
Abstract
Introduction
Laser treatment has been proposed as a possible alternative to acid etching to achieve reliable bond strengths. Laser application removes the smear layer and produces a wide variety of surface textures with increased surface area and roughness. Several studies on the bond strength between resin and laser-treated dentin have been performed using Nd:YAG 4,5 and Er:YAG lasers, 6 –13 which are commercially available for dental practice. When applied to dentin, Er:YAG laser radiation is preferentially absorbed by water because its radiation wavelength (2.9 μm) is within an important absorption band of water. This leads to explosive water evaporation and thermo-mechanical ablation. Intertubular dentin is preferentially ablated, due to its higher organic and water content, and the laser treatment leads to the formation of a smear-layer-free, highly fractured surface with exposed dentinal tubules. 7,14 Collagen may be denatured, 7,15 thus limiting hybrid-layer formation 6 and reducing the resulting bond strength. Recent studies reveal that Er:YAG laser treatment has an adverse effect 6 –11,13 or no effect at all 8,12 on resin–dentin bond strength, and these results were also affected by the composition of the tested adhesive system.
Recent studies performed on dentin surface texturing after treatment with KrF excimer laser, 16,17 revealed that, when fluences higher than the ablation threshold (0.5 J/cm2) and up to 1 J/cm2 are used, a cone-like surface topography is produced by preferential ablation of intertubular dentin. Due to the higher absorption coefficient of collagen compared to hydroxyapatite, the organic phase (collagen fibers) is preferentially removed, leaving a superficial layer of resolidified hydroxyapatite. 16 This cone-like structure increases the surface specific area, 18 which may potentially improve the bond strength between dentin and adhesive restorative materials.
The purpose of this study was to compare the resin–dentin bond strengths achieved by treating dentin with KrF laser and conventional phosphoric acid etching or a combination of both conditioning techniques. The null hypothesis tested is that there are no differences in the surface topography of acid-etched, laser-treated, or laser-treated/acid-etched dentin, nor in the microtensile bond strengths (MTBS) achieved when bonding with an etch-and-rinse self-priming adhesive.
Materials and Methods
Twelve caries-free human third molars were stored in 0.1% thymol solution and used within 1 mo following extraction. The specimens were sectioned below the dentino-enamel junction and ground (180 grit) under running water to provide flat, smear-layer-covered dentin surfaces. The teeth were randomly divided into three groups. In group 1, dentin surfaces were etched with 35% phosphoric acid (3M ESPE, St Paul, MN) for 15 s, rinsed with deionized water for 30 s, and blotted dry with tissue paper. In group 2, the dentin was treated with KrF excimer laser radiation (λ = 248 nm, pulse duration 30 ns) using a radiation fluence of 1 J/cm2 and 100 laser pulses at 5Hz. The laser beam was kept perpendicular to the sample surface and shaped by inserting a square aperture mask into the beam path to select its central area, where intensity is fairly homogeneous. The mask was then optically projected onto the specimen surface by means of a 100-mm focal-length lens. In order to get 3 mm2 treated surfaces, spots 400 μm wide by 500 μm long were consecutively treated and overlapped by 10%. In group 3, the laser treatment (carried out as described for group 2) was followed by acid etching according to the procedure described for group 1.
Two samples from each of the previously described groups were prepared for scanning electron microscopy (SEM) observation. The conditioned samples were immediately fixed by immersion in 2.5% glutaraldehyde for 12 h at 4°C. After fixation, the samples were dehydrated in ascending grades of ethanol (25% for 20 min, 50% for 20 min, 75% for 20 min, 95% for 30 min, and 100% for 60 min). They were then dried by immersion in hexamethyldisilazane for 10 min. 19 The samples were kept in a desiccator for 48 h, mounted on metallic stubs, gold-coated, and their surface topography observed by SEM (S2400, Hitachi, Japan) to analyze the morphological characteristics resulting from the different dentin treatments.
For the MTBS test, dentin–composite samples were prepared. Two remaining samples of each tested group were bonded with the etch-and-rinse adhesive (Adper™ Scotchbond™ 1 XT, 3M ESPE) applied according to the manufacturer's recommendations. Resin build-ups (6 mm in height) were constructed incrementally (1.5 mm at a time) with light-cured hybrid resin composite (Esthet-X®, Dentsply Caulk, Konstanz, Germany). Each layer of composite was light-cured for 40 s with a Translux EC halogen light-curing unit (Heraeus Kulzer GmbH, Bereich Dental, Wehrheim, Germany). The light intensity was monitored with a Demetron Curing Radiometer, model 100 (Demetron Research Corporation, Danbury, CT) at a minimum of 600 mW/cm2. After storage in distilled water at 37°C for 24 h, the composite–dentin samples were sectioned longitudinally into slabs, which were further sectioned into 1.0 ± 0.1 mm2 beams. Each sample originated at least 20 sticks.
Samples were glued to a Bencor Multi-T testing device (Danville Engineering Co., San Ramon, CA) and loaded in tension at a crosshead speed of 0.5 mm/min until failure, using an Instron 4411 mechanical testing machine (Instron Corporation, Canton, MA). After fracture, the beams were carefully removed from the apparatus and the cross-sectional area at the failure surface measured with an error of 0.01 mm with a pair of Sylvae Ultra-Call (Li) digital calipers (Fowler, Newton, MA). The bond-strength values were statistically analyzed using one-way ANOVA. Multiple comparisons were performed using the Student–Newman–Keuls test. The statistical significance level was set at α = 0.05. The failure modes recorded in each test group were evaluated under SEM. Fractured samples were dehydrated with increasingly concentrated ethanol solutions, mounted on metallic stubs, and sputter-coated with gold.
Results
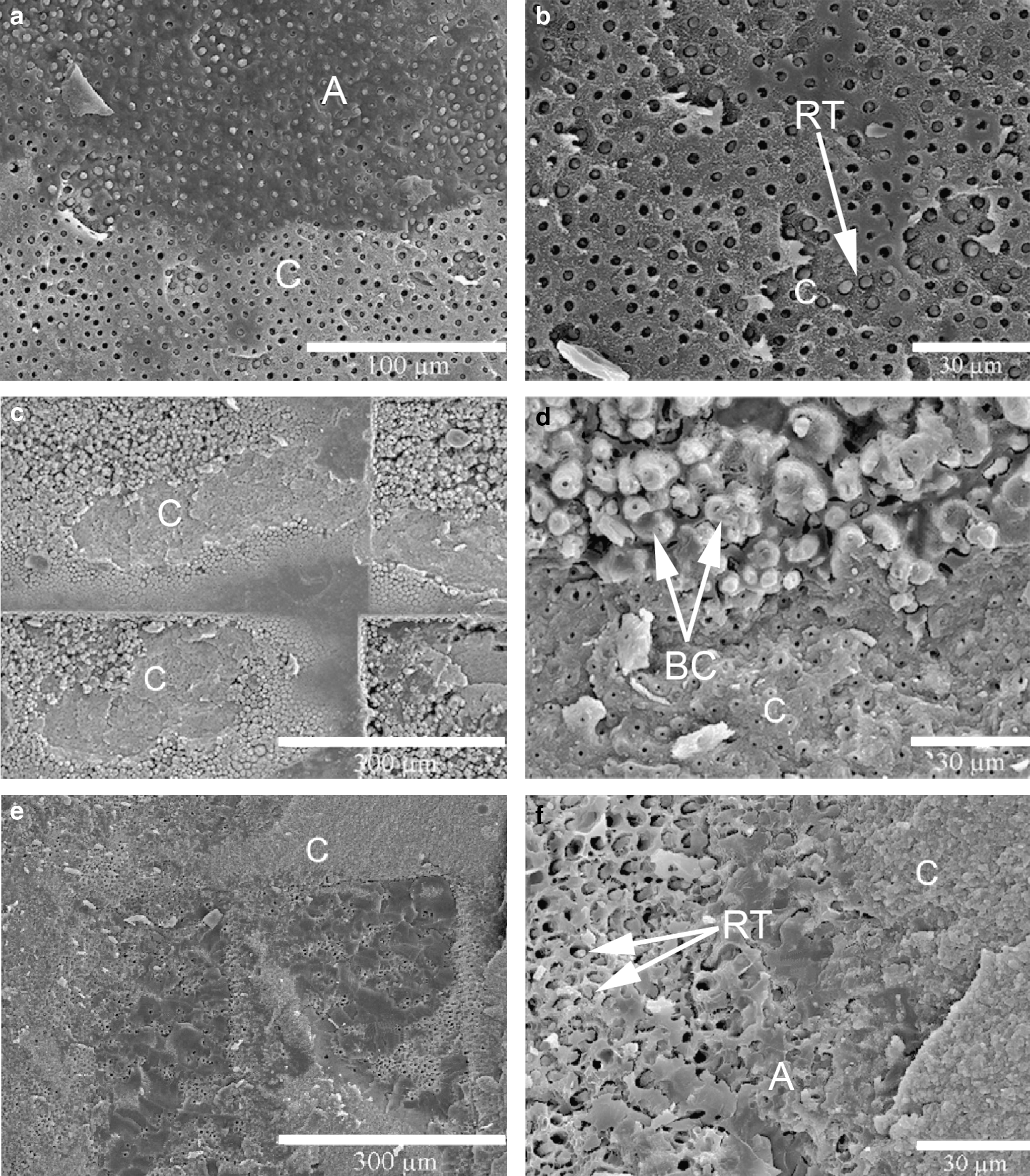
SEM images of the dentin surfaces before and after performing the three surface treatments are presented in Fig. 1. Before conditioning, tubule entrances are partially obliterated. The smear layer and smear plugs may have been partially removed by the SEM specimen preparation procedures (Fig. 1a). After 35% phosphoric acid etching, the dentin tubules are enlarged as a consequence of the partial dissolution of peritubular dentin and removal of the smear plugs (Fig. 1b). The laser treatment preferentially removed the intertubular dentin, resulting in cone-shaped formations with an average diameter at the base of 4 μm and a height of about 7 μm. These cones are formed of partially melted and resolidified peritubular dentin, with occlusion of the tubule openings (Fig. 1c). When acid etching is applied to previously laser-treated dentin, the cone topography disappears, resulting in a relatively rough surface with open dentinal tubules. Some tubule walls are protruding from the surface due to the coverage of loose angular debris of previously resolidified material (Fig. 1d).

SEM micrographs of dentin surface after (
Mean MTBS values and the respective standard deviations are reported in Table 1. The bond strength is influenced by dentin treatment (F = 32.8; p < 0.001). Conventional phosphoric acid etching leads to higher bond strengths than laser-treated or laser-treated/acid-etched dentin (p < 0.05).
Groups with different letters have statistically significant difference after Student–Newman–Keuls multiple comparisons (p > 0.05).
SEM images of fractured beams are presented in Fig. 2. After 35% phosphoric acid etching, failures were mostly mixed in nature affecting the resin–dentin interface. Areas with adhesive remnants (Fig. 2a) and dentin tubules infiltrated with resin tags (Fig. 2b) are detectable. In laser-treated specimens, evidence of neither resin–dentin interaction nor resin tags is detected (Figs. 2c and d). Fractures along the dentin surface often break cone formations at their base, while in other areas cones are broken roughly at half-height (Fig. 2d). In laser-treated/acid-etched samples, a mixed failure mechanism is observed with sparse resin tags and adhesive layer remnants. The underlying dentin surface is detectable (Fig. 2e and f).
SEM micrographs of the fracture surfaces of: (
Discussion
Hybrid-layer formation is the main mechanism involved in dentin bonding to current adhesive systems, in which resin monomers infiltrate the exposed collagen network and the opened dentinal tubules formed during acid etching to create bonding 1 . When hybrid-layer formation is prevented by deproteinization of the surface with NaOCl solution applied after acid-etching, the interfacial bond strength depends considerably on the nature of the tested adhesive and on the possible interaction with the mineral component of dentin. Depending on the adhesive system, the removal of collagen may increase, decrease, or have no effect on the bond strength, 20 –22 challenging in some cases the hybrid-layer bonding mechanism model.
Laser treatment has been widely investigated as a potential substitute or complement to acid conditioning before the application of an adhesive system. Most studies show that treatment with Er:YAG laser prevents the formation of proper resin–dentin interaction, and decreases 6,7,9,10 or has no effect 8,12,23 on the bond strength, depending on the adhesive–resin system used. The surface morphology of dentin after treatment with KrF excimer laser radiation is quite different from that obtained using Nd:YAG or Er:YAG lasers. 16,24 For the range of fluence applied in this study (≤1 J/cm2), KrF laser radiation predominantly ablated intertubular dentin, with minimal thermal damage of the underlying tissue 16 . After treatment, hollow cones of partially melted peritubular dentin stand up above the intertubular dentin surface, leading to a cone-shaped topography (Fig. 1c) with a considerably larger surface specific area and superior roughness. On the other hand, dentinal tubules are partially sealed by the cone-shaped formations. 24 In KrF laser-treated dentin, a frank resin–dentin interaction is not clearly detectable (Fig. 2d) because the laser treatment removed collagen fibers from the surface, leaving a thin film of resolidified hydroxyapatite. 16 As a result, bonding must depend on a micromechanical retention mechanism, due to the infiltration of the adhesive between the cones (Fig. 2d). However, this interaction did not provide reliable bond strengths, which were rendered susceptible to transversal fracture under load. Due to the brittle nature of the cones that are formed by hydroxyapatite, they tend to fracture during testing, justifying the lower MTBS values (13.8 ± 5.1 MPa) compared to the acid-etched dentin, where retention is obtained by the formation of a resin–dentin interdiffusion zone (33.7 ± 8.7 MPa). Depending on the degree of resin penetration between the cones, the fracture occurs at the base of the cones or at some point along their height (Fig. 2d).
The bond strength achieved on laser-treated dentin may also be influenced by the nature of the tested adhesive. When bonding to collagen-depleted dentin, it is important to achieve a proper chemical interaction by means of adhesives that contain acidic monomers with high diffusive potential and capable of reactions with hydroxyapatite, forming low solubility salts. 5,25 Although Single-Bond XT contains acidic monomers (polyalkenoic acid), its high filler content and molecular weight may have limited the diffusion through mineralized dentin. 26 Recently, 27 it has been reported that functional monomers, such as 4-methacryloxethyl and 10-methacryloxydecyl dihydrogen phosphate, present in adhesive composition can bond chemically to calcium ions in dentin hydroxyapatite and potentially improve the bond strength to dentin. Such adhesives could be more appropriate for the mineralized surface of laser-treated dentin, providing an additional bonding mechanism other than mechanical retention between the superficial cones.
When phosphoric acid etching is applied to a previously laser-treated dentin surface, the bond strength is higher (19.7 ± 6.9 MPa) than the bond strength of the laser-treated surface. Phosphoric acid partially dissolves the continuous surface film of resolidified hydroxyapatite and exposes the dentinal tubules (Fig. 2d), enabling the formation of resin tags (Fig. 2f). The fact that the MTBS values achieved are lower than those obtained after etching is probably due to the brittle nature of the surface or to the fact that the laser treatment superficially eliminates the collagen fibers, limiting the resin–dentin interaction.
The results of the present study require rejection of the null hypothesis, since differences in surface dentin topography and bond strengths have been recorded between acid-conditioned and laser KrF excimer-treated dentin.
Conclusions
Bonding of the tested etch-and-rinse adhesive to dentin treated with KrF laser radiation depends on a micromechanical retention mechanism based on adhesive infiltration between superficial cone-shaped formations. No changes in dentin substrate are detectable that may suggest a conventional hybrid-layer formation. The laser treatment does not improve the bond strength, compared to conventional acid etching.
Footnotes
Disclosure Statement
No competing financial interests exist.