
Abstract
Introduction
Osteoclast inhibition could improve the prognosis of tooth replantation; however, current therapies for tooth avulsion are only able to delay rather than inhibit the resorption process. 4 Some of these therapy modalities are based on the use of calcium hydroxide, 5 antibiotics paired with corticosteroids, 6 and calcitonin. 7 More recently, Levin et al. 4 employed alendronate, an anti-osteoclastic drug, in order to inhibit the root resorption of replanted dog teeth. This drug, a third-generation bisphosphonate with demonstrated osteoclast inhibitory activity, enhanced healing and preservation of tooth mass subsequent to replantation. 4 In our experience alendronate applied as a paste in polyethylene glycol is highly cytotoxic in vitro as well as in vivo. 8 Moreover, in direct contact with human periodontal ligament fibroblasts, it is cytotoxic at concentrations higher than 10−6 M. 9
Faced with more severe dental traumatic injuries, such as intrusion and avulsion, there is an inflammatory response that causes resorption of damaged tissue. Damage to the PDL, due to mechanical trauma, dehydration, or other causes, affects the viability of PDL cells and worsens the prognosis for teeth replantation. 1 –3 Moreover, the resorption process, which is directly associated with the PDL inflammatory response, exposes dentin and promotes direct communication with the pulp through dentinal tubules, allowing bacteria and their toxic products to reach the external dental root surface. 1 –3 This can perpetuate the external inflammatory process. Thus, it is important to find a therapy able to block this mechanism by sterilizing the root surface and making it impermeable to bacteria and toxins.
Besides sterilization, the biocompatibility of the replanted root surface is also critical to avoid perpetuating the external inflammatory process. Laser irradiation has been reported to exhibit bactericidal and detoxification effects without producing a smear layer, and the laser-treated root surface may therefore provide favorable conditions for the attachment of periodontal tissue. Of the different lasers available, Nd:YAG laser is bactericidal 10 and when applied prior to tooth replantation could reduce the susceptibility to resorption. 11
We have studied the biocompatibility of human dental root treated by Er:YAG laser 12 and diode laser 13 ; however, little is known about the biocompatibility of Nd:YAG laser–irradiated root surfaces. Thus, the aim of this study was to analyze the in vivo biocompatibility of dental root surfaces previously irradiated with Nd:YAG laser and then implanted into rat subcutaneous tissue.
Materials and Methods
In vitro assay (dental root preparation)
After the approval of the Ethical Committee of the University of São Paulo, 48 freshly extracted human molars were used. In order to simulate an in vivo clinical situation of dental avulsion followed by replanting, these teeth were extracted and immediately used for the experiments. Moreover, no sterilization process were used. The use of freshly extracted teeth was important in order to standardize the time post-avulsion of each dental root treatment. The disto-buccal roots were cut below the enamel cement junction perpendicularly to the root long-axis in order to get a 10 mm long dental root. Each dental root canal was endodontically prepared with manual files (up to a no. 40 size) and 2.5% sodium hypochlorite in a crown-down fashion, until obturation. This endodontic treatment was done in hydrated roots hold manually following all the aseptic conditions of an in vivo treatment. These nonsterilized roots were then randomly divided into four experimental groups (n = 12 dental roots per group).
Experimental groups
The four experimental groups were 1) G1 dehydrated, in which specimens were maintained dry for 3 h prior to implantation; 2) G2 NaF, in which specimens were maintained dry for 3 h followed by soaking in a 2.4% acidulated sodium fluoride solution (pH 5.5) for 20 min and further washing in physiological serum prior implantation; 3) G3 hydrated, in which specimens were maintained in physiologic saline solution for a minimum of 72 h prior to implantation; and 4) G4 Nd:YAG lased, in which specimens were maintained dry for 3 h followed by Nd:YAG laser irradiation prior implantation.
Laser irradiation
The root surfaces were irradiated using a Nd:YAG laser (Pulse Master 1000 IQ; American Dental Technologies, California) with a wavelength of 1.064 μm. Power outputs were measured through a power meter device. Laser light was delivered through a 0.32 mm optical fiber placed 0.5 cm from the dental root surfaces. Laser parameters at the display were set at 2.0 W power output in a gated-pulsed mode (20 Hz, pulse width of 50 msec resulting in a mean power of 2 W, energy of 100 mJ, and energy density of 124.34 J/cm2). The samples were irradiated for 10 sec with scanning movements. The irradiation was done manually with the optical fiber parallel to the root surface.
In vivo assay (tissue response)
For the in vivo study 12 male Wistar rats weighting an average of 180–200 g were used. The rats were anesthetized prior to surgery using a mixture of xylazin and ketamine (0.15 mL per 100 g of rat bodyweight). Each rat received four implants of treated dental roots, one from each experimental group. The roots were implanted into each quarter of the rat back subcutaneous tissue 15 mm from each skin incision. After the implantation of the roots, the skin incisions were sutured.
Histological preparation
The rats were sacrificed by anesthetic overdose 1, 7, and 45 d later. The skin containing the dental roots and the surrounding tissues were cut and immersed into 10% buffered formalin for 24 h. The specimens were decalcified in a solution of 60% formic acid in formalin for 1 wk. After being washed in water, the specimens were dehydrated and embedded in paraffin. Tissue specimens were sectioned at 6 μm and stained with hematoxylin-eosin (HE) for routine histological examination.
Evaluation criteria
The qualitative histological analysis of semi-serial histological sections was carried out considering the presence or absence and the extension of tissue necrosis and/or inflammation as well as connective tissue maturation.
Scanning electron microscopy preparation
One specimen from each experimental group was prepared for surface topography visualization in scanning electron micrographs. These samples were fixed in 2.5% glutaraldehyde in a 0.1 M phosphate buffer solution (pH = 7.4) for 2 h at 4°C. The post-fixation was done in 1% osmium tetroxide in the same buffer solution. Samples were then dehydrated in ethanol and submitted to chemical drying in hexamethyl disilazane (Electron Microscopy Sciences, Fort Washington, PA). Specimens were then sputter-coated with gold (Sputtering, SCD 020, Bal-Tec, Liechtenstein). Scanning electron microscopy analysis was carried out using a scanning electron microscope (SEM-EDS, Philips-XL 30, Phillips, Einhoven, The Netherlands).
Results
Histological analysis
Figure 1 illustrates the histological features of the rat subcutaneous tissue responses to the dental root implants. The overall aspects of the histological sections, independent of the experimental groups, were the presence of connective tissue capsules of variable thicknesses involving and in intimate contact with the dental roots surfaces, some with cement, others with dentin.

Representative photomicrographs of the histological pictures of the rat subcutaneous tissue around the implanted dental root surfaces. (
Differences were observed in the degree of the inflammatory process and the connective tissue maturation. An intense inflammatory process with presence of edema is represented in Fig. 1A. Moderate inflammatory infiltrate in a tissue exhibiting edema and a high amount of cells are presented in Fig. 1B. Features of thin inflammation-free capsules with acellular tissue (Fig. 1C) exhibiting thick, loose connective tissue rich in fibroblasts (Fig. 1D, 1E) were also observed. High collagen deposition in a mature connective tissue capsule was also observed, especially in the specimens of G4, whose implanted root surfaces had been irradiated with Nd:YAG laser (Fig. 1F).
The dental roots, which were maintained dry for 3 h with no further treatment prior the implantation (G1), appeared to be contained in a fine capsule of loose connective tissue 1 d after implantation. This tissue was mostly composed by a high amount of fibroblasts and exhibited a moderate mononuclear inflammatory infiltrate closely related to the root cement. Seven days later this capsule became thicker with areas of dense connective tissue. The inflammatory infiltrate was more intense with mononuclear inflammatory cells dominating the connective tissue capsule around the dental root (Fig. 1B). At the final experimental time point, 45 d, the inflammatory infiltrate was absent. The connective tissue capsule, once free of inflammatory infiltrate, was thinner. This tissue appeared mostly composed of collagen fibers with a low amount of fibroblasts (Fig. 1C).
The histological sections of specimens from G2, which received implants of dental roots treated with 2.4% sodium fluoride solution, presented with a thin connective tissue capsule involving the dental roots 1 d after implantation. This capsule was infiltrated by polymorphous nuclear inflammatory cells concentrated in some areas (Fig. 1A) intermingled with areas free of inflammatory infiltrate. Seven days later, this inflammatory infiltrate had changed and was dominated by mononuclear cells and the capsule had become thicker. Areas free of inflammatory cells were still observed. In those areas the connective tissue presented some degree of hyalinization. At 45 d after implantation, the involving capsule was free of inflammatory cells. This loosely connective tissue presented a high amount of fibroblasts and a low content of collagen fibers (Fig. 1D).
G3, represented by the subcutaneous tissue around the dental roots that remained hydrated in physiologic saline after tooth avulsion and implanted 72 h later, showed a moderate mixed inflammatory infiltrate. Mononuclear as well as polymorphous nuclear cells were present in this infiltrate 1 d after implantation. Areas of the connective tissue capsule were thin and free of inflammatory cells. These areas covered the dental root surface exhibiting a thin cement layer. Seven days later the capsule was mostly thick with moderate inflammatory infiltrate in connective tissue containing many cells. At 45 d after implantation this histological picture did not change, except for the presence of few areas in the capsule, in some specimens, where the connective tissue showed signs of hyalinization (Fig. 1E).
The connective tissue capsule around G4 specimens, which had dental root surfaces treated by Nd:YAG laser irradiation, showed discrete inflammatory mononuclear infiltrate 1 d after implantation. This infiltrate, 7 d later, was restricted to focal areas of the capsule that became thicker. At the end of the experimental time (45 d) this capsule became thinner and was composed of a mature connective tissue. This tissue was free of inflammatory cells and exhibited large areas of hyalinization. This dense connective tissue penetrated the grooves of the dental root surfaces in intimate contact with the dental root (Fig. 1F).
Scanning electron microscopy analysis
Scanning electron micrographs of root surfaces from all experimental groups are presented in Fig. 2. The overall aspects of the root surfaces were similar, except for the irradiated roots (Figs. 2D, 3). The roots presented mostly smooth surfaces with the cement covering the dentinal tubules. The root surfaces of G1 specimens, which were maintained dry for 3 h prior to fixation, exhibited several cracks and a velvet aspect (Fig. 2B). There were no morphological differences between the root surfaces of G2 (Fig. 3B) and G3 (Fig. 3C) specimens, which were hydrated with fluoride solution followed by physiological serum or by physiologic saline solution alone for 3 h prior to fixation, respectively. These root surfaces were mostly smooth and no open tubules were observed.
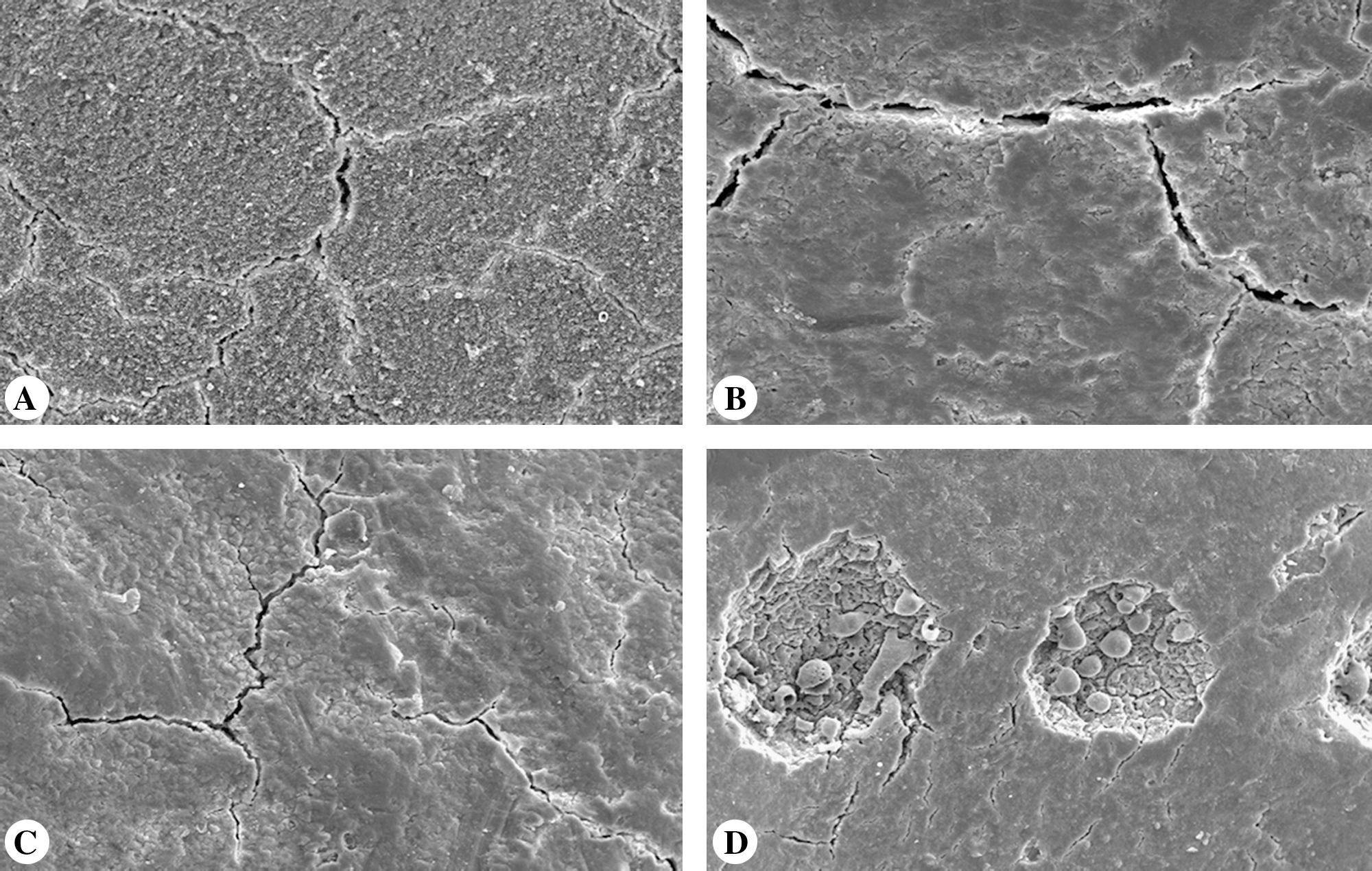
Representative scanning electron micrographs of dental root surfaces of (
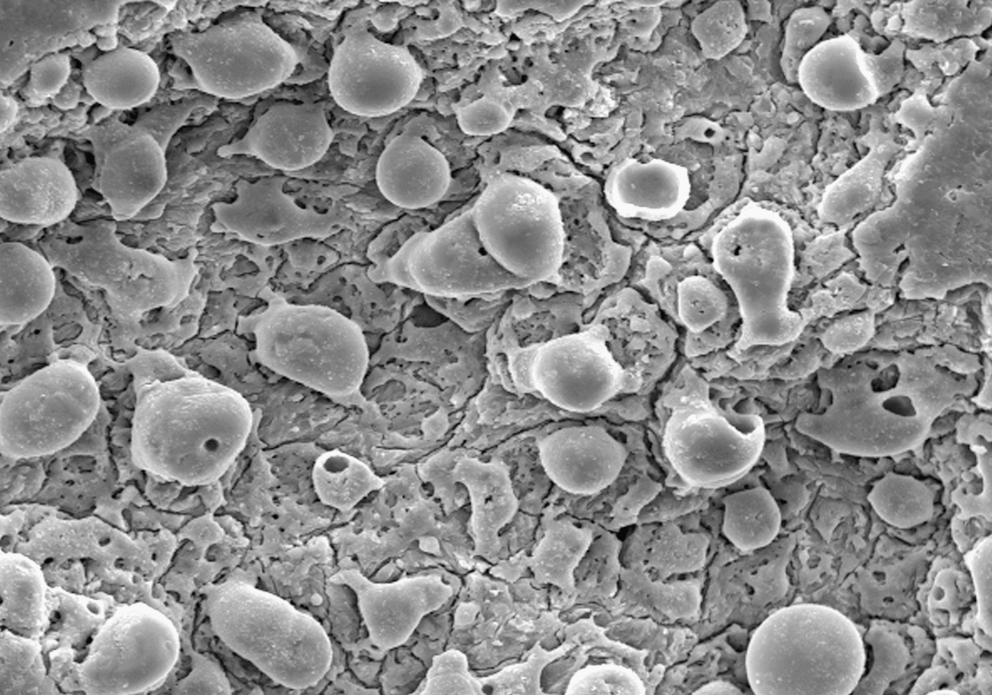
Representative scanning electron micrograph of Nd:YAG-irradiated dental root surfaces (G4; original magnification × 1000).
The root surfaces of specimens maintained dry for 3 h followed by Nd:YAG laser irradiation (G4) showed cement exhibiting smooth areas intermingled with rough areas (Figs. 2D, 3). The rough areas appeared inside circular spots. In detail it was possible to observe a surface with the typical morphology of melted dentine with both globular and glassy appearance (Fig. 3). These areas presented melted mineral globules having a cracked appearance and dentinal tubules sealed by fusion of dentine/cement (Fig. 3).
Discussion
The external dental root resorption that follows tooth replantation can be modulated either by intracanal substances for controlling osteoclastic activity or by creating a sterile and impermeable external surface to control the inflammatory response. The treatment of dental root surfaces before replantation of avulsed teeth must create a biocompatible dental hard tissue, cement, or dentin, to elicit a regeneration of the PDL or at least to induce the formation of connective tissue free of inflammatory cells.
We tested the rat subcutaneous response to implantation of freshly extracted dental roots that were not sterilized and whose surfaces were submitted to one of four different treatment conditions, mimicking the clinical situation. A connective tissue capsule was observed around the dental roots independent of the treatment prior to replantation; however, the progression of the healing process was fastest around the specimens that had been irradiated with Nd:YAG laser.
It is known that the success of the tooth replantation lies in the time between avulsion and replantation 14 –16 as well as the tooth storage conditions during that time. 16 –18 The most frequent period that the tooth stays out of the alveolus with no capital damage to the PDL is between 1 and 4 h. 14,15 More than that, especially if the tooth was stored dry, the PDL can not recover. 18 For this reason the dental roots were left dry for 3 h prior to any treatment and replantation. In one group (G3) the dental roots were left for more time (72 h) prior to replantation, but were kept hydrated.
Some of therapy modalities for controlling the replanted dental root resorption are based on the use of calcium hydroxide, 5 antibiotics paired with corticosteroids, 6 calcitonin, 7 and alendronate, 4 among others. Besides these drugs that can be applied intracanal, the dental roots can also be soaked in 2.4% sodium fluoride solution, 19 tetracycline, 20 stannous fluoride, 20 milk, 21,22 calcitonin, 7 Hank's balanced salt solution, 21 and bisphosphanates. 4 However, physiologic saline and 2.4% sodium fluoride solution are the most universal tooth treatments prior to replantation. 17,19 In this study, the course of reparation of the rat subcutaneous tissue around the implants of dental root was followed at the light microscopy level. Dental roots left dry with no further treatment (G1) or followed by immersion into 2.4% sodium fluoride solution (G2) showed the most intense inflammatory infiltrate during the 45 d period. The sodium fluoride worsened this response, being the only treatment of dental root surfaces that elicited intense and prolonged acute inflammation with the presence of polymorphous nuclear inflammatory cells. Nevertheless at the end of the experimental time inflammation ceased and the cicatrization occurred; however, the sodium fluoride–treated specimens did not reach connective tissue maturation.
When the teeth remained hydrated and were implanted 72 h after extraction (G3) the response of the rat subcutaneous tissue was unfavorable. This approach mimicked the clinical situation in which the teeth were hydrated but remained out of the alveolus for several days. In these G3 specimens the inflammatory infiltrate was perpetuated until the end of the experimental time. This result is in accordance with several authors who have shown that an extended time between avulsion and replantation, even if teeth are hydrated, leads to an unfavorable response with perpetuation of inflammatory response and further root resorption resulting in loss of the teeth. 1 –3,17
The most favorable response was observed in the G4 specimens, which were kept dry for 3 h after extraction and then exposed to Nd:YAG laser irradiation before the dental roots were implanted into the rat subcutaneous tissue. The reparation process occurred in a sequential manner with discrete chronic inflammation followed by cicatrization and complete maturation of the connective tissue within 45 d. This was expected because laser radiation changes not only the dental hard tissue 23 but is also bactericidal. 10
Some features of this study were interesting, such as the different responses in different areas of the same specimen. Areas of explicit inflammation intermingled with areas completely free of inflammatory cells were observed in some specimens of G2 and G4. This indicates that the root treatments on the root surfaces were not homogeneous, which in turn exerted heterogeneous responses. In fact, scanning electron micrographs of Nd:YAG-lased dental roots showed spots created by the pulses of the laser. These irradiated areas probably corresponded to the grooves observed in the light microscopy of G4 specimens that were penetrated by a dense connective tissue in intimate contact with the dental root in 45 d. In these irradiated spots the dental hard tissue melting associated with the sterilization of such tissue could explain the more organized inflammatory process that occurred in these areas.
In conclusion this study has shown that the treatment of dental roots with Nd:YAG laser irradiation improves the biocompatibility of such dental roots, which in turn could be of importance as a tooth treatment before replantation. However, additional studies are needed in order to observe if, along with biocompatibility, this treatment also diminishes tooth resorption after replantation.
Footnotes
Disclosure Statement
No competing financial interests exist.