged 6–11 years had a higher rate of BMI increase (0.086 ± 0.157 kg/m2/month in 2019 versus 0.147 kg/m2/month ±0.289 in 2020, P < 0.001), whereas children ≥12 years showed a decreased rate of BMI increase in the pandemic year (0.077 ± 0.169 mg/kg 2 /month in 2019 versus 0.052 mg/kg 2 /month in 2020, P = 0.002). Rate of change in BMI did not vary by sex, race, insurance type, or asthma severity.
Overall, there were fewer courses of systemic corticosteroids prescribed during the pandemic compared with the year before (47 versus 75, P = 0.005) with systemic steroid use being significantly more frequent in overweight and obese children compared with those with normal weight across all time periods.
Discussion
Several studies have shown increased obesity during the COVID-19 pandemic.14–16 A large pediatric cohort study by Lange et al. found the mean monthly rate of BMI increase nearly doubled in the first year of the pandemic compared with the year before. 14 We report on weight during the pandemic in children and adolescents with asthma.
The rate of BMI change increased significantly for children aged 6–11 years, while it slowed in adolescents with asthma. Other studies have also demonstrated greater increases in BMI in healthy school-aged children compared with adolescents.14–16 A Spanish study of teenagers after COVID-19–related confinement found a lower impact on VO2 max, an indicator of cardiorespiratory fitness, than would be expected after a period of decreased physical activity. 17 The authors speculated that increased compensatory health-related behaviors and increased outdoor physical activity immediately after the strict indoor confinement period may have mitigated the effects on cardiorespiratory fitness levels on their subjects. Data on physical activity or dietary patterns were not available for our study either, but similar factors may have mitigated weight gain in the adolescents in our study.
The relationship between obesity prevalence and socioeconomic factors is complex, and varies across subgroups.18,19 Studies have shown that summer weight gain patterns are more pronounced in Hispanic and African American children.2,19 Our study similarly found that Hispanic children with asthma gained weight at faster rates during the extended school closure compared with non-Hispanic patients. Our study did not find an effect of Black race on rate of BMI change, which may have been due to the limited sample size.
The greatest increase in BMI among our asthmatic population occurred in severely obese patients. Severe obesity is a growing pediatric problem, as recognized by several recent publications.20–22 Severely obese youth have markedly worse cardiometabolic profiles and health outcomes, and decreased effectiveness of traditional treatment approaches compared with those with overweight and obesity. 12 Although increasing BMI correlates with increasing asthma incidence, 7 there are limited data specifically on severely obese children with asthma.
Consistent with other studies, our subjects needed fewer courses of systemic corticosteroids during the early pandemic. Pediatric asthma exacerbations declined sharply after the start of the pandemic, and asthma-related health care utilization remained low throughout the fall of 2020.23–25 School closures, social distancing, and universal masking likely decreased community transmission of common respiratory viruses, thereby triggering fewer asthma exacerbations. The number of systemic corticosteroid courses prescribed throughout our study was consistently higher in overweight and obese patients compared with those with normal weight, reflecting a higher burden of asthma-related morbidity, as seen in other studies.8,9
Our study had several limitations. Due to its retrospective nature, a control group of healthy subjects with multiple visits documenting growth parameters was not available, as there were major disruptions to well-child care in the early part of the pandemic. 26 Still, the increased rate of BMI rise specifically in this high-risk group of children with asthma is an important and concerning trend to report. While we reported a marked overall increase in the rate of BMI change of ∼165% from the prepandemic year to the next, it is unknown how this is compared with prior national trends. Increases in annual prevalence of overweight and obesity over the past 2 decades have been well documented, 27 but monthly rates of BMI change have not been reported. Due to the retrospective design, data on physical activity, dietary patterns, and other potential covariables were not available.
Finally, patients seen exclusively by telehealth were excluded, which may have resulted in selection bias. Since obesity was identified early on as a risk factor for more severe COVID-19,28,29 overweight and obese patients may have been more likely to opt for virtual visits to avoid exposures. The same families may have avoided other activities outside the home as well, exacerbating risk factors for weight gain. Although exclusion of these patients is a limitation, it is unlikely to have affected the direction of the outcome, but rather to have led to an underestimation of BMI increase.
In this single-site, retrospective study of children and adolescents with asthma, there was a more rapid rate of BMI increase during the pandemic as compared with that observed in the previous year. Obesity is a risk factor for poor asthma control and for severe illness due to COVID-19, underscoring the importance of obesity management and prevention in this uniquely vulnerable group, particularly during future similar public health emergencies. Severely obese patients may be at heightened risk and warrant particularly close attention.
Footnotes
Acknowledgment
The authors acknowledge Zachary Messer, MPH, for his support in completing this work.
Authors' Contributions
C.K. designed conceptualization (lead); writing—original draft (lead); data collection (equal); formal analysis (supporting); review and editing (equal). S.K. contributed to conceptualization (supporting); formal analysis (lead); writing—review and editing (equal). J.J.W. and A.J.D. assisted with conceptualization (supporting); formal analysis (supporting); writing—review and editing (equal). K.F., S.D., and J.K. performed data collection (equal); writing—review and editing (supportive). S.K. conducted formal analysis (supporting); writing—review and editing (supportive). D.L.-A. contributed to conceptualization (supporting); writing—review and editing (equal).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.