
Abstract
Objective:
Mitigation of household allergens is associated with the reduction of asthma exacerbations in those with allergic asthma and is recommended in recent asthma guidelines. However, we need to better understand patient knowledge of aeroallergens in their homes prior to integrating direct allergen measurement methods into standard asthma care.
Methods:
We conducted a mixed-methods sequential pilot study consisting of a survey and virtual interview with caregivers of children aged 3 to 15 with asthma diagnosis (any severity) about asthma control, household environment, mitigation knowledge and strategies, and knowledge of allergens and asthma.
Results:
A total of 21 participants responded and 13 completed the virtual interview. Less than half identified mice (43%), rats (29%), and cockroaches (43%) as sources of allergens on the online survey, and no individuals mentioned these in discussions. Only 23% were able to define the term “allergen,” but 69% could list examples. There was a poor correlation between perceived asthma control (57% stated asthma control was good or excellent) compared to asthma that was classified as well controlled per Expert Panel Report 3 (EPR-3) guidelines (33% based on albuterol use and asthma symptoms). Finally, visual identification of mouse infestation was associated with active steps taken to mitigate mouse exposure (P = 0.007).
Conclusion:
Implementation of new Asthma Management Guidelines: Focused Updates 2020 by the National Institutes of Health will require additional aeroallergen education for individuals with asthma who do not recognize that cockroaches, rats, and mice can cause asthma symptoms, do not know the definition of an allergen, and do not correctly perceive asthma control status. Environmental assessment with education addressing these could hopefully decrease additional pharmaceutical needs.
Introduction
Asthma is a chronic disease that affects 5.8% of the pediatric population in the United States (US). 1 Asthma is a heterogeneous disease with multiple phenotypes and allergic asthma is considered the most common. 2 This recognition of allergic asthma was one aspect that was addressed in Asthma Management Guidelines: Focused Updates 2020 by the National Institutes of Health that addresses mitigation of allergen exposures, 3 that addresses mitigation of allergen exposures. An allergen is defined as a substance that can lead to an allergic reaction upon exposure. Reducing allergen exposure may improve asthma outcomes in patients with allergy symptoms and sensitization to indoor allergen exposures especially to dust mites, cockroaches, mice, animal dander, or mold as these allergens have a higher association with asthma mortality.3–5 Reduction of cockroach and dust mite allergens in the bed and bedroom floor can lead to decreased asthma morbidity (reduction of symptom days) during the year the intervention occurs as well as the year after intervention.6–9 Exposure to these allergens is common, and in the US alone, 14 million housing units reported seeing roaches in the past 12 months and 14.8 million saw rodents. 10 This number may be even higher, as a study found that 20% of homes without visual evidence had positive results of cockroach antigen levels in dust samples. 11 Thus, there is an under recognition of common household allergen exposures.
Patient perception of asthma control often has an overemphasis on pharmacological agents, but both medical management and environmental exposures contribute to asthma control. 12 Asthma control is defined by the Expert Panel Report (EPR-3) in three categories “well controlled”, “not well controlled”, and “very poorly controlled” based on criteria including frequency of asthma symptoms, nocturnal awakenings, β-2 agonist usage (albuterol), and oral steroid requirement. 13 Patients’ misperception that high albuterol use is associated with well controlled asthma is in line with shifts in how asthma has been conceptualized since the end of the Second World War. 14 During this period, asthma became increasingly defined not by environmental asthma triggers but by the alleviation of bronchoconstriction by inhaled pharmaceuticals such as inhaled corticosteroids or a combination of inhaled corticosteroids with long-acting β-agonist. 15 Albuterol use and perceived asthma control are often discordant, suggesting that the patient’s understanding of their symptoms that indicated poor control was just part of living with asthma. 12 Health literacy, particularly parental health literacy, has been shown to impact asthma outcomes.16,17 Lower parental health literacy is associated with increased emergency department (ED) visits, hospitalizations, and missed school days. 17 Improved education especially for allergic asthma patients with sensitization and exposure to the same allergens could be targeted for environmental interventions.18,19
Allergy exposure reduction as well as asthma education can be conducted by asthma home-based services, which are frequently utilized by hospital systems and have been associated with the improvement of asthma symptoms. 20 According to Sweet, et al., education by a public health nurse or health educator, providing cleaning supplies, and home interventions including mold or pest control can decrease asthma symptoms by decreasing mean asthma symptom days (5.1 to 2.6 days), nighttime awakenings (3.18 to 1.3 days), days with albuterol use (4.58 to 2.17 days), ED visits (1.17 to 0.5), and missed school days (6.24 to 2.81 days). 21 Multifactorial studies are more effective than single-intervention projects in reducing asthma morbidity.3,22–24 These multifactorial studies have been effective and despite increased cost, have demonstrated a positive return on investment. 21 Much of the cost is related to providing the same services to all homes. Asthma home-based services often provide allergen mitigation supplies to all patients including bedding, cleaning supplies, and HEPA vacuum and pest control if indicated, which contributes to cost. 25 To optimize utilization of limited resources, successful implementation of environmental management programs will require targeting interventions for patients who are sensitized and exposed.18,19
Implementation of the New Asthma Management Guidelines: Focused Updates 2020, 3 will require novel strategies for measuring allergens in homes and integrating results into patient care. Prior to this, we need a more thorough understanding of patients’ aeroallergen exposure, knowledge in relation to asthma control, and if they are willing to proceed with mitigation strategies. Finally, it is critical that patient perceptions of allergen measurement in their home are understood to reduce undesirable outcomes, such as feelings of shame or despair.26,27
The goal of this pilot study is to leverage a mixed-methods approach to assess the perspective of the parents of children with asthma regarding aeroallergen exposure in their homes and how it relates to asthma care. The work is designed to provide foundational information for future integration of allergen measurement into home-based asthma care.
Methods
Patients
Participants (n = 24) were recruited through the Asthma Express program at Nationwide Children’s Hospital Homecare and through the Nationwide Children’s Hospital Pulmonary Clinic in Columbus, OH, USA, between August 2021 and January 2023. The Asthma Express program serves families of children with moderate to severe asthma who have had at least one emergency room visit due to their asthma and provides in home education for allergens and asthma medications to these families. The pulmonary clinic serves a variety of patients with asthma that is difficult to control by first line asthma medications and interventions and is a referral-based service for primary care pediatricians. Inclusion criteria were physician diagnosis of asthma (any severity) for the child and child age between 3 and 15 years old. Exclusion criteria included non-English speaking, and if the parent had a cognitive impairment that might impact their ability to understand the benefits and risks of enrolling in the study they were evaluated by the Institutional Review Board (IRB) on a case-by-case basis.
Study design
We implemented a mixed-methods sequential explanatory study design to provide quantitative data and secondary qualitative nuance. 28 After obtaining online consent, we administered an online survey that was followed up with a qualitative interview via video conference. The online survey included questions about asthma control, allergen knowledge, mitigation knowledge, and strategies applied to the home of the child with asthma, as well as questions about the household environment. After the initial survey was completed, qualitative responses were obtained via a virtual interview with semi-structured questions about asthma, allergens, and mitigation strategies, as well as a discussion about parent perspectives on measuring allergens in the home. In these sections, questions were asked about asthma triggers, medications, as well as perceived control of asthma. Questions included past attempts at environmental allergen mitigation, environmental allergen concerns, and environmental allergen knowledge. We also asked for impressions of a home-based system allergen detection system if that was available. The study was approved by the Nationwide Children’s Hospital IRB (IRB MOD00011451).
Study end points
We completed a statistical analysis of the survey results with the goal to better define participants’ knowledge of household aeroallergens, asthma symptoms and control, and previous mitigation strategies. Data was summarized using frequency (percentage) for categorical variables. Well controlled versus not well controlled based on EPR-3 guidelines was calculated by answers to questions about asthma control. Reported asthma control was tested for associations with frequency of inhaler use, steps taken to remove home allergens, and well versus not well controlled based on EPR-3 guidelines via Fisher’s exact test.
Statistical analyses
Steps taken to remove allergens were tested for association with knowing the definition of “allergen” and listing examples of allergens, and finally, evidence of pests was tested for associations with steps taken to remove them as well as pest control were compared via Fisher’s exact test. McNemar’s chi-squared test for paired data was used to evaluate the difference in proportions of respondents selecting true and decoy allergen sources. Two-sided P-values < 0.05 were considered statistically significant. All statistical analyses were performed in R version 4.0 (R Core Team, Vienna, Austria) with reproducible programming in R Markdown.
The virtual interview was analyzed via somatic analysis. Qualitative data from the semi-structured interviews were manually grouped into themes and subthemes. Themes were identified by knowledge of allergens and actions taken based on concern for allergens as well as allergy testing performed. Participants were asked to define the term “allergen” and also to list examples of allergens. Answers were counted correct for the definition if they were similar to “substances that cause an allergic response,” but we accepted a wide range of similar definitions. For listing examples of allergens, we counted the answer correct if the participant named at least one substance known to cause an allergic response. The majority of answers counted as incorrect were the participant responding “I do not know” or similar. A saturation point was achieved in these qualitative interviews where no new information was revealed upon further interviews.
Results
A total of 24 online surveys were started with 21 surveys partially or fully completed and these were retained for analysis. There were 13 who were able to be contacted to complete the virtual interview and these were analyzed in the qualitative portion of the results. This is described in Supplementary Figure S1.
The characteristics of the child and parent of the participants are described in Table 1 and approximately half (n = 9) of the children in this study had allergy testing, with eight of the nine testing positive for at least one allergen. In more detail, the most common allergen source that families described was pets, but many also reported having dust allergies, food allergies, mold allergies, and one reported cockroach allergy. Two families mentioned, “too many to name here” and “see chart multiple items”. This study did not evaluate which allergens each patient was tested against or the type of allergen sensitization testing.
Characteristics of the Child and Parent of the Participants
n (%).
Definition of allergens and types of allergens
The survey then asked families to answer questions about allergens. Questions asked if participants could identify possible sources of allergens out of a list (Fig. 1). Of the 21 surveys, 100% of the surveyed participants did believe there were allergens in most homes.
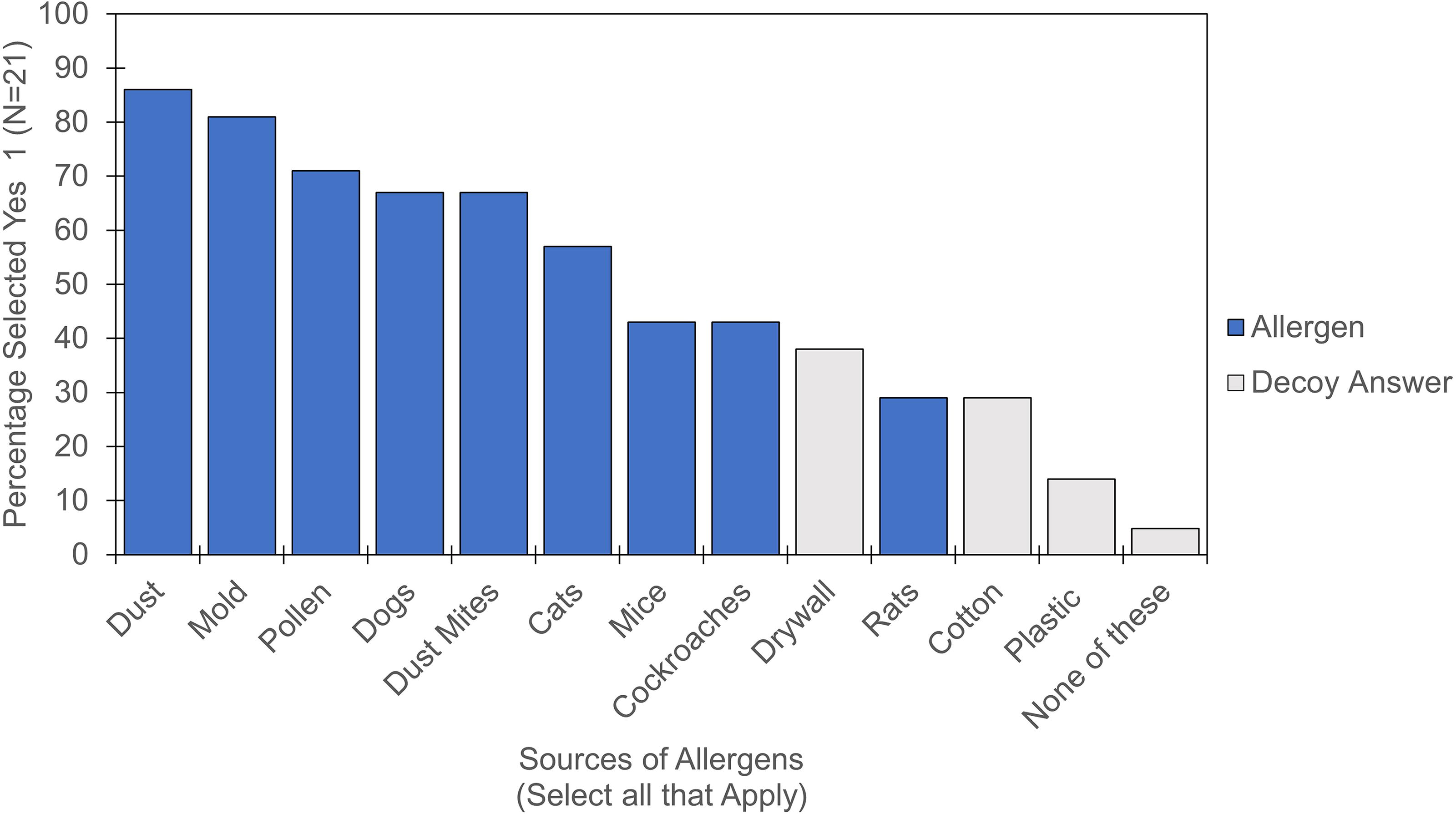
Participant identification of allergen sources. For the decoy answers, while components of these could be allergens, these were selected because they are common in the home and not commonly associated with allergy.
The most recognized allergens were dust (86%), mold (81%), pollen (71%), dog (67%), dust mites (67%), and cat (57%). Mice and cockroaches were only recognized by 43% of participants and rats were only recognized by 29% as a source of allergens, which is similar to the rates of selection for the decoy/incorrect answers (Fig. 1). A total of 52% of the participants answered yes to at least one of the decoy answers or selected “none of these.” The proportion of participants selecting at least one actual allergen among those listed in Supplementary Table S1 (95.2%, n = 20) was significantly different from the proportion selecting at least one decoy allergen (52.4%, n = 11) (P = 0.016), therefore true allergens were significantly more likely to be selected by a larger percentage of participants than incorrect responses (Wilcoxon rank-sum test, P = 0.013).
During the qualitative interview, only 23% of participants knew the definition of an allergen, but 69% could list examples of allergens. This list most often included dust, pollen, and food allergies, but no participant mentioned mice or cockroaches in this list of allergens during the qualitative interview. Of the participants who knew the definition of an allergen, all three had taken steps to remove allergens from their homes (Supplementary Table S1).
Albuterol use and perceived control of asthma
We asked about the family perception of asthma control using questions based on the EPR-3 guidelines, which include nocturnal symptoms, daytime coughing, frequency of inhaler use, and oral steroid need (Fig. 2a–d). 13

Asthma control questions and classification. 1Number included.
Asthma control is frequently measured by how often patients need their emergency inhaler, and out of the 21 surveys, 7 stated that their child used their inhaler daily (Fig. 2a). We found that 25% of patients who stated their asthma control was either excellent or good used their albuterol inhaler daily.
Based on participants answers, 33% were classified as well controlled based on the EPR-3 guidelines (Fig. 2d) compared with 57% who stated they believed their child’s asthma control was either good or excellent (Fig. 2c) as described in Supplementary Table S2.
Mitigation strategies
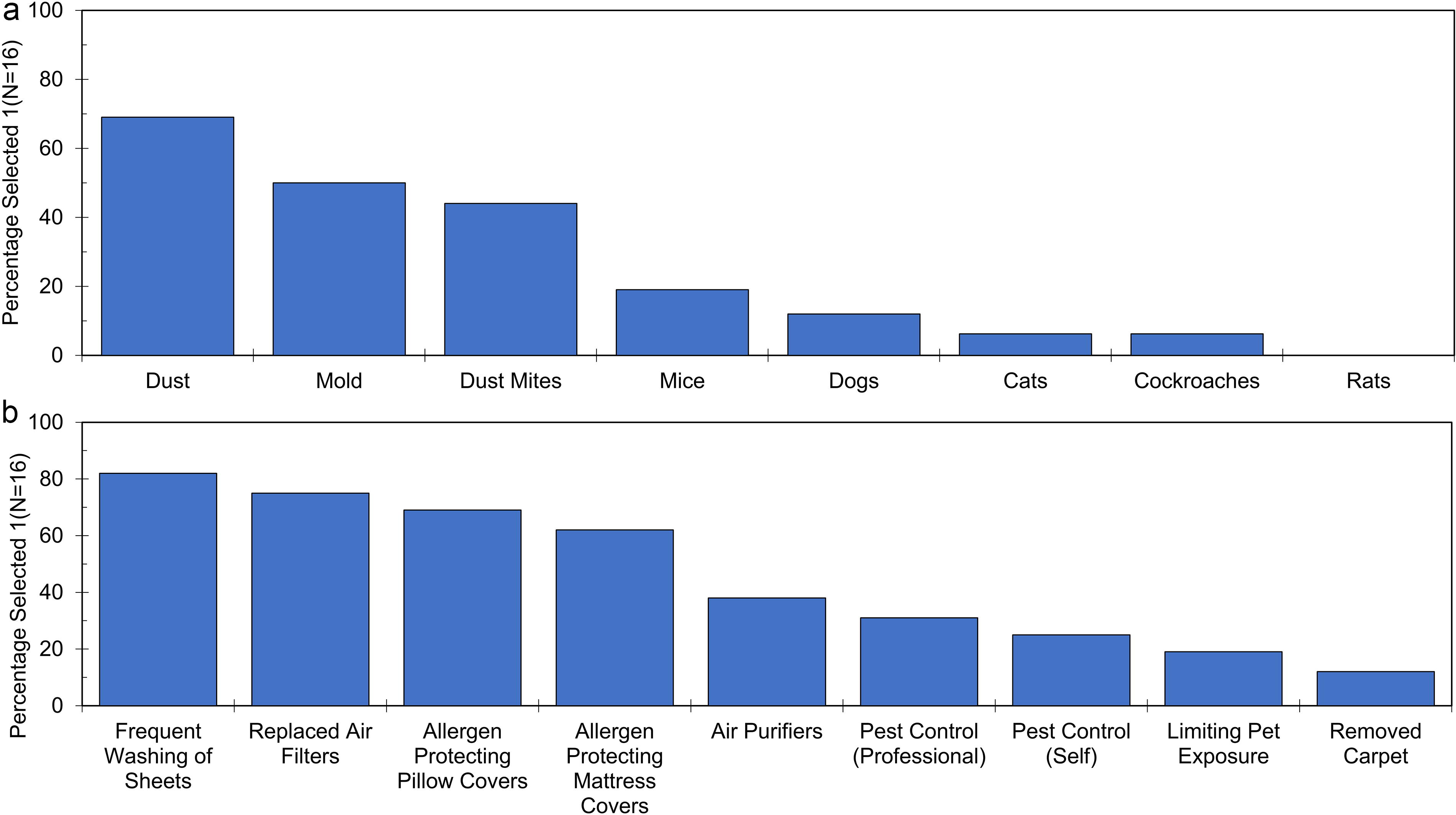
The survey then asked families to answer questions about allergen mitigation. If participants answered yes to removing allergens from their homes, they were prompted to answer what allergens they had mitigated and the steps that they had taken to remove these allergens (Table 2 and Fig. 3a and b).
Mitigation Strategies
When asked, 16 of 21 (76%) participants stated they had taken steps to decrease allergens in their home. Of the 16 that had stated they performed allergen mitigation; dust allergens were the most addressed. Typical mitigation strategies included frequently washing sheets, followed by replacing air filters, pillow covers, and mattress covers.
Only one participant had taken steps to remove cockroaches and three had attempted to remove mice. Eight participants had attempted pest control (either self or by a professional exterminator), which may have included other pests such as ants.
We explored the association between the visual identification of mice or rats in the home and the performing of mitigation and conducted the same comparison for cockroaches and mold (Table 3).
Association Between Allergen Presence and Mitigation Strategies
n (%).
Fisher’s exact test.
If families had identified mice or rat evidence in their home, 75% had taken steps to remove mice. One family mentioned they had cockroach evidence, and they had not taken steps to remove any allergens. There were four participants who stated they had evidence of water damage, leaks, or mold, and of these, three (75%) had taken steps to remove mold.
We also evaluated participants’ perceived concern about home allergens compared to whether the child had allergy testing and if they had taken steps to remove home allergens. Of these results, the majority (71%) of families had no to medium concern about home allergens (Table 2). If their child had allergy testing, their concern was lower as well with 77% having no to medium concern. Most families (76%) stated they had taken steps to remove allergens from their home, which indicates that most participants had low concern about home allergens but had already taken steps to remove home allergens.
Allergen detection in the home
Finally, participants showed interest in systems to detect allergens in their homes (Supplementary Table S3).
Overall, there was a positive response to having an in-home allergen detection system. Participants identified the ability to detect allergens in their home as “extremely important” (71%) and indicated the “extreme importance” of education regarding allergens (52%) and allergen mitigation (71%). All participants indicated at least some interest in a mobile app for allergen measurement. Discussions revealed interest in mitigation strategies, evaluation upon moving and helping with landlord-tenant issues. Some representative quotes from those interviews were “if you knew this room had a lot of dust allergens, then we would change the carpet”, “it would be beneficial for situations such as mine where if you are going to re-locate, you would know what is present”, and finally another participant stated, it could help the “landlord have to get better and put themselves in their shoes.” This interest suggests that families are interested in methods to measure allergens in the home.
Discussion
Implementation of the most recent Asthma Management Guidelines: Focused Updated 2020, 3 will require aeroallergen mitigation strategies to be integrated into clinical care for patients with allergic asthma who are both sensitized and exposed to an allergen. Here, we provide foundational information regarding patient perceptions of allergens in their homes that will be necessary to understand how allergen measurement in homes will impact this population. We demonstrated that only 3 of 13 participants could define an allergen, which indicates that additional patient education may be required. In addition, patients often misunderstood the goal of asthma control as the use of inhalers, instead of the reduction of symptoms. Patients also indicated a willingness to conduct allergen mitigation that might be necessary as demonstrated by past efforts. Finally, participants also expressed enthusiasm for novel methods to measure allergens in their homes. These factors have important implications for clinical practice.
Patient education regarding aeroallergens is necessary
Less than half of the participants could define an allergen or correctly select cockroaches or mice as allergens, which are the most common household allergens associated with poor asthma outcomes.9,29 This suggests clinicians should consider implementing additional aeroallergen education practices to ensure patients understand the relation of allergen exposure to asthma symptoms. Clinicians might also focus efforts on education regarding the most common household allergens (mice and cockroaches) associated with poor asthma control. This suggests knowledge of allergens, especially household allergens, may lead to stronger implementation of mitigation strategies. In addition, the measurement of allergens in the home presents a crucial opportunity to educate patients about their exposures. Patients may also desire this knowledge, as a participant stated, “I can’t think of anything else I could do to remove allergens from our home.”
Patients have misperceptions about the control of asthma
Control of asthma is classified by the EPR-3 guidelines based on asthma symptoms as well as albuterol use. 13 Many participants who perceived their asthma to be well controlled were classified as poorly controlled based on EPR-3 due to frequent inhaler use. This is in the setting of patients recruited from both pulmonary clinics and the Asthma Express program, both of which help with education of asthma and allergies, as well as, a majority being followed by an allergist or pulmonologist. As we know health literacy significantly impacts asthma control, 16 and therefore with patients that already have increased education about their asthma, there is still a disconnect between their perceived and actual asthma control. This has previously been described in qualitative studies, 12 with the continued perception that pharmacological management is central to asthma control. With a diminished emphasis on environmental triggers, both culturally and clinically,14,15 it is easy to understand why patients associated high pharmaceutical use with proper control and found difficulty in identifying indoor allergy triggers. Inaccurate assessment of asthma control could lead to delayed or inappropriate treatment as well as an increase in asthma exacerbations. This suggests that there is a continued need for education and improved perception of asthma symptom control by patients even in these instances when they are receiving education through home-based programs.
Known exposures led to mitigation for mice
Common household allergens of dust mites, cockroaches, and mice are found in many homes, 10 and mitigation of these allergens is associated with better asthma outcomes.18,19 There is limited data if visual versus measured allergen particles in homes that lead to different mitigation strategies, but measured analysis has higher rates of positive exposure compared to visual analysis of common household allergens. 11 Upon discussion with participants, the direct knowledge of allergens present resulted in allergen mitigation as shown with participants who had known mice exposure which had a significant, positive association with mice mitigation.
Implementation of new asthma guidelines
According to the updated asthma guidelines, 3 mitigation of aeroallergens will be critical to integrate into asthma care for patients who have both exposure and positive sensitization. According to the 2024 GINA Guidelines, multicomponent strategies are necessary to address indoor allergen exposures as opposed to single interventions. 30 The fact that the most effective interventions utilize a multicomponent strategy can increase the cost. An accessible means of assessing indoor allergens could help allocate limited resources to the most effective interventions, 25 and provide an important and necessary opportunity for patient education. Patient recognition of the presence and importance of household allergens could then lead to improved implementation of mitigation strategies and ultimately improved asthma control.
Limitations
This mixed-methods study was designed to gather initial data on patient knowledge and perceptions regarding aeroallergens to serve as a foundation for future indoor allergen measurements. The study has a small sample size (n = 21) and may be under-powered to detect significant associations. Most of the participants were recruited from the Asthma Express program, where health literacy is already being addressed, which could lead to improved knowledge of mitigation, actions for allergen mitigation, and asthma control. Standard limitations to qualitative research interviews also apply. For instance, our qualitative research phase was asked via open-ended questions and therefore the patients recruited could interpret these questions differently leading to different answers. This also applies to the quantitative survey with phrasing of questions and ability to interpret questions in different ways including daily inhaler use (such as albuterol versus their daily controller). Associations between the ability to define the term allergen and education level can be evaluated in studies with larger sample sizes. The participants in this population were young (45% were 5 or under) and geographically limited to those in or near Columbus, OH, USA, which limits the generalizability of results. We did not have access to information on the family history of allergic disease.
Conclusion
This study demonstrates that education on household aeroallergens, asthma, and allergen mitigation will be necessary to support the implementation of Asthma Management Guidelines: Focused Updated 2020, 3 regarding aeroallergen control. This study suggests that there continues to be a lack of education regarding common household allergens (cockroaches, mice, and rats). Education is also still needed in the control of asthma as a perception of asthma control can vary greatly from symptoms. In the future, improved allergen measurement in the home coupled with aeroallergen education could ultimately lead to improved asthma control without additional pharmacologic interventions.
Footnotes
Acknowledgements
We are grateful to the clinicians in the Asthma Express program and in the Pulmonary Clinic at Nationwide Children’s Hospital who assisted with recruitment. We are also tremendously appreciative of the families for their participation in the study.
Authors’ Contributions
K.C.D., M.P., C.T., P.S., B.Y. and N.S. contributed to study design. C.T., P.S., E.B., and B.Y. conducted participant recruitment. B.Y., J.P., and K.D. performed virtual interviews. J.P., K.D., and B.Y. maintained the database. M.E. performed statistical analysis. B.Y., N.S., and K.D. wrote the manuscript. All authors edited the manuscript and approved prior to submission.
Author Disclosure Statement
Some of the authors have submitted a patent application for a novel method to detect allergens in homes.
Funding Information
This work was supported by grant HHHU0057-20 from the Department of Housing and Urban Development.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.