
Abstract
Introduction
OM results from radiation-induced mitotic death of the mucosal epithelium basal cells, usually approximately 2 weeks after the beginning of radiotherapy, when an irradiation dose of approximately 2,000 cGy is used. OM is dose-limiting and may lead to interruption or alteration of treatment, interfering with disease prognosis. 4 –6
The use of both radiotherapy and chemotherapy highly increases the incidence of OM, accounting for 80% to 100% of cases. Forty percent of all patients undergoing chemotherapy will develop some level of mucositis, the incidence being even higher when associated with radiotherapy, 5 although previous evaluation of buccal condition and follow-up by a multidisciplinary team during cancer treatment may minimize damage caused to buccal tissues. 7,8
The use of laser therapy has proved to decrease OM intensity in patients undergoing radiotherapy and chemotherapy, as an associated therapy or as an isolated therapy. 9,10 Additionally, preventive laser therapy is advisable because it can trigger a sequence of tissue reactions linked to cellular homeostasis, resulting in cellular metabolic rate increase, higher collagen synthesis, DNA and RNA production and beneficial effects on the immune system. 9
Also, laser therapy seems to increase the formation of capillaries, the liberation of growth factors, and leukocyte activity, which in turn inhibit or reduce the toxic effect of radiotherapy and chemotherapy. The objective of this study was to evaluate prospectively, quantitatively, and qualitatively the effect of diode laser (λ = 660 nm, power = 30 mW, energy = 2 J per point) in the prevention and treatment of OM in patients suffering from head and neck cancer undergoing radiotherapy and chemotherapy.
Materials and Methods
Ethical aspects
This research was performed in compliance with resolution 196/96 of the National Health Counsel of Brazil and was submitted to the Ethics Committee of the Cancer Hospital of Mato-Grosso and of the Vale do Paraiba University. Informed consent was obtained in accordance with the Declaration of Helsinki.
Inclusion criteria
The criteria for inclusion in the study were aged 18 and older, oral mucous intact on the first day of the experiment, and capacity to cooperate with the treatment. Patients must also have signed informed consent.
Exclusion criteria
Patients who did not meet the inclusion criteria, patients who were receiving drugs for the treatment or prevention of mucositis, and patients who the authors did not previously evaluate and release were excluded from this study.
Characterization of sample
A multidisciplinary team of dentists, physicians, physical therapists, dieticians, speech therapists, and psychologists conducted this clinical study. Volunteer patients of both sexes (60 men and 12 women), with no distinction of race or social class and aged 34 to 80 were selected. All volunteers had head and neck cancer and underwent radiotherapy and chemotherapy. Seventy-two individuals fulfilled the study requirements and were divided into two groups: one that received laser treatment (L; 31 men, 5 women) and a control group that did not receive laser treatment (C; 29 men, 7 women). Data about location, type, and clinical stage of cancer were collected.
Data collection
The first contact with patients was an interview in which they signed the “Term of Consent and Clarification,” which guaranteed their anonymity. All volunteers were submitted to adequacy of buccal cavity before receiving treatment. Following the Cancer Hospital of Mato-Grosso protocol, all adult patients with head and neck epidermoid cancer received weekly sessions of chemotherapy (including cisplatin 70 mg/m2 and a radioisotope) plus daily sessions of radiation (medium daily dose of 1.8gy) except on weekends and holidays. During radiotherapy sessions, teeth were protected with a silicone tray containing neutral fluoride gel to protect the enamel from radiation, avoiding demineralization once xerostomy and inclination for infection were inevitable.
Data were collected through daily physical intraoral examination, and evaluation of OM was made according to the association of three criteria: National Cancer Institute (NCI) criteria, Brown scale to evaluate the incidence of OM, and the Visual Analog Pain Scale (VAS).
Laser application
A trained technician, who performed the procedure following standard techniques, performed laser irradiation. For laser therapy, a diode laser (aluminium gallium indium phosphide; Bio Wave-Kondortech, São Carlos, Brazil, λ = 660 nm, power = 30 mW, spot size = 2 mm, continuous mode) was used. Energy used was at 2 J per point or scattering on the affected area with 1 cm2 per application point. The affected area received irradiation in different points in contact mode. Irradiated regions were as follows: three points on jugal mucosa, three points on inferior lip internal mucosa, three points on soft palate, two points on palatine folds, two points on sublingual caruncles, and five points on the tongue. Applications were done twice weekly, before or after radiotherapy sessions.
Statistical analysis
Analysis of variance with a significance level of 0.05 was performed considering the group effect (with and without laser) and the moment effect (day 1 and weeks 1, 2, 3, 4, 5, 6, and 7) for the three criteria used (NCI, Brown, and VAS). In the case of significance of group or moment effect, multiple comparisons of minimal squares were used to identify the difference between the variables.
Results
Profile of patients
The location of cancer in the patients and its distribution in the C and L groups are described in Table 1. Of the 72 patients analyzed in this study, 61.2% had clinical Stage IV, 17.2% had clinical Stage III, 20.4% had clinical Stage II, and 1.2% had clinical Stage I of the disease; 86.6% of the patients underwnet surgery for tumor removal during or after this study.
OM evaluation according to the NCI scale
The results of evaluation according to the NCI scale can be found in Figure 1. Comparing the two groups, statistically significant differences were observed from the first week on (p < 0.001). Patients in group L did not present differences in the oral aspect during the experiment (p = 0.41) with an increase in the NCI scale results being observed during week 4 (p = 0.01) and returning to normal the following week. All patients in group C had OM levels varying from I to III on the NCI scale. This difference was significant from week 1 on (p < 0.001), increased until week 4 and then remained stable up to week 7 of the cancer treatment (p = 0.68).
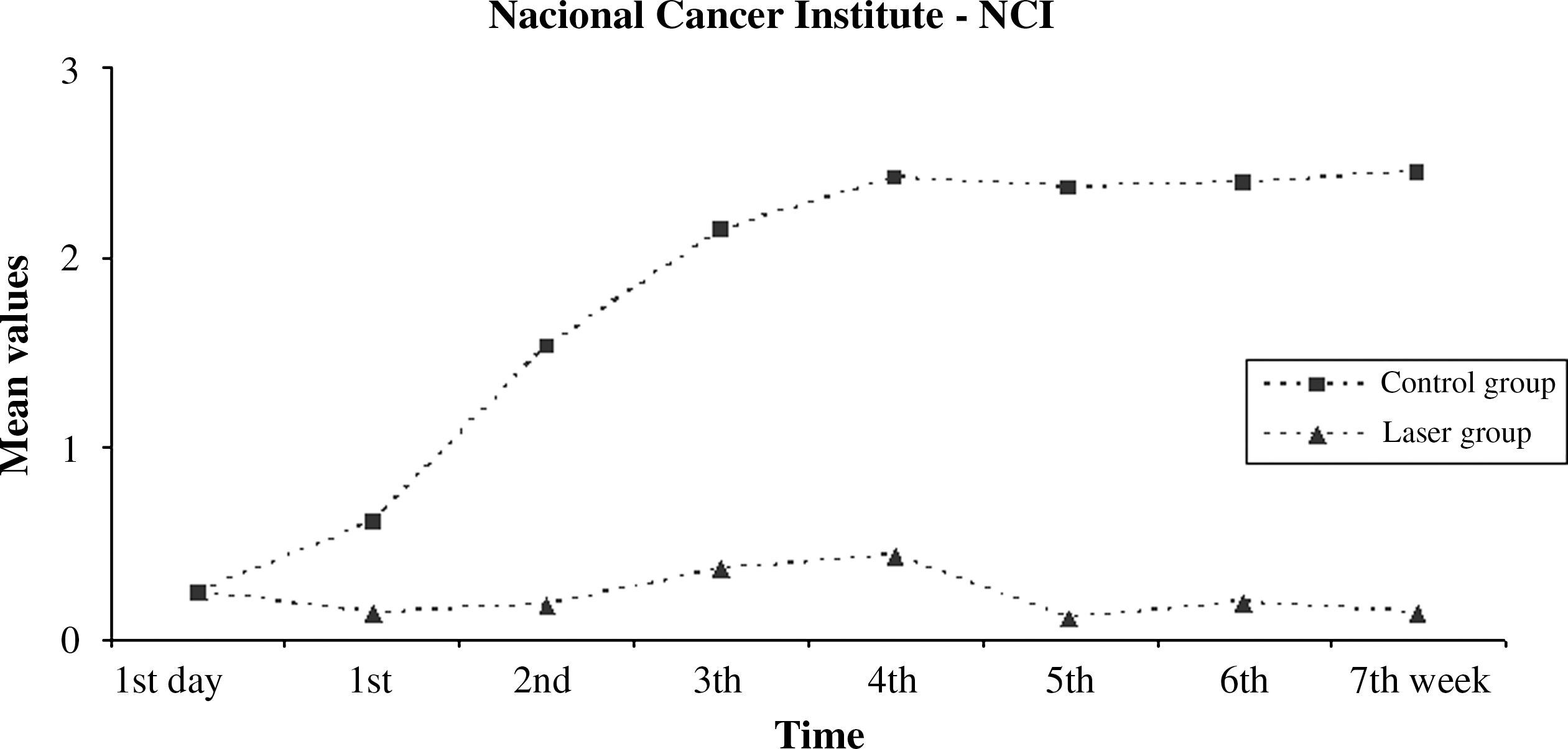
Oral mucositis evaluation according to the National Cancer Institute (NCI) scale during the experimental period.
OM measurement according to the Brown scale
Differences in OM results between the two groups was also significant when the Brown scale was used (p < 0.001). The absence of significant differences with the Brown scale results found in group L during the experimental period (p = 0.42) suggests that laser therapy was successful in preventing and controlling OM lesions. In the control group, OM incidence increased from week 1 until week 4 (p ≤0.001), remaining stable up to week 7 (p = 0.17), with moderate to severe OM lesions being observed (Fig. 2).
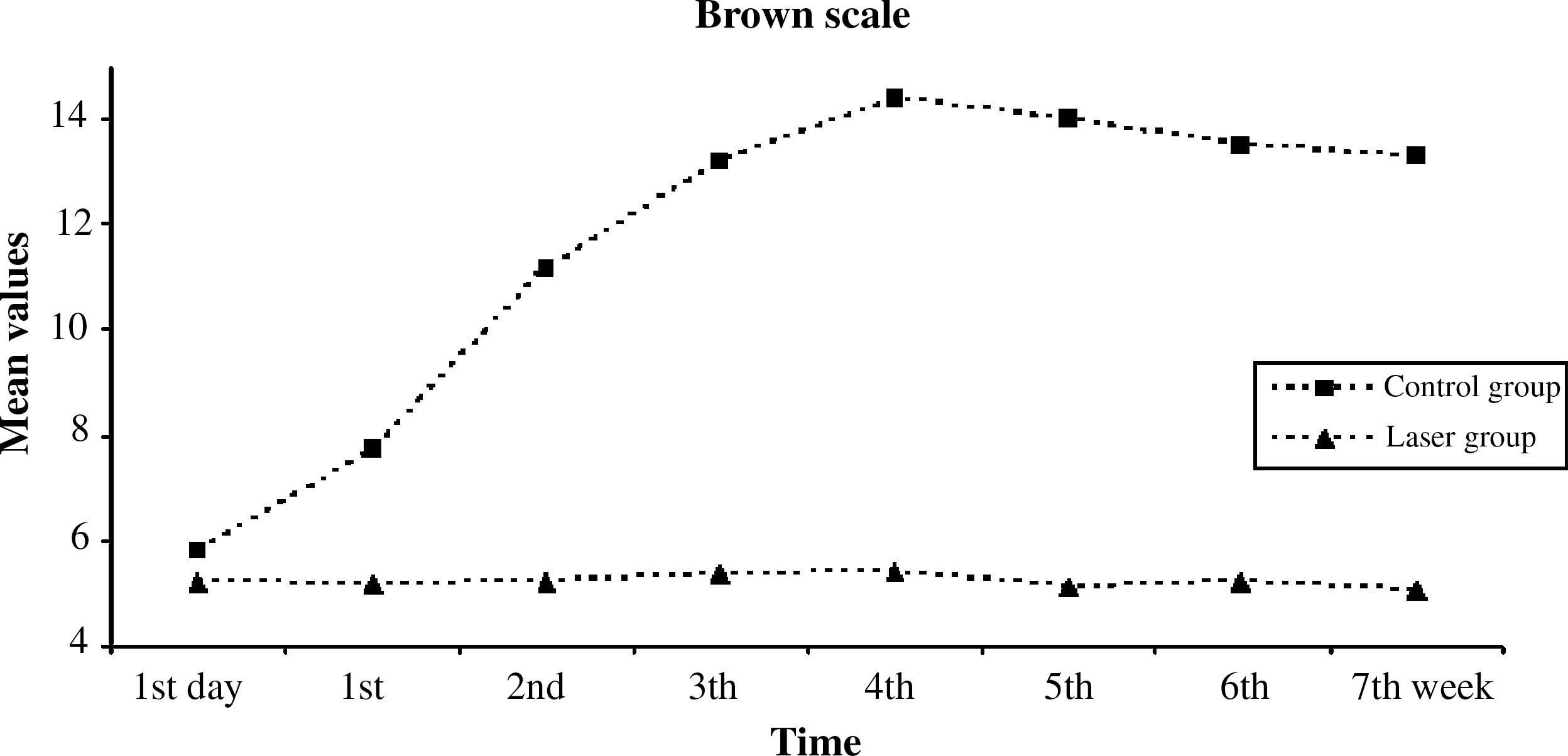
Oral mucositis evaluation measurement according to the Brown scale during the experimental period.
Pain evaluation according to the VAS
The VAS results can be found in Figure 3. As previously described, comparing the groups, statistically significant differences were observed from the first week on (p = 0.02). Also, according to the VAS, patients in group C presented increasing indexes of pain from weeks 1 to 4 (p = 0.008), remaining constant to week 7 (p = 0.44), whereas patients in group L reported absence of pain during the entire cancer treatment (p = 0.05).
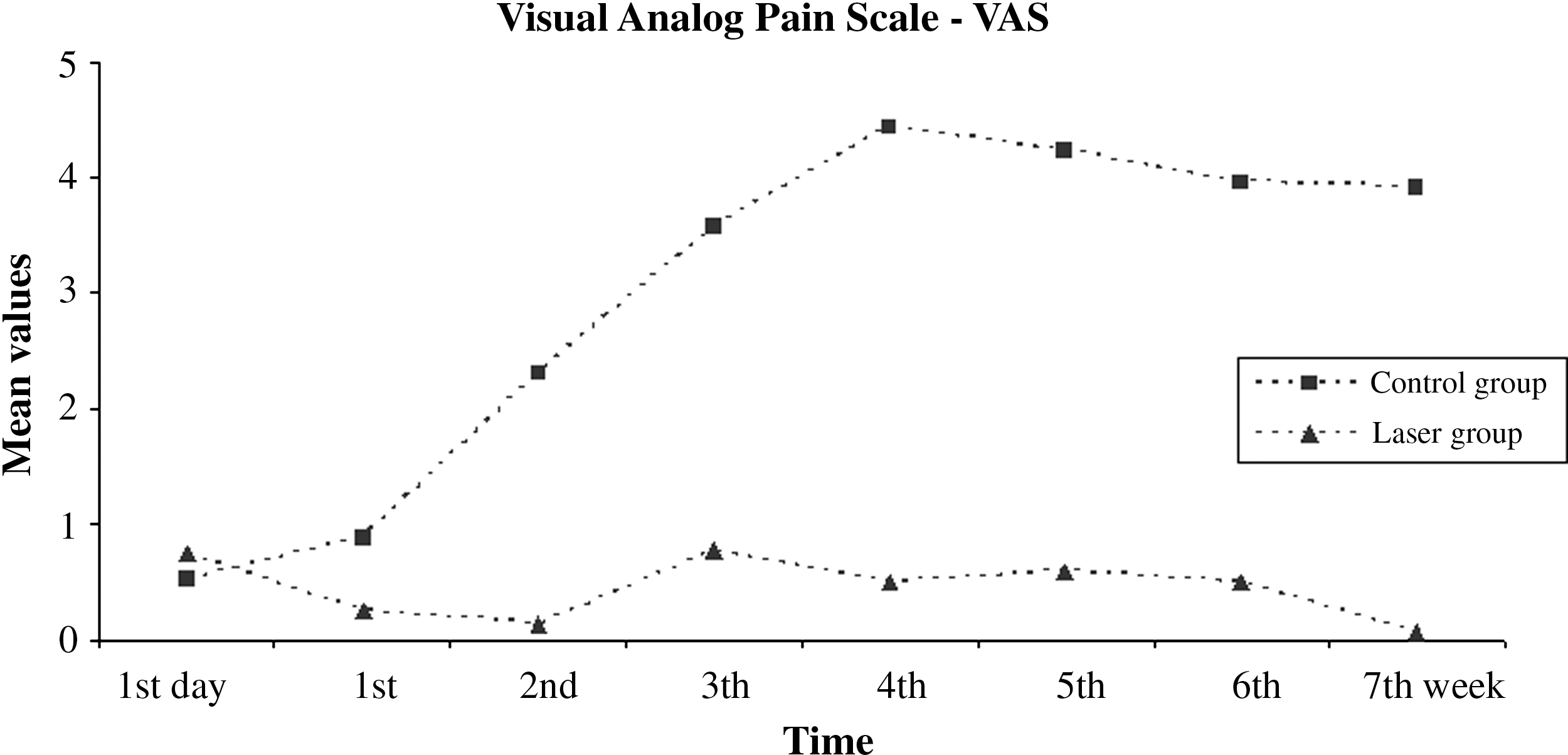
Pain evaluation according to the Visual Analog Pain Scale during the experimental period.
Comparative analysis of NCI and Brown scales
Figure 4 illustrates the comparative analysis between the NCI and Brown scales, in which the agreement between the OM evaluation and measurement results found in this study can be observed (p < 0.001).

Comparative analysis of oral mucositis evaluation (NCI scale) and measurement of lesion (Brown Scale) observed in this study (p ≤ 0.001).
Discussion
The quality of life of patients with cancer has long been discussed. Moreover, the treatment of head and neck cancer is mutilating, and the effects of radiotherapy and chemotherapy are unpleasant. Tadiobiological or toxic products cause radiotherapy-induced mucosal lesions associated with cancer treatments. Thus, the diverse microbiota living in the mouth can lead to development of infection caused by bacteria, fungi, and viruses from indigenous microbiota. 11
Laser therapy is based on nonthermal mechanisms (≤1°C) of light on biological tissues, and its use in the prevention and treatment of mucositis induced by antineoplastic treatment has presented promising results, especially in clinical studies. 12 –15
First, we determined irradiation parameters and energy of 2 J per point. Bensadoun 16 analyzed the use of helium-neon (He-Ne) laser in the prevention of radiotherapy-induced OM in 30 patients in a prospective randomized manner. Our study had a larger number of patients (n = 84), and qualitative and prospective analyses with detailed procedures were performed. Also, calculation of energy per point in the area of irradiated tissue is more appropriate for laser therapy calculations when there is scattering of light in the tissue. 17
Because of decreasing immunity and increasing OM as a result of cancer treatment, some patients in group C undergoing radiotherapy associated with chemotherapy had the antineoplastic treatment temporarily suspended. This did not occur in group L. Although Lopes 8 provided daily laser applications during radiotherapy, the authors suggested that, in the future, three weekly sessions should be provided. In this study, two weekly applications were performed because of the difficulties of volunteers in returning more frequently for laser treatment.
While studying the beneficial effects of laser therapy as a prophylactic treatment method, many authors have performed studies with patients likely to develop OM, such as those undergoing conditioning for bone marrow transplant and radiotherapy and chemotherapy for head and neck tumors. 1,3,9,18,19 Similarly, statistical data in our studys showed that patients receving laser treatment in association with radiotherapy and chemotherapy had a lower incidence of OM and pain.
Bensadoun 14 and Lopes 8 evaluated the prophylactic application of laser and observed that a decrease in OM was significant. In this study, laser was also applied preventively, because laser irradiation started at the beginning of radiotherapy and chemotherapy. Results obtained were positively significant (p < 0.05), corroborating the above-mentioned findings.
Thus, Lopes 8 observed that, in the group treated with radiotherapy and laser, all patients completed the planned radiotherapy treatment, whereas in the untreated group, 13.8% of patients had to interrupt their treatments because of decreased immunity provoked by secondary asthenia and deglutition difficulties. This observation is in agreement with Balakirev et al., 3 who concluded that interruption time to treat complications resulting from radiotherapy and chemotherapy in pediatric patients was reduced up to two times in the group receiving laser therapy. Our results are in agreement with Lopes 8 and Balakirev et al., 3 because in group C, 15 patients needed to interrupt radiotherapy treatment, whereas in group L, no patients interrupted radiotherapy or chemotherapy sessions.
The results obtained in this study and in literature reviews showed the improvement in the quality of life of patients with cancer receiving laser therapy in association with radiotherapy and chemotherapy. OM, pain, dysphonia, and dysphagia were minimized with laser therapy. Thus, benefits and improvement in quality of life observed in patients receiving laser therapy justify the adoption of this therapy associated with conventional cancer treatment.
Conclusion
A 660-nm diode laser, within the parameters used in this study, was effective in the prevention and treatment of OM in patients undergiong radiotherapy and chemotherapy treatment, providing them more comfort and a better quality of life.
Footnotes
Author Disclosure Statement
No competing financial interests exist.