
Abstract
Phage-antibiotic synergy (PAS) has been extensively explored over the past decade, with the aim of developing more effective treatments against multidrug-resistant organisms. However, it remains unclear how to effectively combine these two approaches. To address this uncertainty, we assessed four main aspects of PAS interactions in this review, seeking to identify commonalities of combining treatments within and between bacterial species. We examined all literature on PAS efficacy toward ESKAPE pathogens and present an analysis of the data in papers focusing on: (1) order of treatment, (2) dose of both phage and antibiotics, (3) mechanism of action, and (4) viability of transfer from in vivo or animal model trials to clinical applications. Our analysis indicates that there is little consistency within phage-antibiotic therapy regimens, suggesting that highly individualized treatment regimens should be used. We propose a set of experimental studies to address these research gaps. We end our review with suggestions on how to improve studies on phage-antibiotic combination therapy to advance this field.
Introduction
The decline in the efficacy of antimicrobials against pathogens is of increasing public concern. 1 Moreover, the emergence of Multi-Drug Resistant Organisms (MDROs) presents increasing challenges to health care systems worldwide. The MDROs are classed as pathogens that exhibit resistance to at least one antimicrobial agent in three or more antibiotic classes. Infections caused by MDROs have limited viable treatment options, as known antimicrobials fail to work.
Of particular concern are bacteria belonging to the ESKAPE group: pathogens notorious for infections that are resistant to many antimicrobial agents.2–5 Included are the Gram-positive Enterococcus faecium and Staphylococcus aureus and four Gram-negative pathogens: Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp.
The Global Antimicrobial Resistance and Use Surveillance System (GLASS) 2022 report and the Philippine Antimicrobial Resistance Surveillance Program (ARSP) report increased resistance rates within numerous bacteria, including those from the ESKAPE group, enlisting these as critical pathogens in need of new antibiotics. 6
The broad and expansive use of current antimicrobials in health care and medical settings further stimulates the development of MDROs that primarily target patients with weakened immune systems or those with acute illnesses. Indeed, infections caused by these bacteria result in higher morbidity and mortality among immunocompromised and increase the risk of Hospital-Acquired Infections (HAIs) through patient exposure and medical equipment contamination.7–11 Low- and lower middle-income countries (L-LMIC) are particularly susceptible to MDROs.
A systematic review on ESKAPE pathogens by Ayobami et al. emphasized that although antimicrobial resistance (AMR) is an overarching global challenge, there is a disparity in terms of effects in countries, especially L-LMICs. The burden of the continued rise of multidrug-resistant (MDR) in bacterial pathogens is coupled with the slow development of new drugs and the unmet necessity for alternative interventions. With limited resources and increased risk in HAIs, it is not only critical to increase the surveillance of MDROs, but also critical to urgently seek out alternative treatments to known antimicrobials. 12
Bacteriophage as Alternative Treatments for ESKAPE-Induced Infections
Several options are currently being explored, particularly the use of bacterial viruses, or bacteriophages (phages), as a viable treatment modality. Phages are highly host-specific, targeting only bacterial species or subspecies that they kill by lysing the cells.13–15 In addition to their specificity, they are also self-limiting and self-replicating, have low-inherent toxicity, and do not disrupt the host's microbiota (compared with known broad-spectrum agents).
Studies on the use of phages have demonstrated effectiveness against MDR bacteria generally isolated from medical facilities.15,16 They can also disrupt biofilms of target bacteria that are commonly found and may prominently increase antibiotic resistance.17–20 Phages can be used as a treatment either as a monotherapy or in cocktails. Phage monotherapy, as the name implies, uses one phage isolate, whereas cocktail formulations use two or more phages.
The problem with monotherapy is that it presents a single source of selective pressure driving evolution, which, paradoxically, might also be considered an advantage. Molecular gene pleiotropy, where a change in a single gene may affect multiple traits, can result in either trade-off or trade-up mutations. Thus, utilizing monotherapy might be a preferable strategy. 21
Bacteria develop resistance to both antibiotics and phages, although less competently to the latter, as phages can also evolve alongside their hosts, rendering the relationship more complex. Phage cocktail formulations are commonly preferred during therapeutic applications to mitigate resistance.
It is evident that, in addition to using antibiotics or phages individually, combinations of both could be employed, a concept that several researchers and doctors have explored. To navigate this field, we examined all papers published from 2011 to 2021 that involved the study of ESKAPE pathogens in relation to phage-antibiotic combinations (Fig. 1).
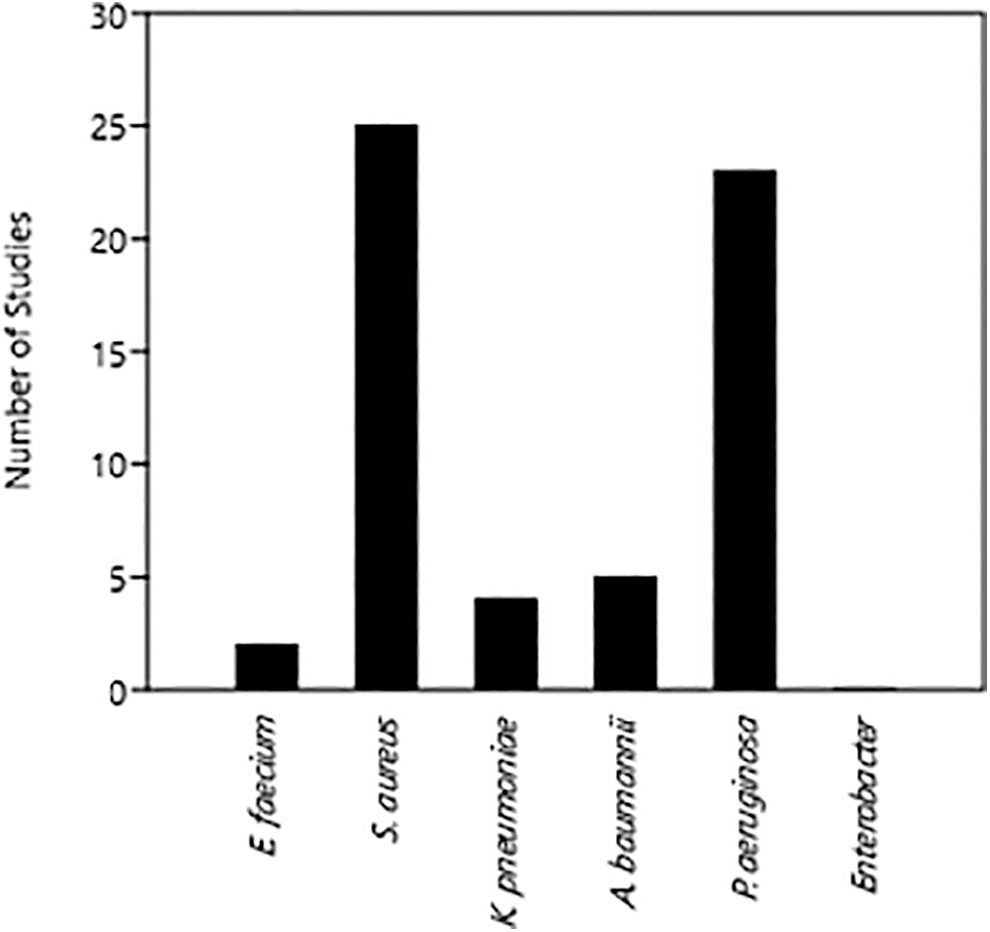
Distribution of studies that tackled each of the ESKAPE pathogens.
Phage-Antibiotic Combinations: Synergism or Antagonism?
The rationale for exploring combinatorial phage-antibiotic therapy stems from observations that combinations of these entities are superior to the use of either antibacterial agent alone. 22 The first interactions between the two microbial agents were observed by Comeau et al., who demonstrated that enhanced phage production and replication were observed when combined with beta-lactams and quinolones.
The interactions in their study induced an increase in plaque size, which they attributed to the intrinsic characteristics of the phage, as well as extrinsic factors such as temperature, bacterial density, and incubation period. According to Comeau et al., these interactions were most likely due to the combination of phages and antibiotics, which altered the interaction between the phage and the bacterial host—specifically altering the adsorption rate of the phage to the host, and the burst size of the phage. 23
This phenomenon is referred to as Phage-Antibiotic Synergy (PAS), whereby the combination of treatments results in enhanced bacterial eradication as compared with using only one treatment. 22 Further studies observed similar results, significantly showing the importance of synergism to drastically improve bacterial inhibitions and prevent the emergence of resistant strains using phage-antibiotic co-treatments.11,24–26
Combination therapy can also result in antagonistic interactions. These are less common than synergistic interactions but still more prevalent than “neutral” interactions. 27 Further, some combinations might be detrimental for the host due to the stimulation of virulence genes. 28 This underscores that PAS combinations should be carefully selected.
For this review, we categorized PAS into synergistic, neutral, and antagonistic interactions. A synergistic effect is defined as an increase in bactericidal effects observed when using both agents compared with using a single antibacterial agent alone; neutral when no change in bactericidal effect occurs using both agents; and antagonistic when fewer bactericidal effects are observed.27,29
In this review, we examine four components of phage-antibiotic combination therapy, namely (1) order of administration, (2) antimicrobial drug dosage, (3) mechanism of action, and (4) viability of transfer from in vivo trials to clinical applications (Fig. 2). A critical examination of this literature leads us to suggest the sustainability and efficacy of using both phages and antibiotics in MDRO infections, as well as considering other factors that may affect the resulting PAS interactions.
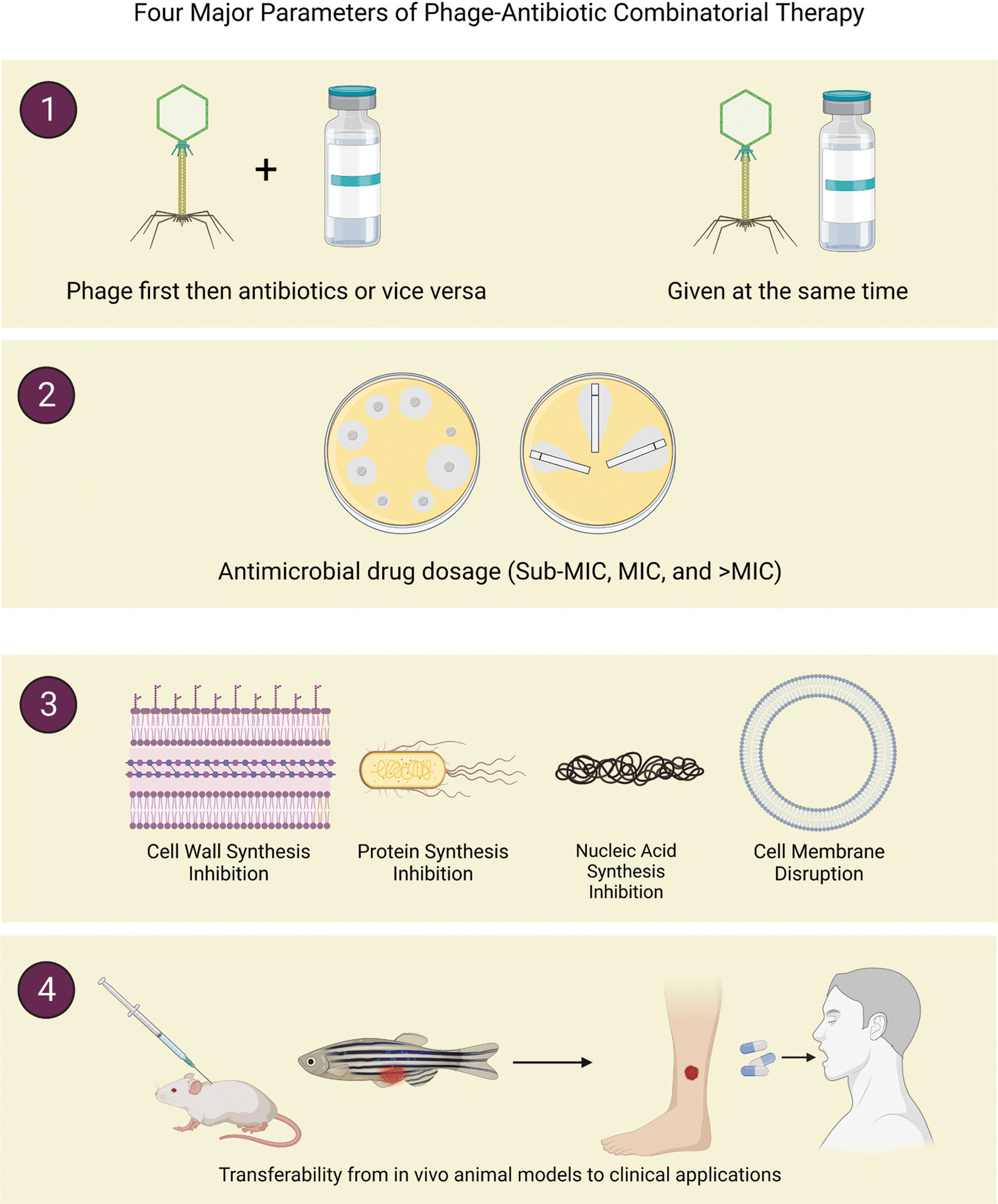
Four major parameters of phage-antibiotic combinatorial therapy. Created with BioRender.com. Agreement numbers MF255AG8OG and NZ255AGHKJ.
We highlight gaps and inconsistencies in previous work that make data difficult to compare. Our review concludes with a proposed framework where data could be collected systematically to benefit the medical field with a solution that could assist in alleviating and mitigating MDROs.
On the order of administration
In combination treatments, one factor that should be considered is the timing and interval of administration, as these can affect the outcome and the efficacy of the combinatorial treatment employed. In simultaneous therapy, the antibiotics and the phages are administered on the subject at the same time, whereas a sequential or staggered regimen entails that antibiotics and phages are applied at different points in time, with a significant time interval between the two treatments.
The possible change in the interactions of both antimicrobial agents provided another aspect that should be considered in combination therapies, which is evident in the increase of studies focusing on testing both simultaneous and sequential treatments rather than simultaneous administration alone (Fig. 3).
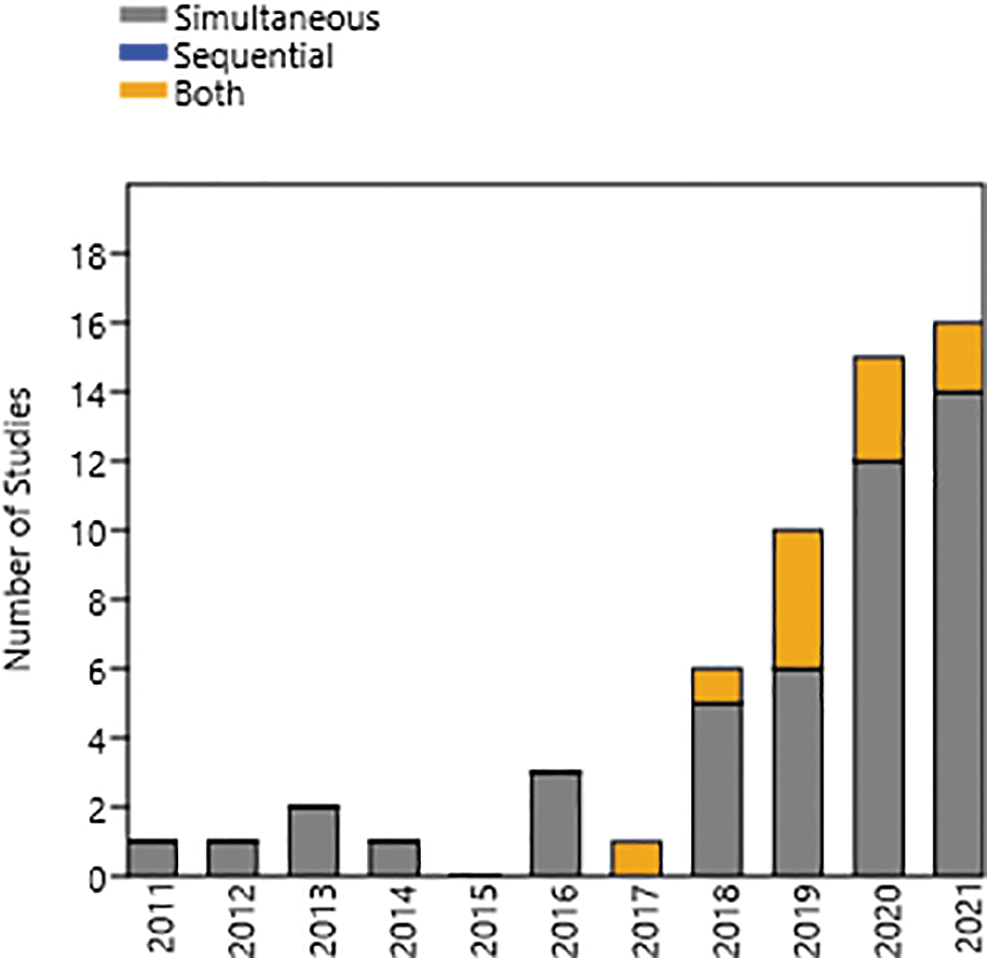
Distribution of studies published in 10 years, each showing those that used only simultaneous or sequential application strategies, or both.
Examples of comparison between timing and administration are shown in Table 1, wherein the order of treatment was tested by both Dickey and Perrot, and Berryhill et al.30,31 In addition, Torres-Barceló et al. tested various intervals for the sequential administration of phages and antibiotics (0, 12, and 24 h). 32
Comparison of Simultaneous Versus Sequential Administration
CIP, ciprofloxacin; DAP, daptomycin; ERM, erythromycin; GEN, gentamycin; KAN, kanamycin; LIN, linezolid; OXA, oxacillin; PYO, pyophages; RIF, rifampin; STM, streptomycin; TET, tetracycline; VAN, vancomycin.
Neutral and antagonistic interactions observed on simultaneous application likely stem from a concurrent bactericidal effect of both agents—wherein the bacterial population decreases before both agents were able to take full effect against the targeted host, thus removing the advantage of employing combinatory treatments. The efficacy of sequential administration of treatments, therefore, can be attributed to population dynamics.
True to its nature as viruses, bacteriophages are only able to continue to infect and lyse effectively through the presence of a susceptible host. Pre-exposure to phages, as performed in the studies outlined in Table 1, allowed successful infection and replication of phages against an abundance of the targeted host without the interference of antibiotics. Subsequently, the delayed administration of the antibiotics provides a second source of bactericidal action, thus more effectively killing the bacteria.31,33,34
In relation to the time delay between the treatments, Berryhill et al. stated that antibiotics would be best administered with 6–12 h delay from the phage pre-treatment. 31 In addition, 12 h intervals between treatments showed the most synergistic interactions based on the study by Torres-Barceló et al. The indicated time interval was not explained in the studies but can be related to the phage-host interaction and phage infection kinetics.
The administration of phages in the presence of susceptible hosts allows for active phage therapy, wherein the effective infection cycle (adsorption—replication—lysis) occurs at the expense of the abundant hosts. 32 However, this phenomenon does not occur instantaneously, as phage populations should be of sufficient density to continuously infect and lyse the host population.35,36 The 6–12 h time frame stated in both studies may consider the substantial lag in phage-host interactions, allowing for a more successful bactericidal action of phages before the administration of antibiotics.
Another significance of applying the sequential order of administration is the likelihood of biofilm formation. Even for bacteria that remain susceptible to antibiotics, the formation of a biofilm affords incredible resistance, most especially in nosocomial infections. Most common treatments against biofilm-forming strains employ the use of anti-biofilm peptides and antibiotic combinations that prevent biofilm formation.
The persistence of bacteria in biofilms allows enhanced antimicrobial resistance due to poor diffusion of the antimicrobial agents against the biofilms, hindering the penetration of treatments in the cells. 37 Roy et al. and Verderosa et al. hypothesized three major reasons why known antibiotics are incapable of eradicating biofilms.
Aside from the restricted diffusion or penetration of the treatments across the film, the resistance of pathogens is commonly conferred throughout the biofilm through gene exchange/transfer. In addition, the biofilm alters the cellular environment and the metabolism of the bacteria—wherein most of the bacterial cells deep inside the film enter a dormant state (called persister cells) and are commonly not susceptible to antimicrobial agents.38,39
Phage-antibiotic combinations target the factors outlined by Roy et al. and Verderosa et al.38,39 The biofilm is disrupted as the virions invade the matrix.40–42 The high bacterial density inside the matrix provides an ideal environment for phage replication. The matrix would have been dissolved by the phages' depolymerases, and the antibiotic would then be free to penetrate and diffuse into the biofilm. 43 This exposes the metabolically inactive bacteria innermost of the film, enabling both antibacterial agents to clear out the remainder of the infection (Fig. 4).

Sequential administration of phages first and then antibiotics resulting into an effective clearing: (1) bacteria covered with biofilm; (2) administration of phages; (3) phage replication and bacterial biofilm disruption; (4) administration of antibiotics; and (5) both agents work together in eradicating the bacterial infection. Created with BioRender.com. Agreement number MO255AJJ8M.
Simultaneous administration of phages and antibiotics would hinder penetration of phages and dissolution of the biofilm matrix, which, in turn, prevents the antibiotic from taking effect.44,45 Simultaneous applications suggest that, in comparison with the mechanisms of sequential treatment, both bactericidal agents will be confined only to the upper layers of the matrix, rendering it ineffective.
On the antimicrobial drug dosage
In any living organism treated, pharmacokinetics and pharmacodynamics present themselves uniquely to each individual drug and, in this case, bacteriophage.46,47 These different interactions between the body, the drug, and the phage play a huge role in the determination of optimal concentrations and whether the said combination would be effective in treating an infection.15,22,48
Although the use of minimum inhibitory concentration (MIC) for antibiotics is based on established clinically relevant concentrations, that is, a concentration that ensures bacterial clearance—in the case of phage-antibiotic combinations, it should be considered that alteration of antibiotic concentration should be done due to its possible interaction with the phages.30,40,44
The relevance of exploring the concentrations of antibiotics in conjunction with phages is to mainly retain or enhance the phages' functionality in infecting the target bacterium, which has been done in various studies as shown in Figure 5. Although most studies have focused on MIC treatments, most of the results published using antibiotics at sub-MIC demonstrated much better antibacterial activity at sub-MIC than at higher concentrations.30,40,44
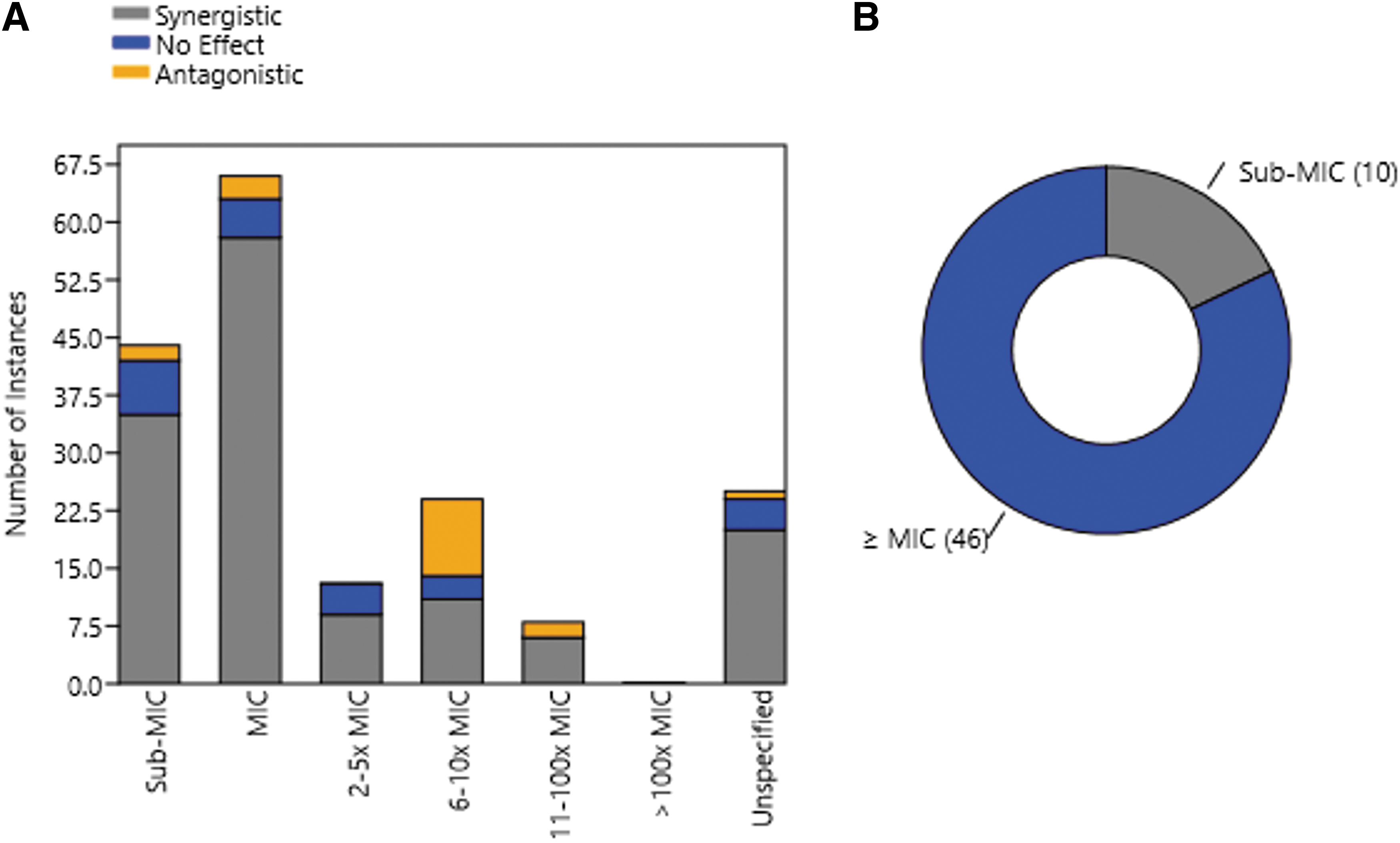
Number of instances of phage-antibiotic combinations displaying synergistic, neutral, or antagonistic effects counted per antibiotic per pathogen
The occurrence of antagonism seems to increase when the concentration is at ≥MIC: All 10 related studies in our review that explored sub-MIC antibiotic levels showed better synergy than antibiotics at ≥MIC. Some were even antagonistic at higher concentrations but synergistic at sub-MIC. A trend may be evident, wherein high antibiotic concentrations cause a large decline of bacterial densities and affect the phage proliferation threshold, which then opposes new bacteriophage infections.44,49,50
In combination therapy, pathogens are exposed to sub-MIC concentrations mainly to assist the bacteriophages through altering the biochemical and physiological characteristics of the pathogen, as well as the upregulation of cell lysis and bacteriophage reproduction.44,51 This amount of dosage impairs bacterial functions via affecting its virulence agents, namely motility, adhesion, oxidative stress sensitivity, cell surface hydrophobicity, and biofilm formation. 52
The changes in the bacterial characteristics pose advantage in adjunct phage treatment at sub-lethal concentrations of antibiotics—where lowering the dose of antibiotics to half or quarter of the original MIC will lessen dose-dependent side effects and toxicity, making the pathogens susceptible to both bacteriophage and antimicrobial drugs.48,53
For example, sub-MIC dosages of macrolides and aminoglycosides were found to inhibit the formation of biofilms in P. aeruginosa infections. 52 When the concentration of vancomycin was lowered, the biofilm reduction was enhanced as compared with cefazolin in which the formation increased. The reduction of biofilm production in these target bacteria, when used in combination treatments, is vital to the adsorption and infection of bacteriophages.
Another example of the use of sub-MIC against bacteria is through the study by Comeau et al., where bacterial filamentation was observed in the target host bacterium after exposure with suboptimal concentrations of B-lactam antibiotics. Enhanced phage infection was observed in their study, which they attributed to the change of bacterial physiology due to exposure to the lowered antibiotic concentration. 23
Some studies also showed that antimicrobial agents may possibly induce biofilm formation such as ceftazidime, benzalkonium chloride, piperacillin, chlorhexidine, ticarcillin, ciprofloxacin, amikacin, and carbenicillin in 10 isolates of P. aeruginosa.51,54,55 This is evident in Gram-positive pathogens due to the increase of the biofilm component eDNA during cell lysis. 56
Beta-lactam antibiotics were also proven to induce biofilm formation in S. aureus strains. 57 The varying sub-MIC exposure results can also be possible due to the quorum sensing systems.58,59 Here, it can be seen that the antibiotic mechanism of action should also be considered, especially when used at sublethal concentrations.
On the mechanisms of action
As with the previous section, extensive swelling or filamentation does not just happen with any antibiotic. Rather, it occurs when bacteria are exposed to antibiotics that inhibit cell wall biosynthesis (e.g., penicillins, cephalosporins, and carbapenems). To take advantage of this class of antibiotics, the bacterial population must be metabolically active. This explanation conversely provides a generalization on antibiotics that inhibit protein synthesis or those that act as antimetabolites—antibiotics that are bacteriostatic inhibit the proliferation of the bacterial population on which phages capitalize.
In the study by Liu et al., five (5) antibiotic classes were tested in conjunction with phage treatments. In the study, they used trimethoprim (folic acid synthesis inhibitor), colistin (cell membrane disruptor), ceftazidime (cell wall biosynthesis inhibitor [CBIs]), ciprofloxacin (DNA topoisomerase inhibitor), and kanamycin (protein synthesis inhibitor).
They found that the combination treatment against Escherichia coli strains resulted in the most synergistic interaction when phage and ceftazidime are combined. Antagonistic interactions were observed in colistin, ciprofloxacin, and kanamycin, whereas negative synergy was observed in using trimethoprim. 60
Similarly, antibiotics that target protein synthesis tend to work antagonistically in the presence of phages, as stated in the studies by Akturk et al., Berryhill et al., and Davis et al.31,40,61 This can be explained with the fact that proteins are integral to the formation of phages and that phage proliferation depends heavily on rapid bacterial metabolism normally used for cell division, a process that bacteriostatic antibiotics target. 40
Majority of the studies related to ESKAPE pathogens used either cell wall synthesis inhibitors or protein synthesis inhibitors, as seen in Figure 6—with most synergistic results coming from the combination of phages and CBIs.
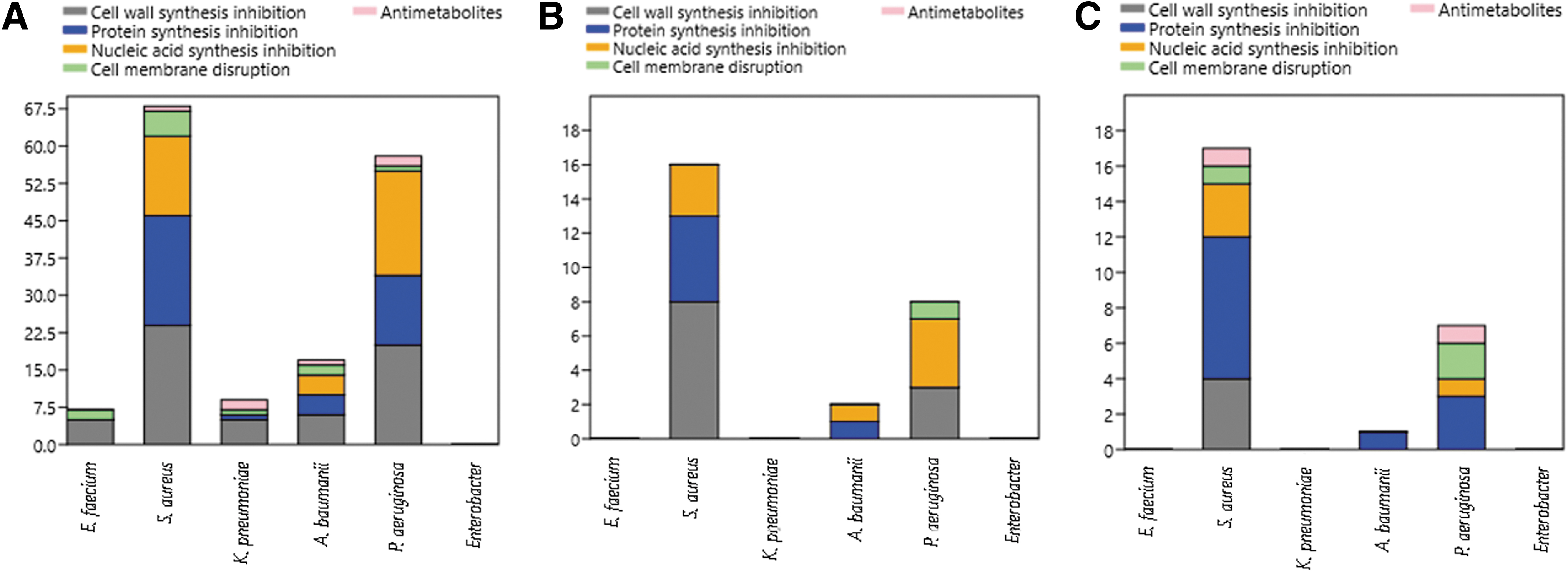
Number of instances of phage-antibiotic combinations using antibiotics with different mechanisms of action per pathogen and different effects—synergistic
Results, however, are not always consistent, as different parameters are applied in each study—including time and order of administration and the concentration of the antimicrobials used in combination with the phages. As stated previously, most studies are limited only to simultaneous applications and administration at MIC. In a similar review by Liu et al., PAS cannot be generalized—in the sense that each parameter is ultimately based on the target pathogen. 29
While CBIs are commonly used together with phages, antagonistic interactions can also be observed, as shown in Figure 6. Some antibiotics such as aminoglycosides (e.g., Gentamycin, Tobramycin, and Amikacin) commonly exhibit antagonistic interactions with phage due to their inhibitory effects in protein synthesis, whereas synergistic interactions can be observed at sub-MIC during sequential applications.
On transferability: from in vitro to in vivo and clinical applications
Carascal et al. defined transferability of phage applications in the context of SEA countries. In their review, they outlined three phases of implementation of phage studies—from (1) basic research including extensive phage isolation and characterization, (2) laboratory and clinical applications, and (3) adaptive regulatory mechanisms (or establishment of guidelines for development and use of industrial and pharmaceutical phage-based products).
The translation of lab-based applications to clinical trials relies on the optimization and stability of the combinations tested. In this case, the first two phases outlined by Carascal et al. work hand in hand, as extensive characterization of phages would provide more information on the infective ability of the isolates, alongside testing as adjuvants with known antibiotics.
In testing for efficiency in animal models, one must first determine the capacity of a particular phage-antibiotic combination to work synergistically. The environment within a host, however, will never be easily replicated in vitro. This massive difference in the complexity and number of other factors would dictate that the trend cannot be expected to be universal, and even if it were, certain physiological mechanisms must be taken into consideration before combination therapy—or any therapy with phages for that matter—is attempted. 62
According to the Antibacterial Resistance Leadership Group and National Institute of Allergy and Infectious Diseases Phage Taskforce, clinical phage therapy can be considered in bacterial respiratory tract infections, urinary tract infections, infections involving immovable devices, endovascular infections, and gastrointestinal infections. Most applications of compassionate use of phages are often employed with known antibiotics. 63 Table 2 lists sample studies that show both in vitro and in vivo applications of combination treatments.
Clinical Applications of Phage-Antibiotic Combination Treatment
ATM, aztreonam; BFC1, bacteriophage cocktail 1; CLI, clindamycin; CST, colistin; MEM, meropenem; MIC, minimum inhibitory concentration; PNM, Pseudomonas aeruginosa Bacteriophage; SMX-TMP, Sulfamethoxazole-trimethoprim.
Nir-Paz et al. treated a 42-year-old male patient with bacterial osteomyelitis involving extensively drug resistant (XDR) A. baumannii and MDR K. pneumoniae. Inefficacy of antibiotic treatments against post-surgical infection resorted to the use of phages ɸAb4909phi111 and ɸKpI303phi158, alongside colistin and meropenem. In vitro testing of phages with meropenem in culture media showed favorable results (exhibiting the most bacterial reduction compared with single phage and antibiotic treatments), which translated to in vivo applications.
Both phages and antibiotics were administered intravenously (IV), for 5 days. Interestingly, clearance of A. baumannii cultures was observed after the first treatment duration, and a second treatment course was done to ensure the eradication of K. pneumoniae. 64
Bao et al. similarly treated a 63-year-old female patient with persistent XDR K. pneumoniae urinary tract infection. In vitro testing of phage cocktail consisting of six phages and the different concentrations of Sulfamethoxazole-Trimethoprim (SMX-TMP) against K. pneumoniae strains showed positive results—exhibiting clearance of bacterial cultures in liquid medium.
The synergistic interaction observed led to in vivo administration, wherein the phage cocktail was administered via bladder irrigation along with oral administration of trimethoprim-sulfamethoxazole, which resulted in a synergistic effect. Both treatments were given once a day for five consecutive days. Afterward, the patient recovered completely with no recurrence during the 6 months follow-up. 65
Van Nieuwenhuyse et al. reported a case of a 10-year-old female patient with Ewing's sarcoma that became infected by Clostridium hathewayi, Proteus mirabilis, Finegoldia magna, and methicillin-susceptible S. aureus months post-surgery. In vitro testing of S. aureus phages from the cocktail Bacteriophage Cocktail 1 (BFC1), combined with three candidate antibiotics clindamycin, rifampin, and ciprofloxacin.
Omnilog assays using the combined formulations showed that only phage with clindamycin showed synergistic results—exhibiting a decrease in bacterial growth after 72 h when compared with other combination treatments and with the phage treatment alone. When tested in patients, an initial synergistic interaction was observed, as with the in vitro results; however, resurgence of secondary infections occurred.
The application, in this case, was considered a failure both in the conventional applications and in the combination treatments that the author attributes to the polymicrobial nature of the infection. It cannot be denied that the phage-clindamycin treatment did work initially, however the lack of antimicrobial agents addressing the other bacterial pathogens led to the persistence of the infection and relapse of the S. aureus infection, after initial eradication. 66
Lastly, another study by Van Nieuwenhuyse et al. reported on the use of bacteriophage-antibiotic combination against nosocomial infection of XDR P. aeruginosa post-living donor liver transplant in a male toddler. The systemic infection caused by the HAI P. aeruginosa prevented re-transplantation in the toddler, and clearance of the pathogen is prevented due to its XDR nature.
As with their previous study, the authors employed the use of phage cocktail BFC1 to address this infection, which was used alongside antibiotics gentamycin, colistin, and aztreonam. In vitro testing of phages and antibiotics showed favorable results, with all antibiotics exhibiting synergistic interactions. They also tested BFC1 phages in Phage Immune Neutralization (PIN) assay.
The PIN assay tests the neutralization capacity of the patient's serum against the bacteriophages before in vivo administration of the treatments. Interestingly, no significant immune neutralization occurred in the P. aeruginosa phages. In vivo applications involved daily 6-h IV infusion of BFC1 spanning 86 days, with adjunct administration of antibiotics to aid the clearance of other microbial infections. The results showed, all in all, that sustained recovery of the patient was observed aided by the use of both antimicrobial agents. 67
Currently, compassionate use or investigational therapy involving urgent life-threatening conditions is the typical regulation governing bacteriophage therapy. This can be observed in the presented studies, as there is a common denominator wherein the use of phages is considered as “salvage therapy” or the “last resort” treatment. Moreover, several characteristics of phages should be considered before their use. For example, Phage cocktail BFC1 is used in both studies by Van Nieuwenhuyse et al.66,67
This specific formulation of phages has been tested extensively—from its physiological to its genomic characteristics. A major aspect of this is the screening for genetic determinants for lysogeny, toxins, and antibiotic resistance genes. Alongside this, the phages are also strictly lytic and the preparations should contain <5 EU/mL of endotoxins. 67
The presented studies in Table 1 consider some of the aspects that were discussed early on. The order of treatment is not explicitly stated in each study, but it is one of the factors that were recommended in each. Different concentrations of antibiotics were also tested, wherein the use of sub-MIC antibiotics is done in two of the applications. Lastly, considerations of the Mechanism of Action of the antibiotics were not explicitly stated; however, the candidate antibiotics used were those to which the target bacterium is still susceptible.
Considering the use of phage, the aspects of phage-antibiotic combinations, and the nature of the target host itself is truly a complex field and is multi-faceted in terms of its applications. There are, indeed, many factors to consider aside from those that are outlined in this study. However, this provides groundwork for those who consider pursuing phage-antibiotic applications. It is, still, undeniable that the use of combination treatments offers such a valuable option in instances where all conventional treatments are exhausted.
A Note on Bacterial Resistance and Re-Sensitization
Another striking observation in the effects of combination therapy is that chances of a relapse with a resistant strain would be drastically reduced.22,46,68 With two (2) drivers of evolution going toward different directions, there is only an extremely small likelihood of any resistant strain emerging. 69
In many of the studies we have examined, no resistant strain emerged at all.30,70–73 The physiological cost of mutating resistance to either agent is already taxing74–77 ; to mutate and become resistant to both is too unlikely,41,78 and those that do display far less virulence than those that remain sensitive to the antibacterial agent. 79
The presence of phages induced bacterial re-sensitization toward antibiotics against which the bacteria already developed prior resistance48,69,74,75,79,80 or demonstrated that this condition would almost certainly have occurred had they tested for it.41,81 Another possible explanation is where cell surface receptors of bacteria degenerate through phage infection, allowing the efflux of antibiotics, to which the bacteria are resistant prior to the exposures. 82 Others, meanwhile, observed a reestablishment of sensitivity to phages in the presence of both phages and antibiotics.22,83
The pathogens are able to make trade-offs with biofilm formation, bacterial growth, nutrient uptake, virulence, and antibiotic resistance.84–86 Bacteria develop resistance to phages via altering their virulence factors, such as capsules have a beneficial effect because they reduce antibiotic resistance and stimulate macrophage phagocytosis.87,88 Conversely, it was proven that using bacteriophage cocktails, containing three or more strains, decreases the possibility of bacteriophage resistance.89–92
The mechanisms by which these occur find their way back to three (3) fundamental points: bacterial physiology, evolution, and population dynamics. Over time, the bacterial populations would face selective pressure from both phages and antibiotics. This necessitates evolutionary trade-offs to allow the sensitive bacteria to develop resistance to either phages or antibiotics.
Resistance to phages tends to manifest as mutations of the type IV pili or the lipopolysaccharide, which are major virulence factors. 77 Others that did become resistant to phages lost their resistance to cell wall inhibitors. According to Chatterjee et al., vancomycin-resistant strains of E. faecalis in the intestines became less able to colonize a host and are unable to propagate because of the normal microbiota that was left undamaged because of the use of phages as adjuvant. 75
The phage susceptibility and antibiotic sensitivity can be tested to propose a precise treatment appropriate to the bacterial strain. It is also important to consider the mechanism or action of both the phage and antibiotics, as it may lead to cross-resistance to both antibacterial agents. 93 A careful choice of combinatorial therapy is needed to lower AMR. Therefore, these evolutionary trade-offs can be put into good use if specific bacterial and bacteriophage characteristics are considered. 94
Recommendations
The demand for more innovative ways to counter bacterial infections forced additional effort into the field, which yielded more studies in recent years. While phage-antibiotic treatments certainly provide a novel avenue for alternative treatment modality, its multifactorial nature renders it complex and, therefore, necessitates further research involving its effects and interaction.
In the conduct of combinatorial phage-antibiotic therapy, it is important to give due consideration to the four factors outlined in this study, as these essentially form the backbone for effective testing of the said treatment. These play on the nature of the phages itself, and the mechanisms of present antibiotic drugs.
As discussed, these factors play into the efficacy of combinations where, ultimately, phage recognition and adsorption work effectively, paired with the correct antibiotic, when adsorption and receptor recognition are considered. As a result of their combination, the evolution of resistance to either antibacterial agent is inhibited and re-sensitization may occur.
To address these aspects, an antibiotic paired with a bacteriophage must be tested together at varying concentrations (multiple setups with different concentrations ≥MIC) and order of treatment, with added experimental setups to explore changes in the interval when sequentially applying phages and antibiotics. It is likewise important to ensure that four different arrangements (each ideally with animal models in triplicate) would be prepared to use (1) antibiotic-resistant bacteria, (2) antibiotic-sensitive bacteria, (3) phage-resistant bacteria, and (4) phage-sensitive bacteria at the start to simultaneously observe the distinction of (1) antibiotic re-sensitization, (2) prevention of antibiotic resistance, (3) phage re-sensitization, and (4) prevention of phage resistance. A sample of experimental design is shown in Figure 7.

Overview of proposed experimental setups for each combination of an antibiotic and a bacteriophage (single phage or phage cocktail). Setups using antibiotics should use several different concentrations (sub-MIC, MIC, and >MIC). Created with BioRender.com. Agreement number HW255AFYTV.
Logistically, assessing multiple factors in a study (for a single phage-antibiotic interaction) would play out to be tedious and, not to mention, costly. An approximate of around 3600 thoroughly characterized bacteriophages are needed for the ESKAPE pathogens alone, with the confirmation that they are lytic with no virulence factors. 90
Moreover, the stringent assessment of methods to be employed in each should be done to determine the novelty and efficacy of each interaction. We do not recommend that bacteriophages should replace antibiotics entirely. Rather, current evidence suggests that a combination therapy is both stronger and more able to prevent future antimicrobial resistance than either phages or antibiotics alone.
The present data relating to phage-antibiotic combinations in this study provided figments of information that are, at best, suggestive rather than conclusive, but they provide a certainty in the efficacy of the said treatment regimen. Whether performed in single research or in a series of linearly planned, correlated studies based on the outlined factors earlier would provide more substantial evidence to this regimen—providing clarity in different aspects that can be further explored and developed in the field.
Footnotes
Acknowledgments
The researchers would like to extend their gratitude to the UST BEATS Research Group for supporting this paper and for providing financial assistance.
Authors' Contributions
G.B.N.F.: Conceptualization, Writing—Original Draft, Resources, Data Curation, Visualization, and Writing—Review and Editing. J.C.W.U.: Conceptualization, Writing—Original Draft, Resources, Data Curation, and Visualization. K.L.J.P.: Conceptualization, Writing—Original Draft, Resources, Data Curation, and Visualization. C.M.A.C.: Conceptualization, Writing—Original Draft, Resources, Data Curation, and Visualization. D.P.S.C.: Conceptualization, Writing—Original Draft, Resources, Data Curation, and Visualization. T.A.D.G.: Writing—Review and Editing, Data Curation, Visualization, and Supervision. M.R.J.C.: Writing—Review and Editing, and Supervision. D.M.D.P.: Conceptualization, Writing—Review and Editing, Data Curation, and Supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this publication.