
Abstract
Rising antibiotic resistance among bacterial pathogens has become a substantial health issue for human civilization. The emergence of these pathogens in high-risk diseases such as cystic fibrosis (CF) has led to financial and nonfinancial losses, necessitating alternative therapies. This study presents an overview of such approaches, including phage therapy, antimicrobial peptides (AMPs), nanotechnology, monoclonal antibodies (mAbs), microbial therapies (probiotic therapy), clustered regularly interspaced short palindromic repeats technology (CRISPR), and aptamers focusing on their mechanisms of action and exploring the impact of combining phage and phage derivatives with the mentioned approaches. Although alternative approaches and their combinations with phages show promise, the phage–antibiotic combination has been the subject of most studies, and It has been proven to be highly effective in combating antibiotic-resistant infections. Other combinations also appear promising, but further studies are needed to determine their effectiveness. This emphasizes the need for more thorough research into different phage combination treatments beyond the well-established phage–antibiotic strategy.
Introduction
Antimicrobial resistance (AMR) has become one of the most troublesome issues of hygiene that can make current medicine insufficient. With the continuing indiscriminate use of antibiotics, it is estimated that AMR will continue to grow, resulting in reaching AMR casualties more than 10 million deaths per year by 2050. 1 The consistent increase in AMR and the declaration of emergency for this situation by the World Health Organization (WHO) make the future of antibiotics as a proper therapeutic approach for bacterial infections unclear. 2 The situation even gets worse by emerging persistent bacterial infections. Among bacterial pathogens, ESKAPE bacteria are considered the most problematic pathogens with drug-resistant features and the leading cause of persistent infections. Moreover, based on WHO predictions, antibiotic-resistant microorganisms, with ESKAPE pathogens playing a major role, could cause 10 million deaths per year by 2050. The WHO anticipates this scenario if no action is taken against AMR. 3
The prevalence of mixed bacterial infections (MBIs) in high-risk diseases such as cystic fibrosis (CF) patients 4 with the ability to survive against frequent antibiotic exposure raises concerns regarding the effectiveness of existing antibiotic treatment approaches and demand for innovative antibacterial therapeutics other than antibiotics due to the complicated situations that the patients can face. For instance, CF patients usually risk a high prevalence of persistent MBI due to high mucus density in the airways. 5
Bacteriophages (phages), 6 antimicrobial peptides (AMPs), 7 nanotechnology, 8 monoclonal antibodies (mAbs), 9 probiotics, 10 clusterd regularly interspaced short palindromic repeats (CRISPR) technology, 11 and aptamers 12 are treatment approaches that have been studied as alternative treatments recently. Since phages are safe and have high potential antimicrobial activity against drug-resistant bacteria, this treatment method can be evaluated against persistent bacterial infections. 13 In addition, AMPs have notable antimicrobial activity (membrane disruption, 14 targeting polysaccharides 15 and intracellular components, 16 and antibiofilm activity 17 ), are broadly expressed in eukaryotic and prokaryotic organisms, and are considered an alternative way to combat drug-resistant bacteria. 18 In recent years, nanotechnology has become a well-known strategy widely used in various biological approaches, including antibacterial drug development. 19 Applications of nanotechnology in tackling AMR include utilizing nanoparticles (NPs) as drug carriers 20 or using them as direct antibacterial agents due to their antibacterial activity via disrupting the cell wall and cell membrane, reactive oxygen species production, targeting intracellular composition, and antibiofilm activity. 21 Another promising treatment approach is mAbs. Due to specificity and high potential antibacterial activity by four different mode of actions, including neutralizing bacterial toxins, antibody-dependent cell-mediated cytotoxicity (ADCC)-killing, opsonophagocytosis, and inhibition of bacterial virulence factors, mAbs have gained researchers’ interest as an alternative therapeutic approach.22,23 The antibacterial activity of probiotics, which is originated from their immunomodulatory properties, production of antimicrobial substances, showing competitive exclusion with pathogen bacteria, enhancement of mucosal barrier function, 24 and antibiofilm activity, 25 as well as their positive impact in increasing patients’ quality of life, draws researchers’ attention to these approaches to develop novel antibacterial medicine.26,27 Another example of novel treatment approaches to eliminate bacterial pathogens is targeting specific genes such as virulence or antibiotic resistance genes, which can be done via nucleic acid-based therapeutics such as aptamers or CRISPR as a direct therapeutic approach.11,12
The prevalence of MBI with AMR features in high-risk patients makes treating procedures complicated, which can increase the mortality rate of individuals. Thus, combating these microorganisms with the optimal treatment choice that can be applied alone or in combination is crucial to avoid AMR. This review sheds light on recent advances in possible phage and phage combinations with other alternative therapeutic combinations against drug-resistant bacteria. The mechanisms of action of these methods are also discussed. However, the main goal of this study is to highlight phage therapy and combination phage therapy.
Antibiotic Therapy for Bacterial Infections
The first antibiotic in history, salvarsan, was introduced in 1910 (Fig. 1); since then antibiotics have significantly altered modern medicine and increased the average life expectancy of humans. The most successful period of natural-based antibiotic discovery began in 1928 with the discovery of penicillin. Despite the mentioned advantages, the indiscriminate use of antibiotics and the reduction of their development gradually resulted in the emergence of AMR. 28

Illustration showcasing the timeline of the alternative therapeutic approaches. These events are significant as they mark the first incidents in history, such as the discovery of the initial substance of its kind. Within the figure, the gray line denotes critical historical events related to antibiotics.28–31 Additional events, such as those connected to ABNPs,32,33 nanocarriers,8,34,35 and CRISPR technology, 36 are marked on the gray line, with colored sections placed just above it. Furthermore, events associated with AMPs37–40 and probiotics26,41–44 can be found on the gray line, and colored segments are placed in the middle of the figure to highlight their importance. As for aptamers, their related events45–47 are depicted on the gray line alongside colored sections at the top of the figure. Phage therapy events 48 can be observed in the colored parts at the figure’s top. Finally, events concerning mAbs22,35,49 are presented on the gray line and in the colored sections beneath it. ABNPs, antibacterial nanoparticles; CRISPR, clustered regularly interspaced short palindromic repeats; AMPs, antimicrobial peptides; mAbs, monoclonal antibodies.
AMR prevalence is not the only cons of antibiotics. Although they are essential for treating bacterial infections, antibiotics can have several adverse effects on their consumers. Along with neurological and psychiatric side effects such as confusion, headaches, seizures, and anxiety, 50 these side effects also include gastrointestinal disturbances such as nausea, vomiting, and diarrhea.51,52 Furthermore, the use of antibiotics can change the gut microbiota, which can lead to antibiotic-associated diarrhea and worse disorders such as toxic megacolon and colitis. 53 Also, in a recent study, Klingel et al. reported that the CF patients who received azithromycin as a treatment had an inferior pulmonary function in comparison with patients who did not receive azithromycin as a treatment (azithromycin nonconsumers); additionally, they were coinfected with methicillin-resistant Staphylococcus aureus (MRSA) more than azithromycin nonconsumers and had lesser relative FEV1 feedback. 54 Furthermore, antibiotics have an antibacterial activity against nonpathogenic and symbiotic bacteria, resulting in a decline in lung function, changing the microbial ecology of the lungs, and the prevalence of some ESKAPE pathogens such as Enterococcus spp. and Klebsiella pneumoniae in CF patients.55,56 Therefore, despite the urgent demand for new antibacterial treatments, many pharmaceutical companies have pulled out of new antibiotic research projects in favor of focusing their development and research efforts on alternative therapeutic areas. 57
Phage Therapy
Phages are 50–200 nm viruses that attack and infect bacterial hosts. 58 Phages are widely spread throughout the biosphere because they are obligatory bacterial hosts and can be found practically everywhere, even in the human body. 59 Due to abundant alternative treatments for patients infected with antibiotic-resistant bacteria and the promising outcomes from current case studies using personalized phages, interest in using phages as a therapeutic agent has recently increased. 60 Utilizing phages as a therapeutic agent has proven efficient and secure for treating infectious disorders brought on by various species of bacteria, including drug-resistant strains. 61 Notwithstanding, phage therapy still has cons, including the high cost of phage screening, time-consuming procedure within diagnosis and treatment, the emergence of phage-resistant bacteria, fewer clinical trial data, and induction of phage-neutralizing antibodies in the body. 62 Nevertheless, by adopting appropriate solutions and optimization, the negative aspects of phage therapy can be adjusted to some extent. For example, establishing novel high-throughput screening techniques can lower the cost of phage screening. 63 Rapid diagnostic tools can shorten the time it takes to diagnose and treat a patient. 64 Phage cocktails can be used to fight bacteria that are resistant to phages. 65 Phage therapy’s acceptability and dependability will increase with the collection of more clinical trial data and the standardization of methods. Lastly, methods such as encapsulated phages to avoid or decrease phage-neutralizing antibodies can improve the effectiveness of treatment. 66
Lytic Activities of Phages
The lytic activity of phages originated from their life cycle. After completing the prelysis stages of the single life cycle of phages, including attachment, infection, multiplication, and assembly, host cell lysis occurs thanks to lysis-related proteins of phages. 67 The use of phages in planktonic form, which uses the mechanism of host lysis, goes back a hundred years to treat bacterial infections. Nonetheless, due to the emergence of antibiotics, using phages as medicine was limited to a few countries. 48
Due to increasing studies with promising results about the therapeutic potential of lytic phages against drug-resistant bacterial pathogens 68 and MBIs, 69 phage therapy is a high-potential alternative treatment for complicated bacterial infections. Although planktonic phages are not the only phage therapy option, phage derivative substances such as lysis-related agents (such as enzymes and proteins) can be another promising route to fight against AMR.
Endolysins are phage-coded enzymes that can degrade the bacterial host’s peptidoglycan. Due to peptidoglycan degradation activity similar to penicillin’s antibacterial mechanism, these enzymes are so-called enzybiotics. 70 Owing to the broader spectrum and lower resistance rate development, quick action, and supreme efficiency compared with phages, endolysins are considered a reasonable alternative phage-derived approach to combat antibiotic-resistant bacteria. 71
Virion-associated peptidoglycan hydrolases (VAPGHs) are another phage-related peptidoglycan-degraded enzyme that belongs to the enzybiotics. 72 VAPGHs consider endolysin analogs and show peptidoglycan degrading activity similar to endolysins except for lytic transglycosylase activity. 73 Moreover, they are generally larger and structurally more diverse than endolysins. 74 In addition to antibacterial activity, due to other properties such as its mode of action, which causes low resistance occurrence to these enzymes, specificity, stability to high thermal conditions, and feasibility of modular designing, make these enzymes a good representative of a suitable enzybiotic and a potential solution to AMR.73,75
Depolymerases are another phage-encoded enzyme with antibacterial activity. Thanks to their polysaccharide degradation features, these enzymes gain researchers’ attention by degrading extracellular polymeric substances. These antipolysaccharide features help phages penetrate biofilms and invade bacterial host cells by degrading their capsules via targeting capsular polysaccharides. 76 Specific and high-potential anticapsule activities of depolymerase against various K. pneumoniae 77 and Acinetobacter baumannii 78 capsular types were reported in previous studies. Moreover, these enzymes can target various substrates, including sialic acid, rhamnogalacturonan, galacturonate, and alginate, making depolymerases promising alternative therapeutic approaches against antibiotic-resistant bacteria. 79
Holins and pinholins are other examples of phage-related proteins with potential antibacterial activity. Holins can form 200–400-nm holes in the plasma membrane of bacteria. These holes are formed to assist endolysins in being released and hydrolyze cell walls, and it is necessary for endolysins to reach peptidoglycan. 80 Holin’s antibacterial potential alone and fused with endolysin were reported in previous studies. 81 In addition, the antibacterial potential of holins against both gram-positive and gram-negative bacteria suggests that holins may have a wider variety of applications than endolysins. Moreover, holins can be modified to include a supplementary peptide that selectively attaches and targets specific bacteria. Hence, holins can be applied in a wide range of biotechnological applications, such as gene therapy and bacterial infection control. 82
Pinholins are lytic proteins of phages considered members of holins class II. 83 These proteins make pinholes less than 2 nm in diameter in the host bacteria’s inner membrane. The pinholes’ size prevents endolysin from passing through them. However, it does allow ions to get through, which depolarizes the membrane, enabling the signal-anchor-release (SAR) endolysins to be folded back into an active form and target the peptidoglycan. 83 In addition, despite holins, there is no evidence of pinholins’ antibacterial activity alone or in combination with other substances. Nonetheless, pinholins have an essential role in the phage lysis cycle despite their mechanism of action still needing to be fully understood. 84
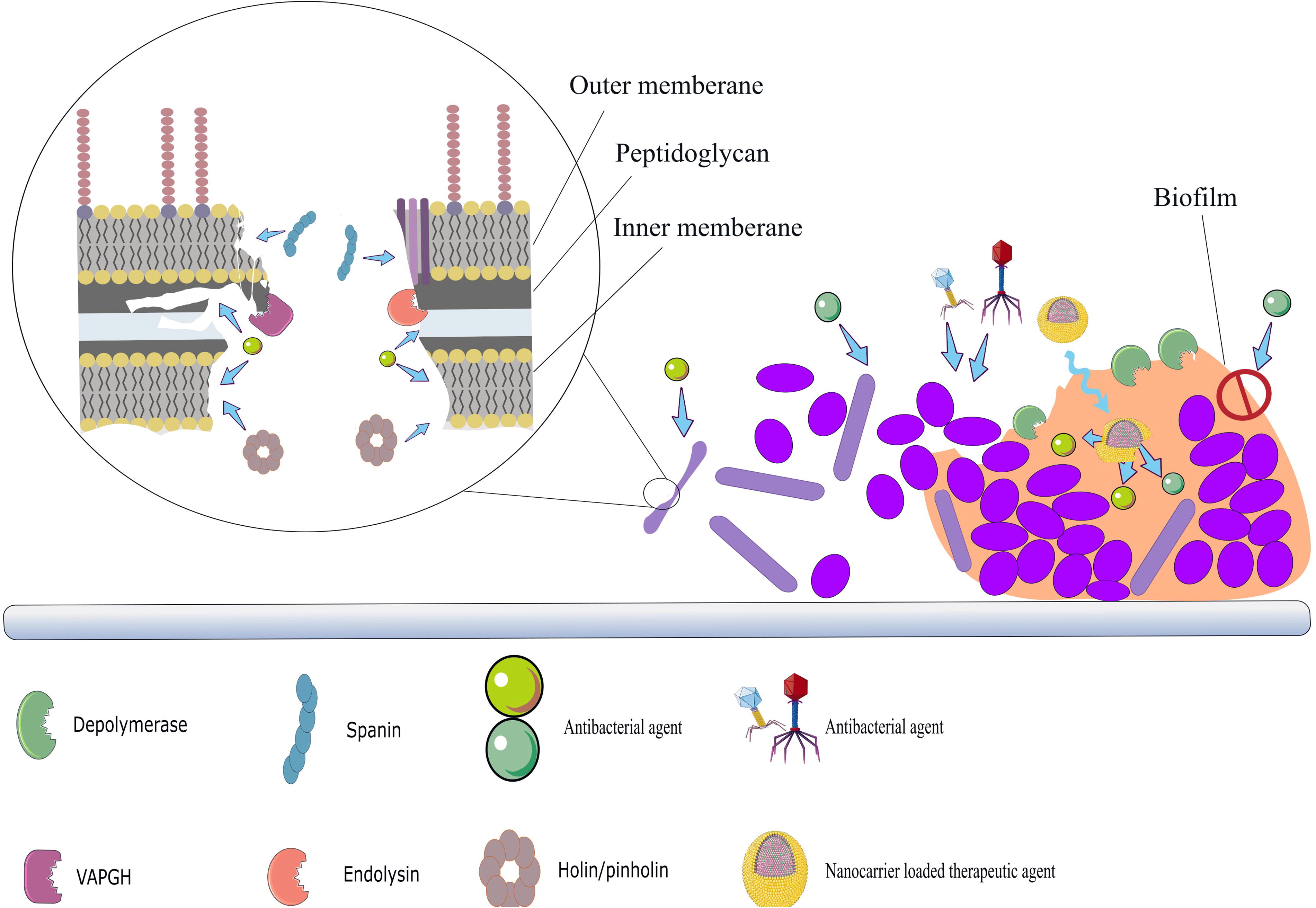
While other phage-related substances degrade the cell wall and inner membrane of bacteria, an interruption of the outer membrane of gram-negative bacteria is also crucial. The specific phage-encoded proteins known as spanins 85 make this interruption activity possible. Without spanins, the lysis procedure is expected to be prevented, and the release of virus particles from the bacterial cells will be inhibited. 86 In addition, it is believed that the peptidoglycan meshwork inhibits spanin’s action. Hence, peptidoglycan disruption mediated by holins and endolysins is necessary for the spanin mechanism of action. 84 The outer membrane interruption should have occurred following the endolysins’ peptidoglycan hydrolysis, 84 showcasing the interconnectedness of these processes in the degradation of bacteria and the possible combination of the three phage-encoded proteins as a therapeutic approach. The antibacterial mechanisms of action of phage and phage derivatives are provided in Figure 2.

Antibacterial mechanisms of phages and phage derivatives. Lytic phage’s antibacterial mechanism consists of injecting genetic material by phage, then the molecular machine of bacteria is stolen, and phage progenies are released following the disruption of the bacterial cell wall. Cell wall disruption can be mediated by several phage-related enzymes and proteins that target the capsule, outer membrane, peptidoglycan, and inner membrane.
Why Using Combination Phage Therapy Is Necessary?
With the emergence of antibiotic-resistant bacterial species in the current age, using phage therapy as an alternative therapeutic agent in place of antibiotics is recommended. Although the high specificity of phages is considered one of these viruses’ most challenging features. 87 Owing to the prevalence of unusual MBIs (bacterial infections with more than one bacterial species) with drug resistance characteristics that increase the mortality and morbidity of patients, 88 using phages as a therapy has become a sophisticated therapeutic approach. This complicated situation can be prevalent in different types of disorders, such as urinary tract infections, 89 chronic osteomyelitis, 90 various types of infections in individuals with diabetes, 91 HIV, 92 and CF. 93 Hence, to combat drug-resistant MBIs in the mentioned patients, phages as a monotherapy must be combined with other therapies to increase the chance of curing patients. In addition, combining therapeutic agents decreases the chance of acquired resistance among bacteria. 94 Nonetheless, choosing proper agents with some features such as nontoxicity, high antibacterial activity, and lack of antagonistic behavior is crucial to having highly efficient medicine (Table 1).
Comparison of Combined Agents Based on Key Characteristics for Enhanced Efficiency in Combination Therapy
AMPs, antimicrobial peptides; ABNPs, antibacterial nanoparticles; CRISPR, clustered regularly interspaced short palindromic repeats; mAbs, monoclonal antibodies.
Combination Phage Therapy
Generally, combination phage therapy, known as treating infections caused by drug-resistant bacteria with phages in conjunction with antibiotics, 108 can cause a synergistic effect between antibiotics and phages and even resensitize bacteria to antibiotics in some cases. 109 However, according to the recent advances in phage field studies, this definition can change due to promising results of recent studies evaluating the combination of phage therapy or phage-related antibacterial substances with other promising therapies.
Phage cocktails and phage–antibiotic combination
Among other phage combination therapies, phage cocktails and phage–antibiotic combinations have been studied well. The amalgamation of at least two phages, known as a phage cocktail, has emerged as a prospective avenue for combined phage therapies, displaying encouraging outcomes in both in vitro and in vivo experiments. 110 The application of phage therapy as a phage cocktail has several advantages, including the possibility of the synergism effect of different phage particles with each other, 111 reducing phage resistance occurrence, increasing the long-term therapeutic efficacy of phages, and providing various selection pressures to the host cell. 112 Also, it can increase host range and show better antibiofilm activity. 65 The way that phages and antibiotics work together largely depends on their distinctive modes of action. Antibiotics belong to several classes and target bacterial processes, such as DNA replication, protein synthesis, and cell wall construction. The antibacterial effect can be enhanced when combined with phages exploiting these vulnerabilities. For example, bacterial membranes and cell wall disruption by phages can increase the effectiveness of antibiotic treatment.113,114 Moreover, it is shown that utilizing proper antibiotics can facilitate phage progeny release from bacteria. 114
For instance, the antibacterial procedure of the combined phage cocktail with colistin and meropenem was recently evaluated. 69 In the mentioned study, a 42-year-old patient with mixed bacterial (A. baumannii and K. pneumoniae) osteomyelitis was successfully cured by phage cocktails and antibiotics. 69 Also, it is reported that phage-ceftazidime and phage-imipenem/relebactam combination can improve treatment outcomes for drug-resistant P. aeruginosa infections in Siamese cat 115 and a 52-year-old male patient, respectively. 116 Thus, using phages as a cocktail and combined with antibiotics in phage therapy should be prioritized over mono-phage therapy. Nonetheless, the antagonistic effect of some antibiotics, such as β-lactams with some phages, was reported in recent studies. 117 For instance, the antagonistic effect of ciprofloxacin and ΦHP3 due to topoisomerase II inhibition activity of ciprofloxacin against phage and bacteria was detected by Liu et al. 113 Hence, choosing suitable antibiotics to combine with phages based on the phage type and the antibiotic mechanism is crucial for effective combination therapy and avoiding any possible antagonistic effects.
Phage-derivative combinations
Similar to phages, antibiotics can also be combined with phage derivatives. One of the notable combinations in this regard is a combination of Dpo71 (depolymerase) and colistin, which was examined by Chen et al. 118 In the mentioned study, the combination approach shows more antibiofilm effect due to the antibiofilm activity of depolymerase, resulting in high accessibility of colistin to target bacteria. 118 Furthermore, an enhanced antibacterial effect between phage, depolymerase, and antibiotic, 119 as combination therapy consisting of phage KP15, depolymerase KP34p57, and ciprofloxacin, was reported in previous studies, 120 emphasizing the crucial role of KP34p57 in combined phage therapeutics as a biofilm degrader, which provides accessibility of KP15 and ciprofloxacin against target bacteria. Moreover, unlike ΦHP3, no antagonistic effects were detected between KP15 and ciprofloxacin in the mentioned study, suggesting that ciprofloxacin is ineffective or has little effect on phage KP15 topoisomerase II. Also, the study highlights preliminary studies on phage biology before combining them with other antibacterial agents.
As described in previous sections, phage derivatives are complete packages of antibacterial agents targeting the inner membrane, peptidoglycan, outer membrane, and bacteria capsule. In addition to the synergism that can be seen between them, 81 the functionality of some of these derivatives (spanins) is dependent on other derivatives (holins and endolysins). 84 Thus, using these substances in combination seems to be more logical. Notwithstanding, as far as the authors’ knowledge, there is no evidence of using spanins as an antibacterial agent alone or in combination or fused with other phage derivatives, while the synergistic effect of endolysin with holin, 81 VAPGHs, 121 and depolymerase 122 was detected in previous surveys.
Phage-derivative-AMP combination
AMPs are essential elements of the intrinsic immunological defense system. In most living species, AMPs have been produced by the host organism to strengthen the immune response and protect against pathogens. Due to their broad-spectrum antibacterial activity, different pharmacodynamics compared with antibiotics, synergistic effect with antibiotics,37,95 and high potential in degrading biofilms, 123 AMPs are considered high-potential antibacterial agents.
According to previous studies, AMP and phage-derivative combination can be a proper therapeutic approach due to the synergistic effects of these components. Nisin with antibacterial activities, such as creating holes in the membrane and inhibiting cell wall synthesis, 124 and cecropin A with cell membrane interrupting features 125 are among AMPs used as combined agents with endolysins. For instance, it is reported that there is an anti-staphylococcal synergistic effect between LysH5 and nisin. 126 Furthermore, the fused endolysin-AMP agent (ST01-cecropin A) described by Lim et al. shows high antibacterial activity against gram-negative bacteria compared with ST01 alone. 127 The synergistic mechanisms of these peptides with endolysins may be related to their ability to weaken the bacterial membrane, which leaves bacteria more vulnerable to the action of endolysins, which engage the cell wall.
Also, the triple combined therapeutic, including AbEndolysin fused with cecropin A, and cefotaxime, ceftazidime, and aztreonam antibiotics, is another combined therapeutic that showed a synergistic antibacterial effect against A. baumannii. In this study, the combined therapeutic successfully rescued infected mice, emphasizing the pivotal role of phage-derivative-AMP-based combination therapies in combating drug-resistant bacterial infections. 128 In the case of using such a combination, high cell wall accessibility to beta-lactams and endolysin provided by cecropin A in addition to anticell wall activity of beta-lactams and endolysins with two different procedures, including targeting penicillin-binding proteins (PBPs) to cell wall generation inhibition 129 and degrading the peptidoglycan layer of cell walls, respectively, 130 may enhance the antibacterial activity of the agents. However, the antiviral activity of AMPs that can also impact phages is one of the limitations of using these viruses and AMPs as a combination therapy. 131 Thus, the feasibility of amalgamating AMPs with phages that can turn into combined therapy demanded further studies for possible solutions in this manner. Also, investigating the mechanisms of action of AMPs and phage biology is highly recommended to avoid antagonistic effects when used as combination therapies.
Phage and nanotechnology approaches
Nanotechnology can be used to combat drug-resistant bacteria in two different ways. The first method uses antibacterial nanoparticles (ABNPs) as direct antibacterial material. On the contrary, NPs are used as carrier vehicles to deliver medicines to target. 132 NPs with antibacterial activity can be the satisfactory definition for ABNPs. They have many advantages over antibiotics, such as not causing immediate, severe side effects and resistance against them rarely happens.
Moreover, ABNPs are maintained in the body for a notably extended period compared with relatively small antibiotics, which may be advantageous for achieving long-lasting therapeutic effects. In addition, antimicrobial ABNP preparation could be more affordable than synthesizing antibiotics. Also, ABNPs can tolerate the high temperatures used in sterilizing without losing any characteristics that cause conventional antibiotics to become inactive. 96
In previous studies, researchers evaluated the combination of endolysins with various ABNPs, including poly(propylene imine) dendrimers, 133 AgNPs, 134 and carbosilane dendrimers combined therapeutic with endolysin. 135 Additionally, they examined the potential combination of liposome-based ABNPs with a phage cocktail. 136 In the mentioned cases, except carbosilane dendrimers that show synergistic antibacterial effects with endolysin, any other ABNPs enhance the performance of phage cocktails or endolysins. The enhanced antibacterial activity of each mentioned combined therapy might originate from the unique mechanism of action of each ABNP, including the cell membrane disrupting activity 137 of poly(propylene imine) dendrimers, interfering with vital bacterial processes and membrane disruption of AgNPs, 138 and biofilm disruption and interfering with crucial bacterial processes of carbosilane dendrimers (particularly those modified with metal ions such as copper(II) and ruthenium(II)).139,140
Drug carriers can play a pivotal role in unraveling drug-resistant MBI issues. Utilizing NPs as drug carriers has many advantages, such as withholding any interference with nonloaded drugs, 97 the ability to be designed as multifunction medicine, 98 sustained release of a drug, 99 elevating drug serum half-life, making eliminating bacteria possible even at low doses of medicine, consistent and uniform dispersion in the site of action, and reduced side effects of medicines20,141 that put NPs in the solution list of antisuperbug approaches. Moreover, nanodrug carriers can be used depending on disease-specific conditions to evade such conditions and successfully target the infective agent. In the case of CF, there are three notable biological barriers, including high mucus density in the lungs, formation of biofilm by infecting bacteria, and intracellular infection by some pathogens in the way of effective antibacterial therapy against bacterial infections.142,143 To bypass these barriers, liposomes, polymer NPs, nanostructured lipid carriers, and nanodrug crystals are the most critical carriers that have been used in pulmonary delivery of encapsulated antibacterial agents by dry powder inhalers (Fig. 3).144,145
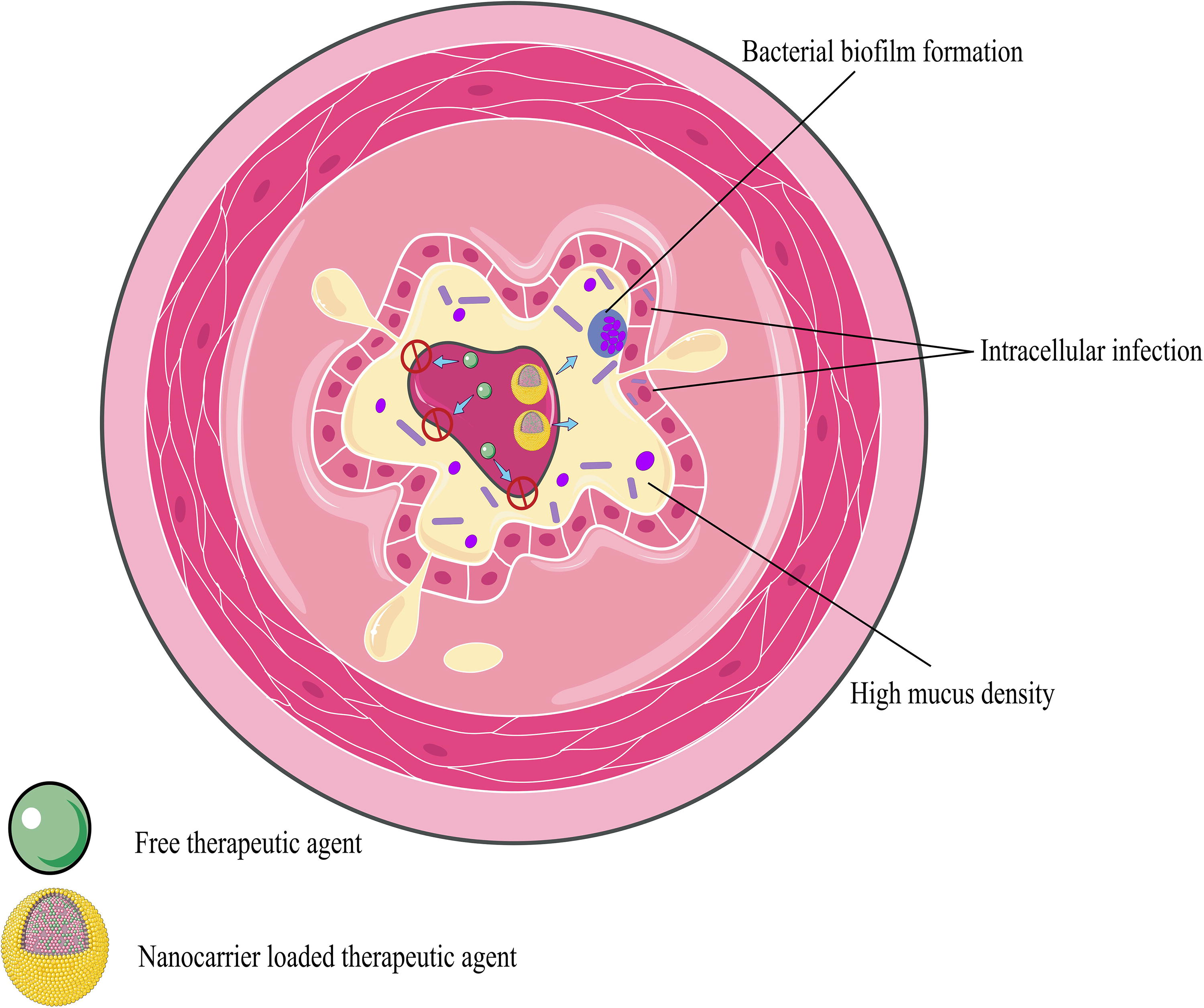
Notable barriers to CF patients’ bacterial infection cure. The biofilms formed by pathogenic bacteria, intracellular infections, and the dense consistency of mucus contribute to the complexities encountered in effectively treating these infections. Nevertheless, utilizing nanocarriers for precise delivery of the desired therapeutic substance to the site of infection is a valuable approach. CF, cystic fibrosis.
Liposomes are one of the NPs used to deliver phage cocktails and enhance their efficacy over free ones. 146 Polymer NPs such as poly(lactic-co-glycolic acid) 147 and hydrogels, including sodium alginate hydrogel and carboxymethylcellulose hydrogel for encapsulation of phages, have also been evaluated in previous studies. 148 The studies’ promising results are one step closer to the highly efficient target delivery of phages for drug-resistant infections.
Phage–probiotic combination therapy
In the modern era, probiotics have become more popular and are being more successfully marketed. 26 Bifidobacterium and Lactobacillus genera, as well as Lactococcus species, Streptococcus thermophilus, Escherichia coli Nissle 1917, and Saccharomyces boulardii, are the most commonly used microorganisms as probiotics. 24 Probiotics can boost the immune system, prevent dysbiosis, 26 show antibacterial activity alone or in combination with other antibacterial agents, 149 and increase patients’ quality of life. 150
Phage and probiotic combination can be an alternative antibacterial solution for three reasons. First, phages are highly specific and do not negatively impact commensal bacteria or probiotics; in some cases, they can improve probiotics’ function. 151 Second, combining phages and probiotics can enhance the antibacterial activity of probiotics and phages. 152 Third, in addition to antibacterial activity, some probiotics can restore the proper balance of the gut flora by elevating intestinal acidity and inhibiting the growth of several harmful bacteria. 24 By using several mechanisms of action, the combined phage–probiotic therapy approach helps avoid acquired resistance by making it more difficult for bacteria to establish resistance simultaneously. Probiotics, for instance, can prevent the growth of pathogens by competitive exclusion, the synthesis of antimicrobial compounds, and the augmentation of host immune systems, whereas phages directly lyse microorganisms. Therefore, probiotics can be a promising composition to phage combination therapies and a proper supplementary material to increase patients’ quality of life. Various investigated phage combination therapies and examples are provided in Figure 4 and Table 2.
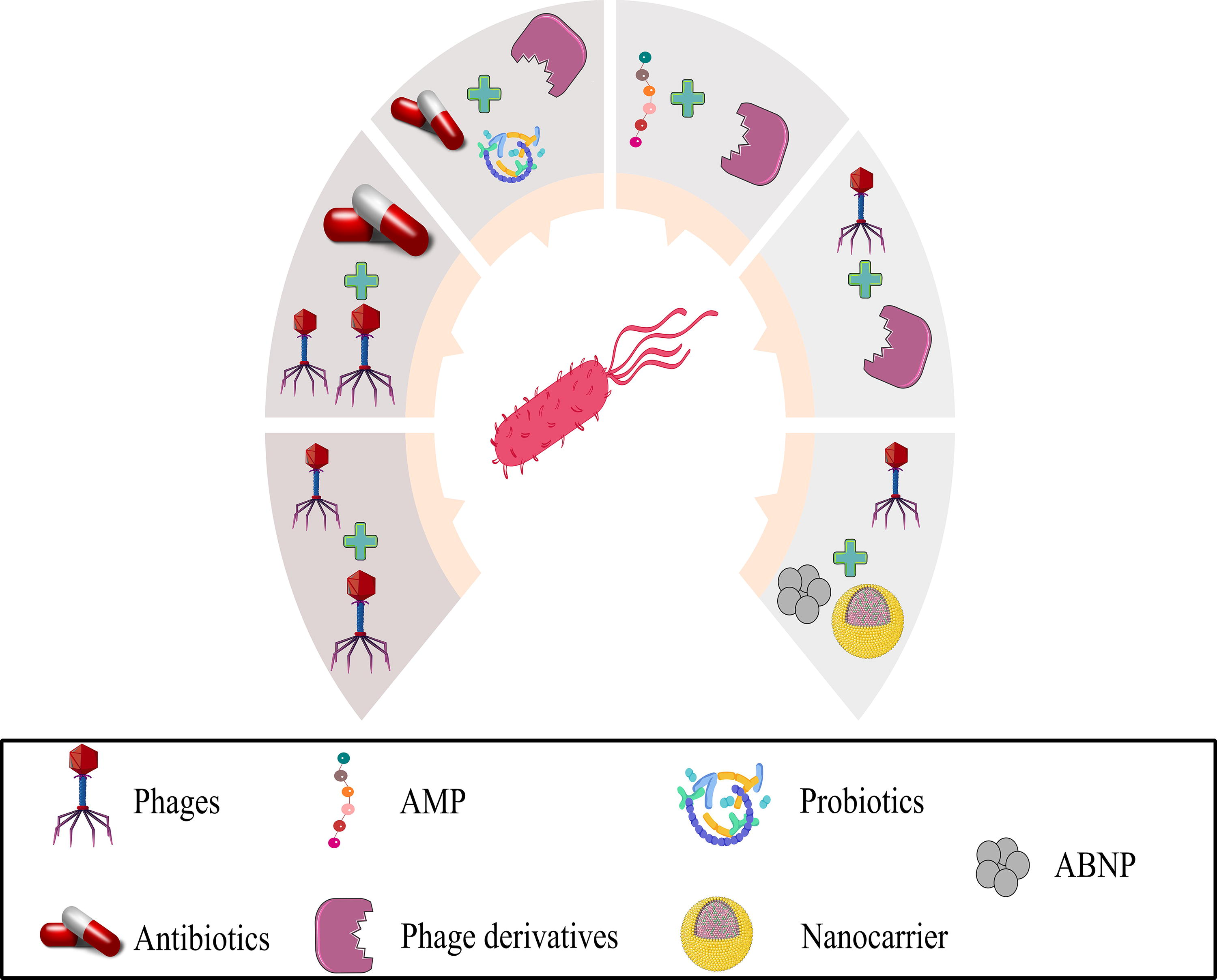
Various combination therapies in the case of combating antibiotic-resistant bacteria.
Examples of Phage or Phage Derivative-Based Combination Therapy
Prospects of Combination Phage Therapies
According to the studies that assessed the efficacy of combination therapies, the complementary components that affected a common target together or had direct or indirect antibacterial activity increased the effectiveness and synergism (Fig. 5). For instance, a combination of KP15, KP34p57, and ciprofloxacin shows the highest antibiofilm activity. 118 On the contrary, using phage cocktails can be a proper example of standard target components, and probiotics are among the components that can have direct or indirect antibacterial activity. In addition to any combination therapies assessed in previous works, many other combinations can still be evaluated in future studies to achieve the most proper medicine against MBIs. Agents such as aptamers, spanins, mAbs, and CRISPR-based therapeutics also may hold significant potential for investigation as combination therapies. By investigating their combined effects with the previously stated agents, scientists might discover the possible antibacterial efficacy of these agents.
Complementary mechanisms of action to combat persistent polymicrobial infections.
Spanin-based combination therapies
As a phage-encoded protein, there is a lack of information about the antibacterial activity of these proteins due to the possible inactivity of spanins with the presence of peptidoglycan meshwork. 84 Notwithstanding, owing to the potential of spanins to fuse with other proteins, 168 it seems that a fusion of spanin with endolysin and holin can enhance the antibacterial activity of the components on account of the antipeptidoglycan activity of endolysin and holin. Fusion of spanin with AMPs with antipeptidoglycan activity (e.g., oritavancin, nisin, ramoplanin, and friulimicin 169 ) or using spanins as an adjuvant to an antipeptidoglycan antibiotic such as β-lactam antibiotics 170 can be a proper option. Hence, exploring the potential fusion of spanins with other proteins such as endolysin, holin, or AMPs, as well as utilizing spanins as an adjuvant to antipeptidoglycan antibiotics, could offer promising options for enhancing the antibacterial activity of these approaches.
Phage-target-specific therapeutic combination
Aptamers, CRISPR-based therapeutics, and mAbs are target-specific therapeutics with high-potential antibacterial activities. Aptamers are synthetic RNA or ssDNA oligonucleotides that are incredibly organized and bind to their corresponding targets with high affinity and specificity. 171 Aptamers’ antibacterial features consist of neutralizing bacterial toxins, depolarization of cell wall, biofilm formation inhibition, opsonization, controlling the propagation of pathogen bacteria, inhibition of antibiotic resistance genes, attachment to the cell surface, and degradation and blocking antibiotic resistance enzymes.172,173
mAbs are target-specific laboratory-produced antibodies cloned from single immune cells. 101 These types of medicines can have an antibacterial effect by neutralizing bacterial toxins by blocking their binding to host cell receptors, ADCC, opsonophagocytosis, inhibition of bacterial virulence factors,22,23 and antibiofilm activity. 174
The biofilm inhibitory potential of aptamers and mAbs is a marvelous feature that can combine with depolymerase to achieve high antibiofilm activity and provide accessibility to other therapeutics. Also, it seems the studies that can build on the inhibition of resistance genes by aptamers and, in parallel, use antibiotics as combined therapy have become attractive. In the case of the other antibacterial activities of mAbs and aptamers, it demanded further studies to evaluate the feasibility of mAbs and aptamers as combined therapy with phages and uncover any possible antagonistic effects between them and phages or other substances.
The CRISPR-Cas system-based therapeutics’ antibacterial activity cleaves the pathogen’s virulence factor and antibiotic resistance genes. 11 These types of medicine are typically delivered by phages or phage-related agents such as phagemid or genetically modified phages. In addition, encapsulation of phage to deliver CRISPR-related agents into the infected cells by intracellular pathogens and CRISPR-Cas bearer plasmid can be suitable for this manner. 175 The proper delivery of these therapeutics is pivotal to achieving highly efficient medicine, and the role of phages in this manner is undeniable. When it is clear that CRISPR-Cas system-based therapeutics have high potential in combating drug-resistant bacteria, especially their gene editing potential to eliminate resistance genes in target bacteria, efficient delivery of these therapeutics is still a big concern because, without efficient delivery, target bacteria remain unharmed. 176 Hence, it is crucial to wipe out barriers such as biofilms in the way of CRISPR delivery systems to achieve highly efficient antibacterial compounds, and it is not possible without using previously discussed antibiofilm agents in combination with CRISPR-Cas system-based therapeutics.
Current Gaps and Future Perspective
According to the current resistance status, the emergence of MBIs and future antibiotic resistance prospects, utilizing combination therapies, is inevitable. Nevertheless, there needs to be more information about the exact mechanism of action and antibacterial activity of spanins, holins, and pinholins alone or in combination with other agents. Moreover, various combinations, such as targeted molecular therapeutics with phages or phage derivatives, antibiotics, and ABNPs, are yet to be assessed. Another huge gap in combination therapies is the lack of in vivo studies that make these types of therapy not reliable enough. In the case of CF, the need for proper in vivo models with CF-mimicking characteristics 177 is another issue that must be addressed in future studies. Furthermore, regulatory and ethical challenges related to these therapies are another difficulty scientists may face. Thus, to gain acceptance as a treatment for combination therapy, appropriate regulatory requirements must be created, and ethical concerns must be resolved.
Identifying any single bacterial species or subspecies associated with MBI, identifying any confounding factor such as biofilms or high mucus density, and choosing proper agents as combination therapies according to the situation are pivotal to achieving a highly efficient combination therapy. While these therapies are considered practical therapeutic approaches, performing the mentioned steps can be time-consuming. Therefore, the following steps must be taken: using sophisticated novel tools to reduce the time of these processes.
The emergence of artificial intelligence (AI) is evolving and revolutionizing life sciences. AI tools have a high potential for predicting infection occurrence, 178 biofilm occurrence, choosing antibiofilm agents, 179 and discovering new antibacterial agents, 180 developed or developing. Also, AI can play a significant role in choosing the optimal therapeutics for patients in personalized conditions. 181 With increased data from biofilm formation chemicals, infection occurrence percentage, and interaction of various antibacterial agents with their target, the AI tools grow and will be more accurate than ever. In addition, developing AI tools that can design proteins that never existed 182 and predict biofilm chemicals developing proteins with antibiofilm activity will be available soon.
To put all this together, AI will accelerate the discovery of new treatments and brighten the future of biological sciences. In particular, AI will diagnose infections, recommend possible combinations of treatments based on the properties of the agents, and even create new protein designs with antibacterial activity for use in mono or combination treatments. AI can speed up identifying therapeutic combinations that work, cutting down on the time needed for experimental validation, and enabling the creation of novel medicines. It is expected that AI will play a vital role in the advancement of therapeutics as we advance, especially in the areas of combination therapies and phage therapy. The future of biomedicine will not just be based on combination therapies but also on combination AIs, servers, and robots to combat complex infections that will threaten humans’ future.
Conclusion
In the modern era, AMR in bacterial pathogens is a significant hygiene problem in the developing and developed countries. Since these pathogens resist antibiotics, fighting against these bacteria requires alternative therapeutic approaches. Hence, many alternative approaches have been investigated by researchers to deal with antibiotic-resistant bacterial pathogens in recent years.
Therapeutic agents based on mAbs, CRISPR technology, nanotechnology, probiotics, aptamers, AMPs, and phages have shown promising results. Despite phage utilization as a planktonic form, phage derivatives are also considered a promising alternative therapeutic approach due to their broad-spectrum antibacterial activity compared with planktonic phages. Enhancing the efficacy of phages or phage-relative derivatives, especially in treating MBIs, is another challenging phage therapy case. The easiest and most applicable method for addressing this challenge is combination therapies. However, most combination therapies are limited to phage cocktails, phage with antibiotic combination, and endolysin with antibiotics, and the other combined methods are limited to the in vitro efficacy evaluation studies or need more reliable data. Hence, subsequent investigations must expand our understanding of phage combinations beyond the widely recognized phage–antibiotic approach. To create comprehensive and robust treatments against drug-resistant bacterial infections, we must investigate the synergies and possible antagonists among multiple therapies. The combination of phage and antibiotics continues to be a mainstay of current research efforts in this sector, even though it is impossible to conclusively determine which technique has the highest or most minor potential efficacy due to a lack of evidence in other combination therapies.
In conclusion, the use of phage therapy has a long way to go until it is accepted as a universal drug against antibiotic-resistant bacteria since there are many challenges facing this type of treatment process currently. Notwithstanding, recent clinical studies have brought phage therapy closer to the market in Western countries. The use of phage derivative agents or combination therapies is in the early stages of research, and except for endolysins, which have been studied in vivo, other methods are currently undergoing the in vitro process. Meanwhile, with the continuation of in vitro research, many questions arise about various aspects of combination therapies, leading to a more protracted process of their acceptance as the primary treatment.
Footnotes
Acknowledgments
Authors’ Contributions
All authors contributed to the study’s conception and design. M.R.: Conceptualizing and writing and reviewing the original draft. D.J.-G. and E.M.: Writing and reviewing the original draft. N.Z.: Reviewing and editing the original draft and supervising. All authors read and approved the final article.
Disclosure Statement
The authors declare that they have no known competing interests.
Funding Information
No funding was received for this article.