
Abstract
Introduction
The term low-level laser therapy (LLLT) is broadly applied to the therapeutic effects of lasers. The clinical application of LLLT is expanding rapidly and several review articles on the topic have been published. 12 There are reports indicating that LLLT can improve fracture healing and bone regeneration in vivo and in vitro. 13 –23 Trelles and Mayayo 13 demonstrated that LLLT significantly increased vascularization and modulated the formation of osseous tissue in the fractured tibiae of mice. 13 Barushka et al. 14 found that laser photo stimulation on drill-hole injuries in the tibia of rat affected the population of osteoblasts and osteoclasts, altered alkaline phosphatase activity, and promoted bone repair. 14 The positive effects of low-level laser on healing fracture were documented by measuring the biomechanical integrity of healing bones. 15,16 Recently, Silva Junior et al. 17 and Liu et al. 18 illustrated that laser irradiation improved fracture repair of bones in animal models with latent promotion of bone remodeling at the area of injury without changes in bone architecture and increased callus volume and bone mineral density, and Garvello-Freitas et al. 19 demonstrated that laser irradiation significantly improved bone matrix organization in surgically produced damage to rat tibia. Very recently, other investigators demonstrated that LLLT accelerated bone formation and bone repair in rat calvarial bone defect and in the mandibular region. 20 –22
Until now, there has been no knowledge pertaining to a study of LLLT on diabetic bone tissue. However, whether LLLT can be useful as a treatment modality in diabetic hard tissue, and how it may be beneficial and effective is yet to be determined. It is necessary to investigate the effects of low- and high-energy densities (doses) of He-Ne laser on diabetic bone tissue by biomechanical and histological evaluating methods because the mechanisms of action of LLLT of diabetic bone are not known. The purpose of this study was to investigate the hypothesis that biostimulation with LLLT increases biomechanical and histological parameters in streptozotocin-induced diabetic (STZ-D) rats.
Materials and Methods
Animals and study design
Twenty adult male Wistar rats, 4 months old and weighing 273.2 ± 28.3 g, were used in this study. Rats were randomly divided into groups 1, 2, 3, and 4. They were provided food and water ad libitum and were weighed biweekly throughout study. Diabetes was induced in rats of groups 1 and 2. The right tibia of rats in group 1 was treated by He-Ne laser with 28.6 J/cm2 energy density daily for 14 consecutive days. In groups 2 and 3, the right tibia was treated with LLLT the same as group 1 but with 636.9 J/cm2 energy density. The left tibia of rats in groups 1–3 was used as relevant control bone of right laser-treated bone. In five healthy rats of group 4, the right tibia was used for baseline studies. All procedures were approved by institutional medical ethics committee.
Induction of diabetes
Diabetes was induced in 10 rats of groups 1 and 2 by an intraperitoneal injection of pancreatic β cell toxin STZ (Zanosar Pharmacia & Upjohn Co., Kalamazoo, MI) freshly dissolved in sterile distilled water at a single dose of 60 mg/kg body weight. 24 Rats of groups 3 and 4 received a control injection of distilled water. Diabetes was defined as blood glucose concentration greater than 300 mg/dL in orbital sinus blood sample (Gm 300; Biomine GmbH, Heerburg, Switzerland) 7 d after STZ injection. Blood glucose levels were monitored once a week throughout the study. All diabetic rats were maintained for 30 d after STZ injection.
LLLT
LLLT was begun in the right tibia of rats in groups 1 and 2, 31 d after STZ injection. LLLT was performed daily for 14 consecutive days. To administer LLLT, we divided the whole length of the tibia into three equal squares (1 cm × 1 cm) and placed the tip of the laser source near (<1 cm) the surface of the skin at the center of each square, directing it perpendicularly to the target tissue for the designated time, i.e., 90 sec in group 1 (28.6 J/cm2 energy density) and 1200 sec in groups 2 and 3 (382.2 J/cm2 energy density). A gaseous He-Ne laser unit (Model IR 2000; Iranian Atomic Energy Agency, Tehran, Iran) with a continuous wavelength of 632.8 nm, 10 mW output, circular beam shape, and 0.0314 cm2 spot size was used in this study.
Biomechanical examination
After 14 d from the beginning of LLLT, rats of study groups were sacrificed by inhalation of chloroform in a closed space. Tibiae were collected, wrapped in gauze that had been soaked in physiologically balanced saline, and then were frozen at −20°C for later biomechanical tests. Before biomechanical testing, the specimens were slowly thawed at room temperature and kept moist during all handling and testing procedures. Biomechanical properties of five bones in each group were determined. Bones were subjected to the three-point bending test 25 on a materials testing device (Zwick Z 2.5 H 15 WN, Ulm, Germany) until failure occurred. All bones were similarly oriented in the testing machine. A supporter with two loading points 19 mm apart was used to mount each bone, and a press head was then activated to compress the middle of the bone shaft until fracture occurred. Compressive loading speed was 0.08 mm/sec in all tests. Data were automatically recorded to the material testing device from the load–deformation curve and the following values were calculated: maximum force (N), load at the break (N mm), bending stiffness (N/mm), and energy absorption (N mm). Briefly, these biomechanical indices may be defined as follows: maximum force is the force needed to break the bone; load at break is the force needed to separate breaking segments; bending stiffness is the slope on the linear portion of load–deformation curve, i.e., the ratio of load to deformation in the elastic region of the curve; and energy absorption is the amount of energy that is absorbed by bone until breaking occurred.
Histological examination
The fractured tibiae were fixed in formalin saline and decalcified in an EDTA solution for 6 wk. Embedded in paraffin, transverse sections of diaphysis were cut and stained with hematoxylin and eosin. Histological analysis was carried out on sections from five animals per group. The results were evaluated semiquantitatively by an experienced pathologist in a blinded fashion, on a graded scale. The scoring was based on the density of bone lamella meshwork (BLM) in compact bone as: (0) absent, there was no BLM in the field; (1) mild, <25% of BLM in the field; (2) moderate, 25–50% of BLM in the field; (3) severe >50 % of BLM in the field. 20,26
Statistical analysis
The results are expressed as mean ± SD. Normal distributions of data were examined by one-sample Kolmogorov–Smirnov test. Paired Student t tests were used for comparison of body weight and biomechanical and histological data of control and laser-treated bones (subgroups) of each group. Independent sample t test was used for to compare data between different study groups. A p value of ≤ 0.05 was considered statistically significant.
Results
Out of 10 rats of groups 1 and 2, 8 rats developed clinical evidence of diabetes following STZ injection so another 2 rats were added to the study. Diabetic rats showed a significant decrease in body weight by the end of study (273.2 ± 28.3 vs. 216.7 ± 47.54) (paired Student t test, p = 0.000). Blood glucose levels rose to 421.8 ± 92.6 mg/dL in diabetic rats.
Biomechanical examination
Biomechanical examinations revealed that LLLT with 382.2 J/cm2 energy density significantly increased maximum force of normal bone and diabetic bone in comparison with controls (paired Student t test p = 0.05, p = 0.007; Fig. 1). These examinations also showed that LLLT with 28.6 J/cm2 energy density significantly increased load at the break of diabetic bone in comparison with its control (paired Student t test p = 0.000; Fig. 2). Additionally, LLLT with 28.6 J/cm2 energy density significantly decreased bending stiffness of diabetic bone in comparison with its control (paired Student t test, p = 0.025; Fig. 3).

Mean ± SD of maximum force (N) of study groups. Maximum force of laser-treated bone in group 3 and in group 2 was significantly higher than the relevant control bones (paired Student t test, p = 0.05 and p = 0.007, respectively). Group 4 was normal bone.
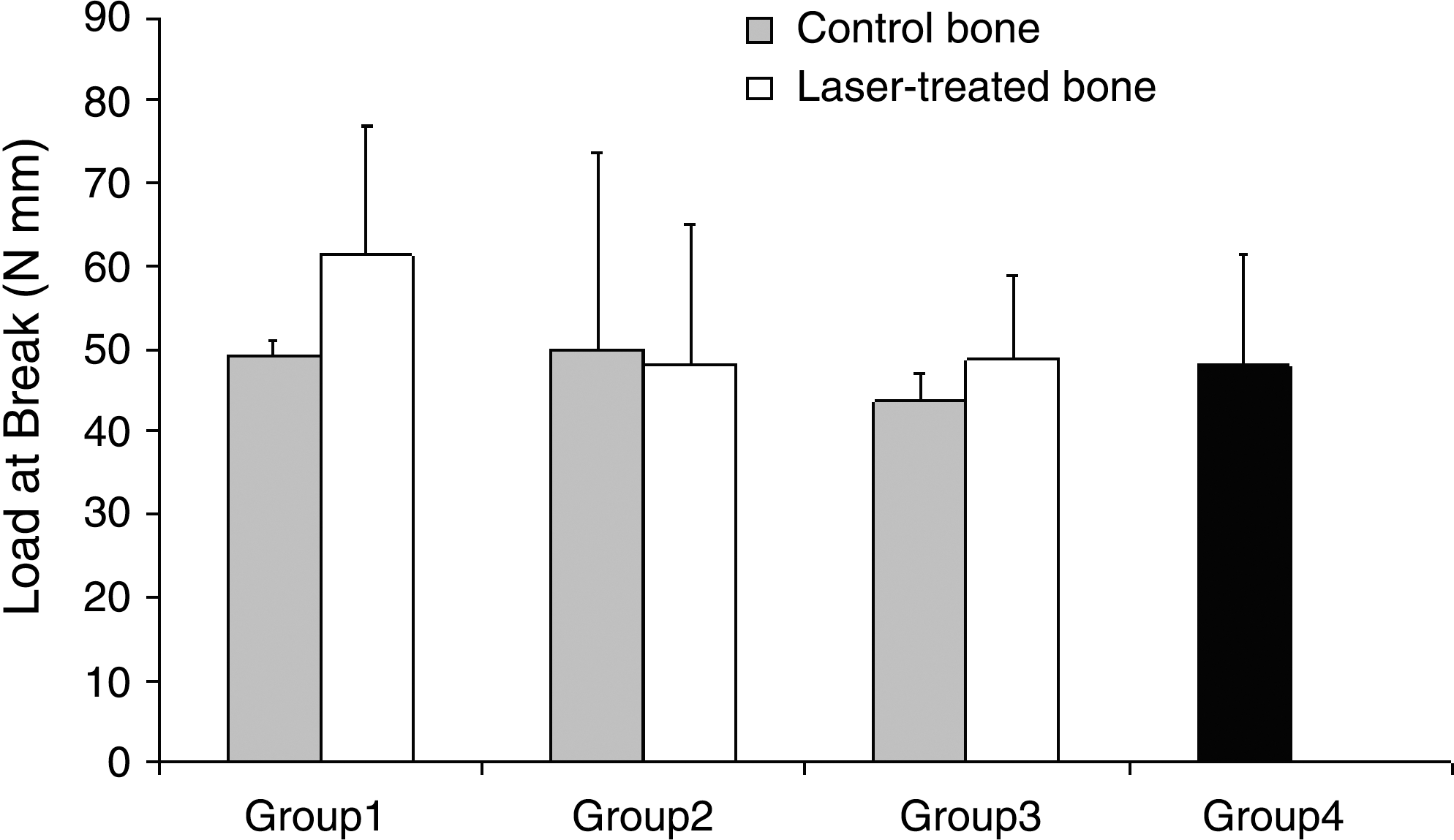
Mean ± SD of load at break (N mm) of study groups. Load at break of laser-treated bone in group 1 was significantly higher than its control bone (paired Student t test, p = 0.000). Group 4 was normal bone.
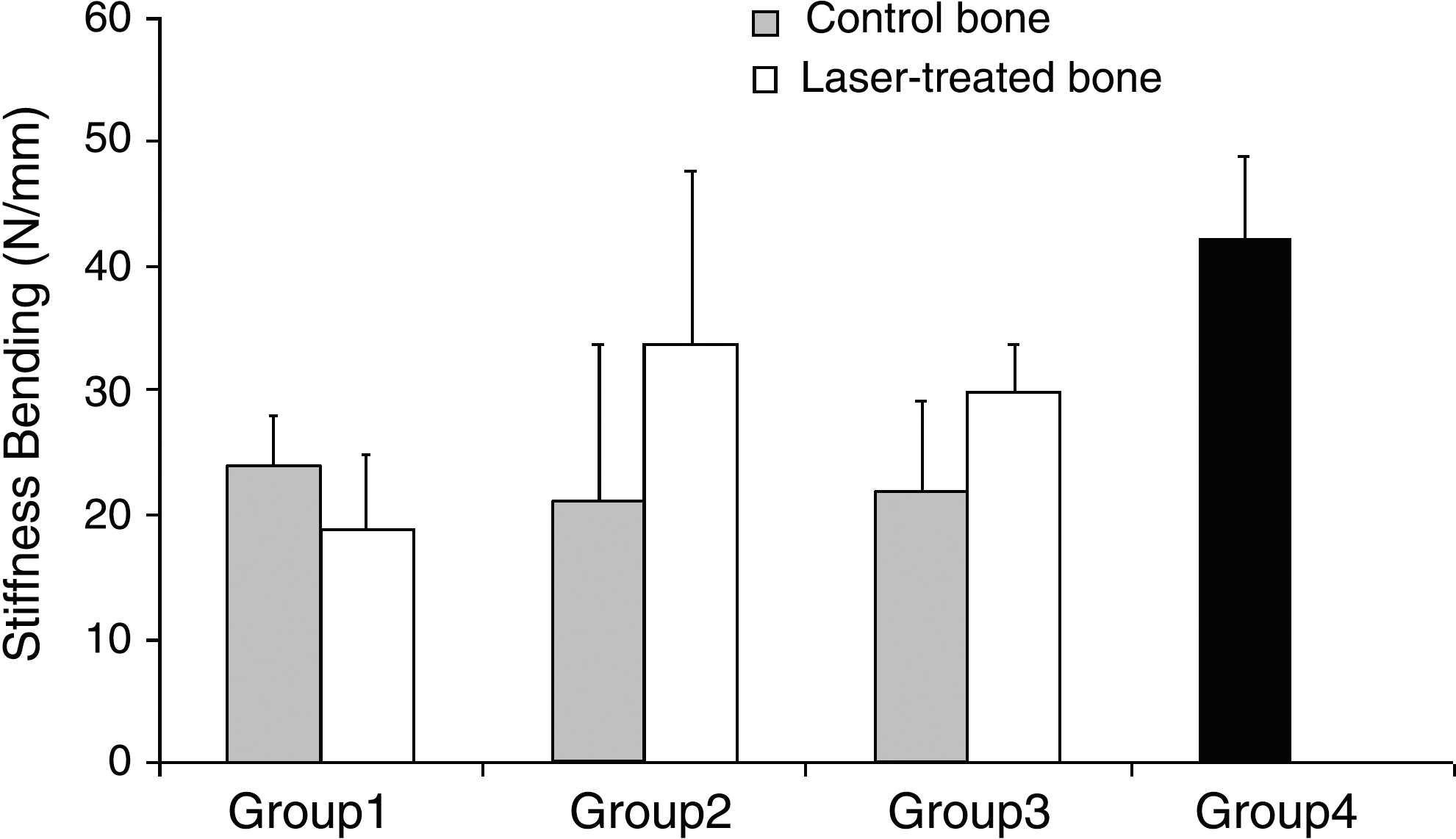
Mean ± SD of bending stiffness (N/mm) of study groups. Stiffness bending of laser-treated bone in group 1 was significantly lower than its control bone (paired Student t test, p = 0.025). There was also bending stiffness of control bone in group 1, laser-treated bone and also control bone in group 1 and laser-treated bone in group 2 were significantly lower than group 4 (normal) (paired Student t test, p = 0.002, p = 0.001, p = 0.011, respectively). Group 4 was normal bone.
Detailed biomechanical examinations also revealed that diabetes significantly decreased bending stiffness of control bone of group 1, laser-treated bone, and control bone of group 2 in comparison with the normal group (independent sample Student t test, p = 0.002, p = 0.001, p = 0.011, respectively). Further, diabetes significantly decreased the maximum force of laser-treated bone in group 1 compared with the normal group (independent sample Student t test, p = 0.05; Fig. 1).
There were no significant differences between study groups with regard to energy absorption (Fig. 4).
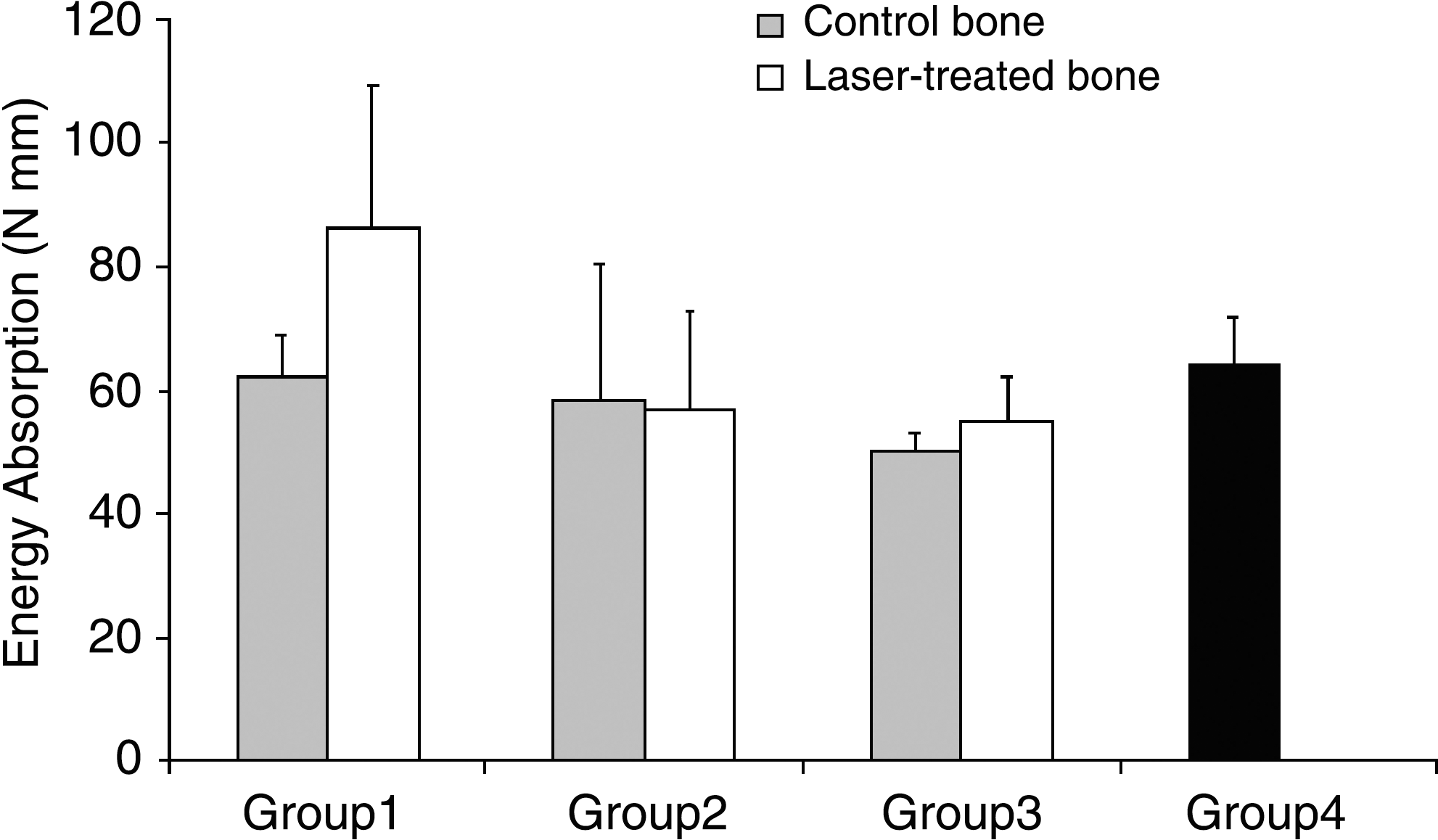
Mean ± SD of energy absorption (N mm) of study groups. There were no significant differences between study groups. Group 4 was normal bone.
Histological examination
Histological examination indicated that LLLT with 382.2 J/cm2 energy density significantly increased the diabetic bone lamella density of compact bone in comparison with its relevant control group (paired Student t test, p = 0.005; Fig. 5). Also, LLLT with 382.2 J/cm2 energy density considerably increased the diabetic bone lamella density meshwork in comparison with laser-treated bones and control bones of groups 3 and 4 (independent sample t test, p = 0.016, p = 0.016, and p = 0.034, respectively) (Fig. 5).
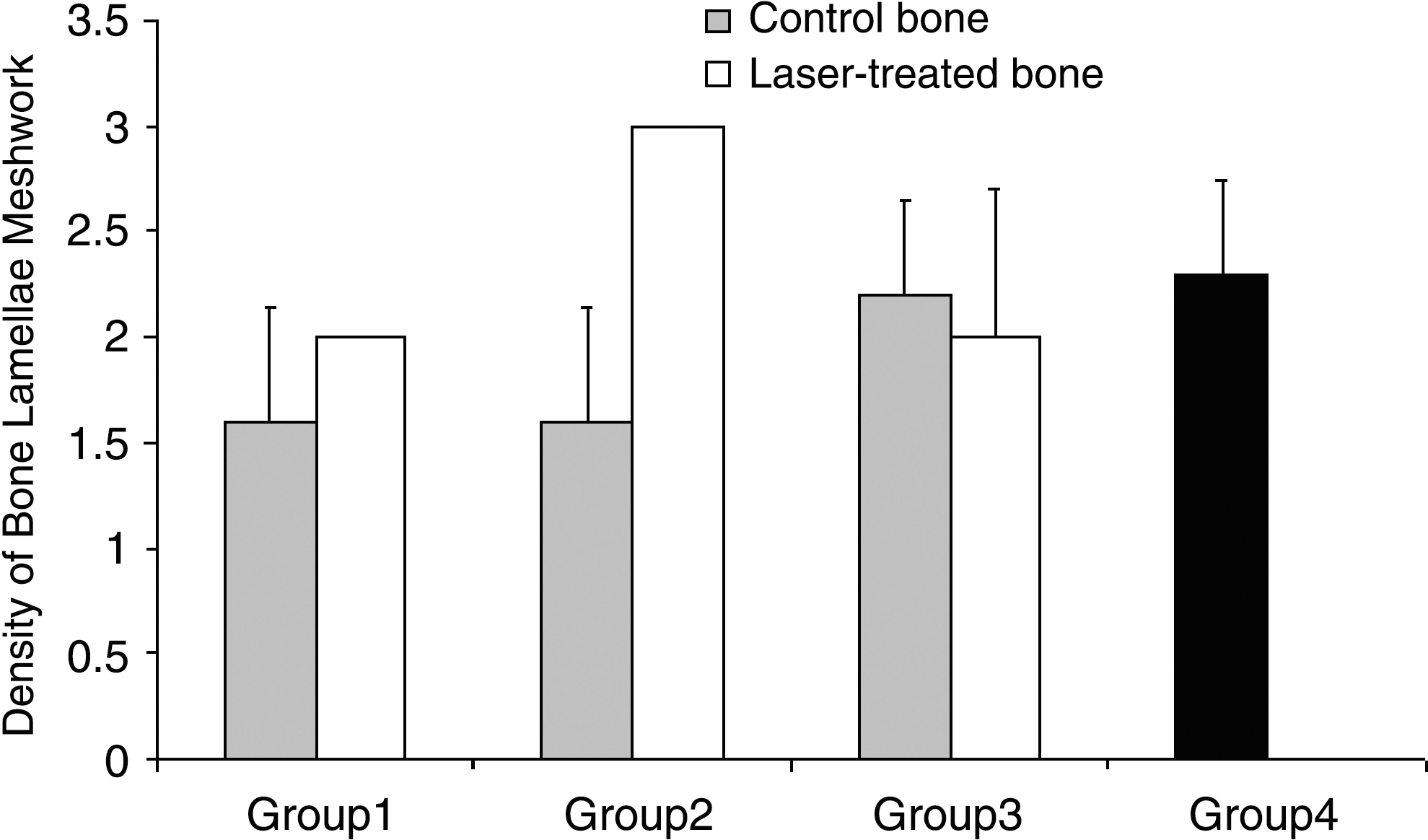
Mean ± SD of bone lamella meshwork density of study groups. Bone lamella meshwork density of laser-treated bone in group 2 was significantly higher than its control bone (paired Student t test, p = 0.005). Bone lamella meshwork density of laser-treated bone in group 2 was significantly higher than that of control bone and also laser-treated bone in group 3 and also group 4 (independent sample Student t test, p = 0.016, p = 0.016, and p = 0.034, respectively). Group 4 was normal bone.
Discussion
The choice of the type of low-level laser used
The radiation produced by He-Ne laser at 632.8 nm wavelength has mostly been studied among various low-intensity lasers for promoting wound healing. Several studies have shown that He-Ne lasers at 632.8 nm wavelength are effective in accelerating fracture healing in animal models. 13 –17 It is notable that evidence suggests that the absorption of light emitted by a He-Ne laser begins with the components of the respiratory chain, whereas radiation emitted by the Ga-As (diode) laser begins at the membrane level, that is to say, during the cascade of molecular events that lead to a better photochemical response of the tissue in comparison to other lasers. In addition, the differences in coherent properties of lasers may be attributed to He-Ne effects on diabetic tissue. It is known that the radiation emitted by the He- Ne laser has more coherence in its nature than that of radiation emitted by Ga-As laser, 14,27,28 which led to our choosing the He- Ne laser for the present study.
Luger et al. 15 and Rochkind et al. 21 investigated the effect of He-Ne laser irradiation on bone fracture healing in animal models. Luger et al. 15 made a bone defect in right tibia of rats and Rochkind et al. 21 made a defect in the mandible. The bone defects were treated by He-Ne laser transcutaneously to the area of fracture daily for 14 consecutive days. They observed that the results from laser-treated groups were significantly better than those of control groups. Luger et al. 15 and Rochkind et al. 21 concluded that He-Ne laser treatment plays a role in enhancing bone healing, so in the present study we treated bones by He-Ne laser for 14 consecutive days too. It is notable that doses in previous studies performed on healthy animals varied from 20 to 178 J/cm2. The doses used in the present study were higher than these, because previous studies have shown that diabetes impairs bone metabolism. 1 –5
The choice of energy density
Results of histological and biomechanical examinations in the present study showed that LLLT with a 382.2 J/cm2 energy density had a biostimulatory effect on bone in STZ-D rats. It caused an increase in the density of the BLM of compact bone and in the maximum force. Although LLLT is expected to have a biostimulatory effect on diabetic bone, the results of the present study demonstrated that LLLT with a proper energy density had an ideal effect on diabetic bone. At first the bones of diabetic rats (group 1) were treated with He-Ne laser radiation with 28.6 J/cm2 energy density, and biomechanical and histological examinations failed to show a biostimulatory effect in comparison with relevant control bones. These results agree with findings reported by Gordjestani et al. 29 who showed no differences in bone metabolic activity between laser-treated bone defects (20 J/cm2 infrared laser) and control bone defects. We performed further examinations. Other diabetic bone (group 2) was treated with 382.2 J/cm2 energy density, and we found maximal force was significantly higher in laser-treated bones compared to control bones. LLLT dose used in group 2 was chosen due to the results of group 1 possibly being due to skin reducing the energy level of the He-Ne laser beam. 30 The increased energy level in group 2 was needed to induce biostimulation of bones of diabetic rats as shown by biomechanical and histological examinations. Our results are in line with those of studies on fracture healing in healthy rats by David et al., 31 Luger et al., 15 and Garvello-Freitas et al. 19 David et al. 31 studied the effect of 0, 2, and 4 J/cm2 He-Ne laser irradiation of tibial fracture in rats. Radiological and histological examinations of fracture area failed to show any biostimulatory effect of He-Ne laser; our group 1 results coincided with these findings. However, these results contradict those of our group 2 and of Luger et al., 15 who showed that maximal load at failure and structural stiffness was elevated significantly in the He-Ne laser–treated rats at a dose of 140 J/cm2. It is notable that Luger et al. 15 broke the tibia according to the method used by David et al. 37 Luger et al. 15 reported that based on their experience they are of the opinion that David et al. 34 used laser irradiation doses that were too low (since the skin reduces the energy level of laser beam to 3–6% of its original intensity 30 ) and that explains the lack of effect. Garvello-Freitas et al. 19 reported a significant increase in the area of neoformed in the tibiae irradiated with 0.3 J and 0.9 J compared to control, but there was no significant difference between laser treatment with 0.03 J and the control. 19 So it is concluded that the response of diabetic bone to LLLT is dose dependent.
The choice of laser-treated and control groups
Comparison of a laser-treated bone to a control bone, both from the same animal as performed in present study, has been described by different authors 15,32 –34 who have reported a biostimulatory effect of LLLT on irradiated bone defect compared to nonirradiated ones. However they did not report a systemic effect of LLLT. 15,32 –34 It seems there were not any systemic effect in our study either.
The effect of diabetes on bone
We could not find any significant difference between the biomechanical parameters of bones in diabetic and nondiabetic rats, but there may be significant differences between them as Reddy et al. 8 reported. However, Reddy et al. 8 did not exactly clarify the duration between STZ injection and sampling in rats. and they performed biomechanical tests 7 wk after establishment of diabetes in rats. 8 In our study we performed biomechanical examination 6 wk after injection of STZ.
According to the previous reports the mechanisms behind diabetic effects on bone are as follows: 1) decreased osteoblast recruitment and function 35 ; 2) decreased osteoblast activity 7 ; 3) decreased bone formation 36 ; and 4) altered soluble form of alkaline phosphates. 37
The effect of low-level laser on diabetic bone
In the present study we show LLLT with 382.2 J/cm2 energy density significantly increased the maximum force of normal bone when compared to the control group. Other studies have shown biostimulatory effects of LLLT on osteoblasts and bone, including: 1) a tendency for enlargement of the Golgi apparatus 38 ; 2) stimulation of cellular proliferation, ALP activity, and osteoblast cin gene expression 39 ; 3) much higher osteopontin as compared to nonirradiated osteoblasts 23 ; 4) prevention of bone loss 40 5) stimulation cell proliferation in human osteoblast-like cells 41 ; and 6) biostimulation of bone tissue. 42
In the present study some or all of the above-mentioned issues may be responsible for the observed biostimulatory effects of LLLT on diabetic bone.
In our study, in which histological findings support the biomechanical results, one explanation for these results may be LLLT increases both osteoblasts' proliferation and activity. Furthermore, bone formation and LBM density of diaphyseal compact bone in diabetic rats are increased, so strength of bone was significantly increased compared to its control group. However, further studies are needed to evaluate our speculation.
Osteoblasts have been found to be responsive to LLLT in vitro 23,27 and in vivo. 13 –22,32 –34 LLLT may enhance the response of osteoblasts to insulin, which increases their activity and leads to increased bone formation. It has been shown in other studies that LLLT significantly accelerates the wound healing process in experimental diabetic models. 34,43,44
It seems that LLLT enhances cell proliferation and activity in hyperglycemic and diabetic conditions. 44 Since elevated glucose has been shown to impair mineralization in vitro, 45 the positive effect of LLLT on cells in hyperglycemic conditions may be responsible for improved BLM density and biomechanical integrity, which were observed in the present study.
Conclusion
We conclude that LLLT with a He-Ne laser given in a dose-dependent manner in an experimental diabetic model increased BLM density of compact bone on diaphysis of long bone; it also increased its maximal force as compared to nonirradiated bones. The results show the positive effects of LLLT on diabetic bone for the first time. Clearly further studies need to be carried out to investigate the biostimulatory process affecting cells of bone in diabetic animal models in vivo and in vitro.
Footnotes
Acknowledgment
This paper is supported by Vice-Chancellor of research of Shahid Beheshti University, M.C. (grant No. 10012). We wish to thank the late Mrs. Jamileh Rezaie. We also wish to thank the Vice-Chancellor of research of Shahid Beheshti University, M.C. for financial support (grant No. 10012), Miss Sahar Bayat for assistance in feeding rats, Mrs. Mina Koohi for typing the paper, and Miss Nasrin Khateri for drawing figures.
Disclosure Statement
No competing financial interests exist.