
Abstract
Introduction
PDT, developed as a therapeutic method for selectively killing targeted cells, 5 involves the systemic administration of a photosensitizer that accumulates in the targeted cells. Subsequently, the cells are irradiated with a laser beam at the appropriate absorption wavelength, and this induces a photochemical reaction. 5,6 Porphyrins were the initial photosensitizers considered to be useful as they have a selective affinity for tumors. 4,5 PDT with systemic administration of porphyrins combined with laser irradiation has been used to treat various malignancies, including lung cancer, gastric cancer, and cancer of the uterine cervix. 5,6 Although porphyrin derivatives, such as hematoporphyrin derivative (HpD) and photofrin II, are used most often for clinical treatment, it is difficult to determine their localizations and mechanisms of action because they are complex mixtures that can have variable compositions. 4,5 Recently, the anti-tumor effects of pheophorbide a (Phde a), a derivative of chlorophyll, in combination with semiconductor laser irradiation, were reported. 7 Because Phde a is hydrophobic, its water-soluble sodium salt, sodium-pheophorbide a (Na-Phde a) was synthesized, and rapid incorporation of Na-Phde a into cells has been demonstrated using fluorescence microscopy. 8
In addition to its antitumor effects, PDT has also been reported to have antibacterial properties. 9 –20 Since the bactericidal activity of PDT is different from the antibacterial activity of antibiotics, PDT has been studied for treating drug-resistant bacteria. 11,12,14,16 PDT has two major advantages over conventional antimicrobials. First, since neither of the two components, the laser or the sensitizer, are inherently bactericidal, the antibacterial effects are limited to the laser-irradiated regions of the sensitizer-treated area. This avoids the disruption of normal microflora at sites other than those targeted. 4,9 Second, the development of resistance to photochemically induced death is unlikely. 18,20 Nevertheless, there are potential problems with PDT, one of which is a lack of bacterial specificity. 4
Recently, we have demonstrated that the combined use of semiconductor laser irradiation and Na-Phde a as a sensitizer exhibited antibacterial efficacy against methicillin-resistant Staphylococcus aureus (MRSA) in vitro. 21 Combination treatment with Na-Phde a and laser irradiation completely eradicated MRSA at a density of 108 cfu/ml. 21 Furthermore, we also reported that PDT using Na-Phde a prevented bacterial growth and joint destruction caused by MRSA septic arthritis in a mouse model. 3 These findings suggest that PDT with Na-Phde a has excellent potential for treating MRSA septic arthritis. 3,21 Therefore, the investigation of the most suitable light source is required for the clinical use of antibacterial PDT.
The objective of this study was to compare the effects of various light sources on the sterilizing power of PDT using Na-Phde a.
Materials and Methods
Target bacteria strains
The bacteria used in this experiment were a standard Staphylococcus aureus strain obtained from the American Type Culture Collection (ATCC25923: provided by the department of clinical microbiology, Surugadai Nihon University hospital).
They were subcultured and incubated at 37°C for 24 hours in blood agar medium.
Catalase and a morphologic Gram test were used to confirm species identification.
The strains were diluted to an optimal density using No.1 McFarland standard solution (1.0 × 108 CFU/ml) and distributed into glass tubes.
Photosensitizer
Na-Phde a (Chlorophyll Research Institute, Yamanashi, Japan) was used as a photosensitizer. The absorption wavelength of Na-Phde a is 667 nm. 3,8 Na-Phde a was dissolved in phosphate buffered saline (PBS) to achieve a concentration of 280 μmol/L, as this concentration completely eradicates MRSA in vitro. 21
Light sources
To establish the best conditions for PDT, the sterilizing power of various light sources for PDT treatment were compared. The following light sources were used for this study: GaA1P semiconductor laser (power: 300 mW, wavelength: 670 nm, Jntec co., Ltd, Tokyo, Japan). Total fluence was approximately 7.2 J/cm2. Halogen lamp (power: 75 W, Tokyo metal co., Ltd., Tokyo, Japan). Total fluence was approximately 15.8 J/cm2. Xenon lamp (power: 300 W, Smith and Nephew Japan co., Ltd., Tokyo, Japan). Total fluence was approximately 68.6 J/cm2. Fluorescent lamp (power: 27 W, National co., Ltd., Tokyo, Japan). Total fluence was approximately 19.6 J/cm2.
Irradiation with each of these light sources was performed for 30 minutes at a distance of 30 cm from the bacterial dishes. This distance was selected as the minimum distance at which the semiconductor laser could irradiate the entire Petri dish. Total fluence of the laser device was calculated as laser power (W) × time (seconds)/area of Petri dish (diameter 10 cm). The fluence of incoherent lamps (lm · S) was calculated using an illuminometer (illuminance meter; T-10, Minolta co., Ltd. Tokyo, Japan) and converted to J/cm2 as previously reported. 22
PDT
One ml of 280 μmol/L Na-Phde a solution and 1 ml of bacterial inoculum were mixed in a capillary tube and incubated for 60 minutes in a dark room. After incubation, the solution was transferred to several Petri dishes and then irradiated by each light source for 30 min, as described above.
Evaluation of the bactericidal effect of PDT
The reaction liquid dilutions were made by using 0.1 ml of the reaction liquid and 0.9 ml of NaCl solution (10 times dilution), and this was repeated up to 106 of dilution. Twenty μL of the reaction liquid was positioned at the division of the blood agar. After this, irradiation was performed by each light source, and the dish was incubated in microaerophilic conditions for 24 hours at 37°C. The control groups were diluted and incubated using the same method as the PDT groups. The solution used was made of a mixture of 1 ml of bacterial inoculum and 1 ml of PBS.
The dilution series were made in two separate plates (for safety) and after 24 hours' incubation, the plate with colony development was selected for evaluation.
The results of bacterial cultures were graded as follows: +++: bacterial growth that exhibited confluence. ++: bacterial growth that showed partial confluence but the number of colonies could not be counted. +: bacterial colonies were isolated and countable. −: no bacterial growth
Results
The GaA1P semiconductor laser and halogen lamp group showed complete bactericidal effects at all dilution levels. In the xenon lamp group, only the original concentration plate showed bacterial growth, and this was at the level of isolated bacterial colonies. In the fluorescent lamp group, a bactericidal effect was observed under the dilution of 104. The control group showed bacterial growth at all dilution levels (Fig. 1). Evaluation of bacterial growth is shown in Table 1.
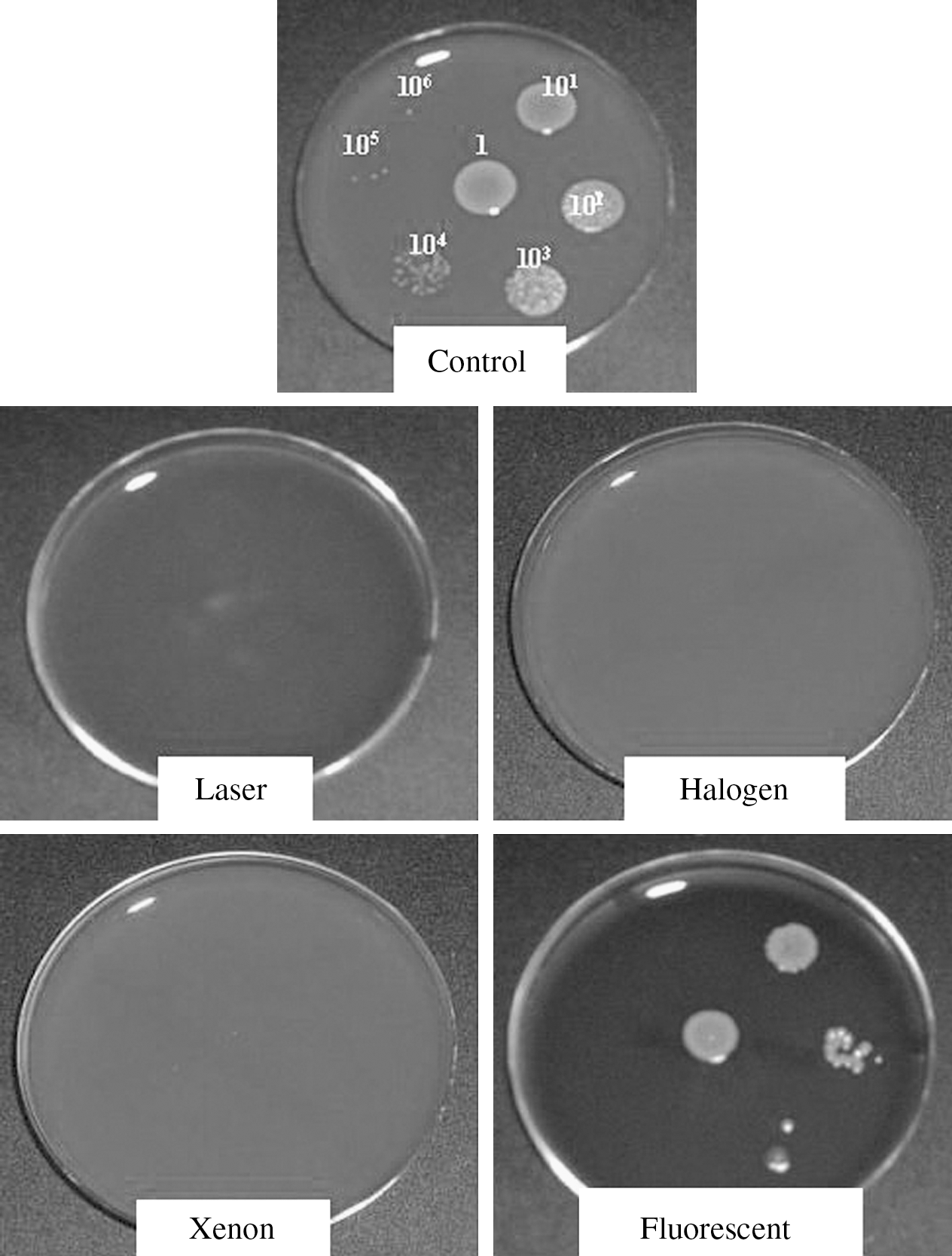
Sterilizing power of different light sources for PDT using Na-Phde a. Diluted series of bacterial solution were divided in each area as described in the materials and methods. Semiconductor laser and halogen lamp groups showed perfect bactericidal effects after PDT. Xenon lamp and fluorescent lamp groups showed partial bactericidal effects.
Bactericidal effects of PDT with different light sources. Results are graded as described in the materials and methods.
Discussion
In this study, PDT using Na-Phde a showed a strong bactericidal effect against MRSA with the combination of semiconductor laser or halogen lamp irradiation. Xenon and fluorescent lamp irradiation exerted weaker bactericidal effects, showing partial sterilizing power.
In the field of orthopedic surgery, PDT has been widely applied for treating joints affected by rheumatoid arthritis. 23 –30 However, the effectiveness of PDT against septic arthritis or soft tissue infections has not been well studied. We have focused on the antimicrobial effect of PDT using Na-Phde a. Na-Phde a is a photosensitizer that is made from chlorophyll. As chlorophyll is a natural compound, it can be metabolized easily in the human body without any side effects. 8 The most important attribute of Na-Phde a as a photosensitizer is its long absorption wavelength (670 nm), that allows deep body layer penetration even with low power laser irradiation. 8 Furthermore, as Na-Phde a has a much longer absorbance wavelength (around 670 nm) when compared with hematoporphyrin derivative (HpD), Na-Phde a has a stronger effect in causing cell death. 8 Taira et al. 3 demonstrated that the intra-articular injection of Na-Phde a as a sensitizer and percutaneous irradiation with a semiconductor laser inhibited MRSA growth and joint destruction in an MRSA arthritis mouse model. 3 Since one of the obstacles of using PDT clinically is the long-term skin photosensitization that occurs after systemic administration of photosensitizers, intra-articular injection of the photosensitizer minimizes the occurrence of this complication. 3,23,24 Recently, Iriuchishima et al. reported that the use of PDT with Na-Phde a for joint tissue in normal mice is a safe procedure and does not cause any irreversible changes in the joint tissue. 31
Light source selection is one of the most important factors in PDT. 4,5,6,10 As each photosensitizer has its own appropriate absorption wavelength, the laser is widely used in the clinical setting. 6 We have reported the effectiveness of the combined use of semiconductor laser and Na-Phde a to eradicate MRSA or to treat MRSA septic arthritis in a mouse model. 3,31 In this study, we revealed that not only the semiconductor laser but also the halogen lamp is useful for PDT using Na-Phde a. The xenon and fluorescent lamps also showed a partial sterilizing power against MRSA. Several studies have evaluated the influence of the light source in PDT. Babilas et al. found no difference between the halogen lamp and the LED in PDT for the treatment of actinic keratosis. 32 Wiegell et al. reported that daylight is also useful for actinic keratosis treatment, as is LED for PDT. 33 Juzeniene et al. evaluated the difference between LED and halogen lamp light sources for PDT, and showed that even with the use of the halogen lamp, human tumor cell death was observed. 34 For deep infectious focus, such as septic arthritis, a coherent light source, such as semiconductor laser or LED, should be used for PDT. However, to irradiate widespread infections, the laser device is not suitable and its cost is high when compared to the incoherent lamps. Therefore, for large superficial infections such as wound infection and pressure ulcers, incoherent lamps are adequate for sterilization. We believe that the strong local sterilizing effect of Na-Phde a makes the use of PDT with incoherent lamps possible.
One limitation of this study is that the influence of hyperthermia was not evaluated. Further studies are required to determine the appropriate energy, irradiation time and distance of the light source for clinical use of PDT. In particular, in vivo studies are needed to investigate PDT using Na-Phde a for clinical application as an antibacterial therapy. However, PDT using Na-Phde a appears to be a functional treatment for septic arthritis or other soft tissue infections.
Footnotes
Acknowledgments
We wish to thank Sheila J.M. Ingham, M.D., for her kind grammatical revision. Authors also wish to thank Masataka Nakazato and Chlorophyll Research Institute for their kind donation of Na- Phde a. This study was supported in part by Grant-in-Aid for Scientific Research (c) from Japan Society for the Promotion of Science, and grants from the Ministry of Education, Culture, Sports, Science, and Technology for the promotion of the industry-university collaboration at Nihon University.
Author Disclosure Statement
No competing financial interests exist.