
Abstract
Background:
Biological agents are considered important therapies and are increasingly used in the treatment of a range of rheumatological and inflammatory diseases. Nevertheless, the prevalent use of these treatments has been associated with increased incidence of drug-induced hypersensitivity reactions (HSR).
Case Presentation:
A 15-year-old patient with enthesitis-related arthritis developed late HSR after the use of adalimumab. Consequently, etanercept was used as an alternative treatment. Etanercept was administered subcutaneously through a single dose without any reaction upon examination using skin tests (skin prick test, intradermal test, and patch test) against likely cross-reactions given that both adalimumab and etanercept were anti-tumor necrosis factor (TNF) agents.
Conclusions:
Currently, TNF-α inhibitors find widespread use. Caution is required against HSR reactions, including systemic or local injection site reactions, although they are generally considered safe to use.
Introduction
Tumor necrosis factor-α (TNF-α) is one of the main mediators of inflammation. TNF-α stimulates proinflammatory interleukins, increases leukocyte migration, activates neutrophils and eosinophils, and stimulates acute phase reactions. Therefore, TNF-α inhibitors are frequently used in the treatment of chronic rheumatic and inflammatory diseases, including rheumatoid arthritis, enthesitis-related arthritis, and ulcerative colitis, as they can prevent the activation of this cytokines. 1
As a fully human IgG1 monoclonal antibody that inhibits TNF-α, adalimumab is one of the most frequently used anti-TNF agents. 2 Etanercept (ETN) is a recombinant protein formed through the fusion of the ligand-binding portion of the TNF-α receptor to the fragment crystallizable (Fc) portion of IgG and mainly binds to the soluble form of TNF-α. ETN is also considered the only TNF-α inhibitor that blocks lymphotoxin-α. Injection site reactions frequently occur with these agents, and it was reported that they might also cause systemic hypersensitivity reactions (HSR).3–5 Increased use of this treatment option is associated with increased prevalence of adverse drug reactions.6,7 These adverse reactions may limit the use of biologics, interrupting effective treatment and leading to deteriorated quality of life.
Current HSRs associated with biological agents are classified as infusion-related reactions, cytokine release reactions, type I (IgE/non-IgE), late-type III and IV, and mixed reactions. 8 Clinical manifestations of HSRs can be mild, severe, or even life-threatening. Late HSRs can occur days to months after exposure to the agent. 9
This report aimed to share our case on enthesitis-related arthritis. The patient developed a late reaction to adalimumab and received etanercept treatment, which was successfully used as an alternative treatment.
Case Presentation
A 15-year-old boy presented to the Pediatric Rheumatology clinic with complaints of hip pain and morning stiffness, which started 8 months ago. Upon examination, bilateral sacroiliitis was identified, and consequently, he was diagnosed with enthesitis-related arthritis (EIA). It was understood that the patient, who had a history of preterm birth, was operated on twice at the ages of 5 and 13 years for congenitally corrected transposition of the great vessels and continued to take acetylsalicylic acid (2.7 mg/kg/day), furosemide (0.8 mg/kg/day every other day), spironolactone (0.45 mg/kg/day), and digoxin (0.0045 mg/kg/day) treatments for years without any problems. Due to no response to nonsteroidal anti-inflammatory drugs, sulfasalazine (18 mg/kg/day) treatment for EIA was started in the 3rd month of the treatment. Urticarial edema of the left ear and maculopapular rash on the skin occurred 7–8 h after oral intake (sulfasalazine) during the second week of drug treatment. The patient had no comorbid symptoms, and his complaints resolved within 3 days after a single dose of antihistamine.
Treatment was changed to methotrexate (MTX) because of a suspected allergic reaction and failure to resolve clinical complaints associated with EIA. Eleven doses of subcutaneous (SC) MTX (MEKSRATU 15 mg/0.6 mL-once a week) were regularly administered. The patient’s complaints of nausea and abdominal pain gradually increased during treatment, and his treatment was replaced with adalimumab because of drug intolerance. Gastric complaints regressed and did not recur after MTX was discontinued. Subsequently, SC adalimumab (HUMIRA PEN 40 mg/0.4 mL once in 2 weeks) alternative treatment was started. On Day 12 of the first dose of this drug, the patient presented with the rash all over the body. Subsequently, the patient was thoroughly examined. In addition, his vital signs were stable. The skin had generalized maculopapular eczema on the body that faded with pressure, generalized maculopapular eczema on the extremities that did not fade with pressure, and a 10 × 11 cm diameter hyperemic plaque at the injection site. There was no accompanying mucosal involvement, bullae, and vesicles along with the rash (Fig. 1). Other systemic examination was normal. There were no pathological features in the hemogram, biochemical parameters, complement levels, and urine microscopy. Adalimumab treatment was discontinued because of the reactions suggesting late-type maculopapular exanthema (MPE). The lesions regressed upon antihistamine treatment, and marked regression was seen within 4 days.
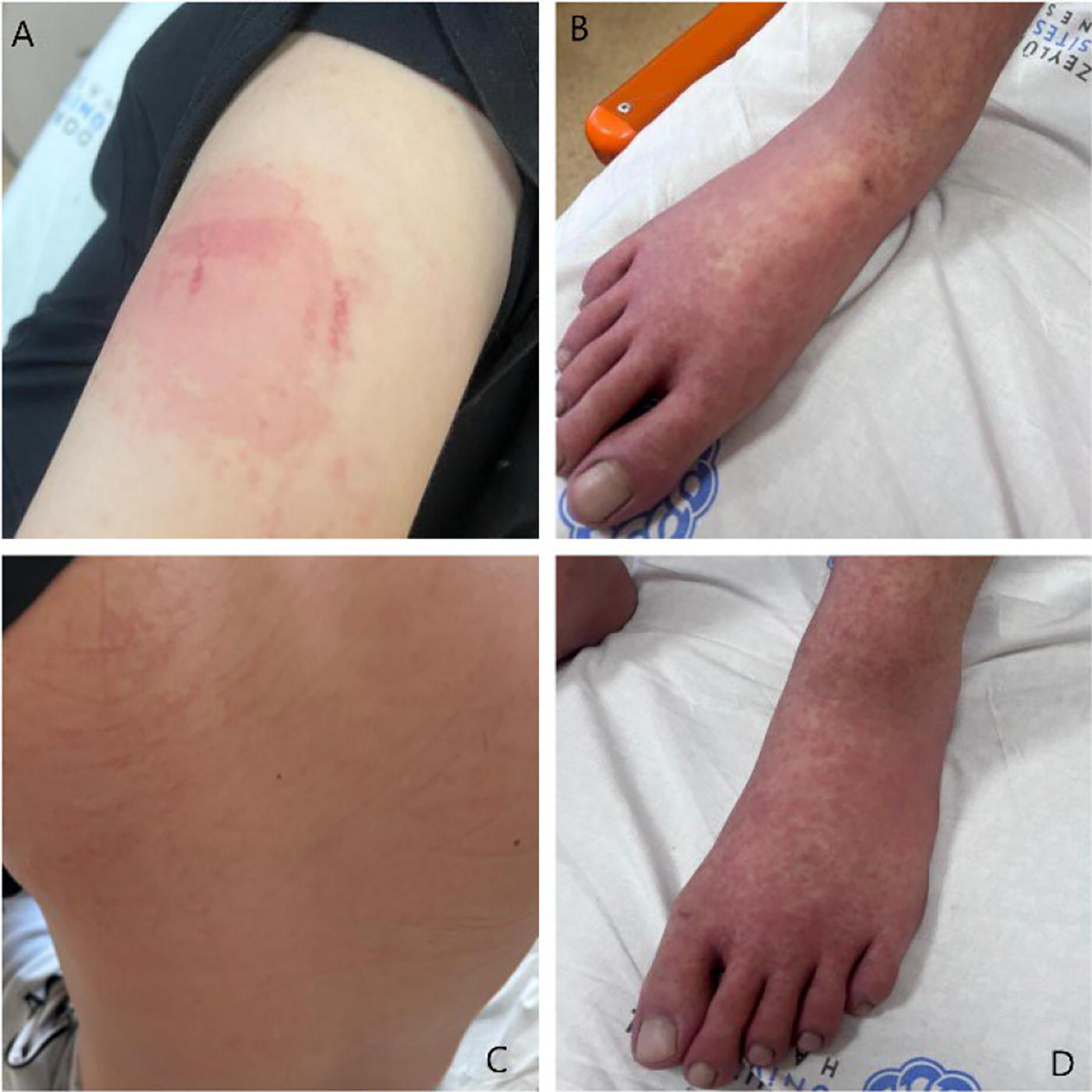
Reactions associated with adalimumab treatment.
Upon detailed examination of the patient and collection of informed consent from the patient’s parents, a skin prick test (SPT) for adalimumab at a concentration of 50 mg/mL and dilutions of 1:100 and 1:10, an intradermal test (IDT) with 0.02 mL of each solution, and a patch test (IQ Patch test units) with a concentration of 50 mg/mL were performed sequentially 4 weeks later (Table 1). Patch tests were examined for delayed reaction at 48 and 72 h. There was no early or late reaction in SPT, IDTs, and patch test.
Test Concentrations of Drugs
SPT, skin prick test; IDT, intradermal test.
The Pediatric Rheumatology clinic was reinterviewed for adalimumab use and possible risks. Etanercept treatment was scheduled as an alternative treatment. Allergy tests against etanercept were scheduled to predict likely reactions.
Three weeks after adalimumab tests, SPT was performed against etanercept (Embrel®) at a concentration of 50 mg/mL, and IDT with 0.02 mL of each solution, sequentially with dilutions of 1:100 and 1:10. Histamine and saline were used as positive and negative controls. Then the asymptomatic patient was discharged after 4 h of observation following the last IDT. In addition, at 48 and 72 h, the patient was checked for late reaction. However, no reaction was observed (Table 1).
One week after the tests, 50 mg etanercept was administered SC in a single dose under observation. The patient was discharged after 4 h of observation without any reaction, and no late reaction was observed during the follow-up. Our patient has continued weekly etanercept treatment for 2 months without any problems. (The parents gave permission for all procedures. Written permission was given by parents with minor assent for publication of this case study.)
Discussion
Biological agents are considered important therapeutic treatments for a variety of rheumatological diseases and find increased use in clinical practice. The incidence of HSRs has also increased with increased use of these treatment modalities. 9
The most prevalent side effect for adalimumab is the injection site reactions, with an incidence ranging between 3.2% and 20%. 10 Serum-like disease, maculopapular rash, leukocytoclastic vasculitis, acute generalized exanthematous pustulosis, drug reaction with systemic symptoms of eosinophilia, Stevens-Johnson syndrome, and toxic epidermal necrolysis have been reported among moderate to severe immune-mediated reactions. Late HSRs typically occur within 14 days of drug administration.9,11
In our case, a late-type reaction associated with adalimumab was considered because of the rash in the form of MPE on the body accompanied by a large local reaction at the injection site on day 12 after the initial administration, the absence of additional suspicious agents, and no change in terms of laboratory parameters and rash during the follow-up period.
There is only a limited data in the literature on in vivo allergy testing for late HSRs with biological agents. Most of this data is at the level of recommendation. It is not possible to completely exclude drug-related allergies using available tests. Nevertheless, these tests are recommended even with their low sensitivity and specificity. 9 Therefore, we planned SPT, IDT (early and late reading), and patch tests against adalimumab in our patient. However, based on the tests, no reaction was observed. Nevertheless, adalimumab treatment was changed to etanercept treatment upon decision with the Family and Pediatric Rheumatology clinic. Skin tests were performed for early and late examination before etanercept administration, considering that both biological agents belonged to the anti-TNF drug group. Based on the test results, the risk of cross-reaction was negative. Moreover, early clinical and radiological remission responses can be achieved with etanercept in inflammatory diseases. Advanced pharmacogenetic studies are being conducted to predict clinical responses. These studies aim to identify which patients are likely to respond more effectively to specific drug classes, thereby reducing the risk of potential adverse effects. 12 Unfortunately, detailed studies on this subject are not feasible in our clinic. Another anti-TNF agent used in the pediatric population is infliximab; however, it was not preferred due to the higher risk of infusion reactions and anaphylaxis, as well as the need for intravenous administration. Etanercept was preferred because of its short half-life, SC administration, and ease of patient adherence. 13
Cases of HSRs associated with anti-TNF agents have been reported previously. Typically, early reactions were reported with these agents.14–16 Quercia et al. reported on a 50-year-old woman with rheumatoid arthritis, who developed anaphylaxis after adalimumab use and continued to receive the treatment upon successful desensitization, indicated by negative skin tests. 14 Bavbek et al. successfully performed desensitization against the responsible drug in a patient with early injection site reaction associated with adalimumab. In a 2015 case series, 12 patients who reported systemic early and late reactions with adalimumab and etanercept underwent rapid SC desensitization with both drugs. 14 A recent case report stated that a 46-year-old woman underwent a successful graded challenge with adalimumab after a late reaction to golimumab. 17
After etanercept tests, our patient, who was considered to have a low-risk reaction, took the drug in a single administration without any problems, and the weekly administration of 50 mg/dose SC continued without any reaction.
To the best of our knowledge, our report is the first pediatric case report in which etanercept treatment was successfully administered under the guidance of diagnostic skin tests in a low-risk case with a history of late reaction to adalimumab. In conclusion, TNF-α inhibitors are frequently used in the treatment of chronic rheumatic and inflammatory diseases. They are typically well tolerated; however, caution is required as there is a risk of HSR, including systemic or local injection site reactions.
Footnotes
Authors’ Contributions
H.Y. and Ö.A. made substantial contributions to the conception and design of the study, drafted the study, and revised it critically for important intellectual content and gave the final approval of the version to be published; D.B.B., G.K., T.A., R.T., and N.U. made substantial contributions to the acquisition, analysis, and interpretation of data, drafted the study, and revised it critically for important intellectual content and gave the final approval of the version to be published; all authors approved the final version of the article as submitted and agreed to be accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved.
Ethical Approval and Trial Registration
The case description was performed following the ethical standards as laid down in the Declaration of Helsinki and its later amendments.
Consent for Publication
Written informed consent was obtained from the child’s parents for all procedures performed and for publication. (Since our patient was under 18 years of age, permission was obtained from his legal guardian).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.