
Abstract
Introduction
The disadvantages of lasers include eradication of the specimen for histologic examination, slower healing rate, and high cost of equipment. The most common advantages are less bleeding, improved sterility, decreased scarring and swelling, reduced postoperative pain, greater precision and improved cutting control. 5 –9
The CO2 laser, which has a wavelength of 10.6 μm, has become a favorite instrument in the treatment of soft tissue pathologies because of its affinity for water-based tissues. 9 –11 It destroys tissue with minimal surrounding tissue damage. Its hemostatic nature make the CO2 laser ideally suited for excision and vaporization of mucosal tissue in the oral cavity. 10,12
In oral surgery, the clinical application of CO2 laser has been recommended to treat benign oral lesions such as fibromas, papillomas, hemangiomas, gingival hyperplasias from various causes, aphthous ulcers, ankyloglossias, and premalignant lesions like lichen planus and oral leuokoplakia. 13,14 The CO2 laser does not possess any enhanced ability to cure oral disease when compared with conventional procedures such as the scalpel, electrosurgery or cryotherapy. Rather, it is a precise means of excising soft tissue lesions with little upset to the patient. 15
Recent studies present conflicting results on the efficacy of CO2 lasers when compared with other surgical instruments. Some clinical reports have indicated that the early phase of wound healing after laser surgery is faster than that after scalpel surgery and is associated with less postoperative pain, less blood loss, and shorter operative time. 10,16 In contrast, later investigations have suggested that the CO2 laser produces more secondary tissue injury with slower healing rates than the scalpel. 10 Lateral thermal damage from the CO2 laser is primarily due to thermal diffusion, the conduction of heat energy to the tissue surrounding the incision site during laser irradiation. 17 The conflicting data from early reports concerning the efficacy of the CO2 laser may have resulted, in part, from differences in instruments, variations in instrument settings, and differences in tissue and animal models.
The aim of the present study was to evaluate the effect of collateral thermal damage on histopathological diagnosis, and to compare CO2 laser and conventional surgery applied on oral soft tissue pathologies in terms of anesthesia need, postoperative pain, and intraoperative and postoperative complications.
Materials and Methods
A total of 43 patients, referred to our clinic for the treatment of soft tissue pathologies, participated in the study. Thirty-two female and 11 male patients with a mean age of 54 ± 7.0 (range 15–80) requiring soft tissue surgeries were randomly assigned to receive treatment either with conventional surgery with scalpel (control group; n = 19 patients; 14 female, 5 male, with a mean age of 52.85 ± 18.09,) or with the CO2 laser technique (study group; n = 24 patients, 18 female and 6 male with a mean age of 55.95 ± 15.54 (range 16 to 75). The exclusion criteria consisted of (a) diseases or drugs that would affect the wound healing, such as diabetes, (b) suspicious malign tumors, and (c) corticosteroid therapy. The study protocol was reviewed and approved by the ethical committee (No: 17. 10. 2006). Consent was obtained from all patients. The patients' past medical and dental history, thorough extraoral and intraoral examination, and, if needed, radiographic imaging were recorded. Also recorded were systemic medications, anesthesia method and need, postoperative pain, systemic pain medications, if needed, and intra- and postoperative complications.
For the surgeries in the laser group, a 10.6μm CO2 laser, which is invisible to the eye, was used (MedArt®610, MedArt A/S, Hvidovre, Denmark). The system has flexible, hollow wave guides and straight and angled handpieces which apply laser to the oral soft tissues in a non-contact treatment mode. Laser power was adjusted to 3–4 W, continuous wave (CW), depending on the size of the lesion under local anesthesia. The tissue was irradiated in defocused mode for several seconds without water spray. The radiant power density varies throughout the cross sectional area of the laser beam, with an increased density in the center of the beam. It is important to move the handpiece continuously in small circular movements to achieve the best possible heat distribution.
The patients, surgeon, and other staff in the separate operating room wore safety glasses during the surgery and the room entry was clearly marked with a warning sign. Mouths were protected from reflection of the laser by wet gauzes. In the control group, conventional surgery procedures were applied.
Conventional surgery procedures were performed under local anesthesia (Ultracain D-S 4%, Aventis Pharma, Istanbul, Turkey) whereas the surgeries with CO2 laser were performed under topical anesthesia (Xylocain spray 10%, Astra Zeneca, Sweden), if needed, additional local anesthesia (Ultracain D-S 4%, Aventis Pharma) was applied. Excised tissues, except soft tissues taken from frenulum and vestibuloplasty operations, were sent to Yeditepe University, Department of Pathology, for histopathologic evaluation. Assessment of the effect of thermal damage was determined according to the presence of the artifact.
All wounds formed by laser were left open to secondary epithelization. In the control group, wounds were also sutured for primary epithelization.
Both groups received postoperative instructions and they were told to use the same analgesic containing paracetamol (acetaminophen) (Minoset, Roche, Basel, Switzerland), if needed. To avoid infection of the open wounds, patients were told to rinse their mouth twice a days with chlorhexidine gluconate 0.1% (Klorhex, Drogsan, Istanbul, Turkey). Amoxicillin (Largopen, Bilim, Istanbul, Turkey), 500 mg, 3 times daily, was prescribed to patients treated with scalpel.
For statistical analyses, the Statistical Package for Social Sciences (SPSS) software (SPSS for Windows, version 10, Chicago, IL, USA) was used for data processing and analysis. The Pearson x2-test or the Fisher exact test were used as appropriate to assess the statistical significance, and p-values of less than 0.05 were considered statistically significant.
Results
CO2 laser or conventional surgery was used for the treatment of 43 cases aged between 15 and 80 years, indicated primarily for fibroma (16), epulis fissuratum (EF) (11), peripheral giant cell granuloma (PGCG) (6), labial frenulum (LF) (4), pyogenic granuloma (PG) (3), and hemangioma (3). The age distribution of treated cases is shown in Table 1.
EF, epulis fissuratum; PG, pyogenic granuloma; PGCG, peripheral giant cell granuloma; LF, labial frenulum; C, control group; S, study group.
The distribution of study and control group patients in terms of anesthesia need and analgesic usage are shown in Table 2. Postoperative pain was assessed according to analgesic usage. Although 18 (90%) patients in the control group used analgesics postoperatively, only seven (29%) patients in the laser group used them (x2 = 16.45, p < 0.001). When both groups were compared in terms of anesthesia need, it was significantly lower in the laser group (x2 = 17.11, p < 0.001).
The operation time with the CO2 laser was short, as there was no bleeding during or after the operations and no need to use sutures. There were no intra- or postoperative complications during either the CO2 laser surgery or the surgical scalpel surgery of the lesions (Fig. 1a, b, c and Fig. 2a, b, c). No secondary infection was observed in any of the cases. The coagulated tissue changed into a layer of scab tissue over the irradiated surface within one day, and a new epithelium gradually grew from the surrounding tissue, closing inward until the wound surface was fully healed. The patients who underwent laser surgery were healed within three weeks whereas the patients who underwent scalpel surgery were healed within two weeks.


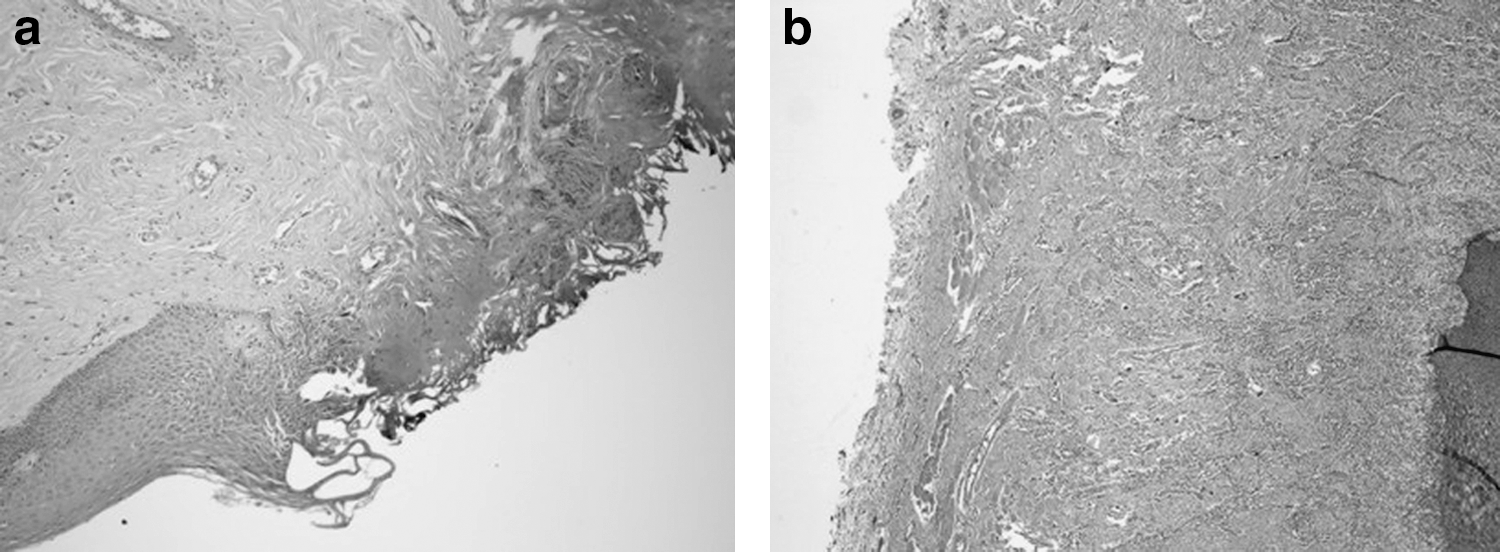
According to histopathological evaluation of 39 specimens, diagnoses of fibroma (16), epulis fissuratum (11), pyogenic granuloma (3), hemangioma (3), and peripheral giant cell granuloma (6) were established. Thermal damage caused by the CO2 laser surgery on the borders of the specimen did not effect the pathologist's diagnosis (Fig. 3a, b).
Discussion
Although the scalpel and electrosurgery are the methods of choice for making surgical incisions, the CO2 laser is becoming a widely accepted alternative in oral surgery. Introduced more than 20 years ago, the CO2 laser was used on only a limited basis because of the unwieldy nature of its rigid delivery system. With the advance of the flexible hollow wave guide, surgeons can now easily access nearly all regions in the oral cavity. 18 Through the development of smaller portable devices, minor routine procedures can be performed in the office under local anesthesia. 1,18
Injection of local anesthetics is the most uncomfortable part of the entire dental treatment. Topical anesthetics are usually applied before local anesthetic injections to prevent dental anxiety and fear. Local anesthetics are used to control intraoperative pain and reduce bleeding. Research has shown that the CO2 laser has a coagulation effect on small vessels that provides hemostasis and seals the sensory nerve endings, providing reduced anesthesia need. 5,6 Bornstein et al. reported that almost one third of studied cases did not need additional local anesthetics after topical anesthesia. 12 In this study, topical anesthesia was also sufficient for intraoperative pain control for more than half of the patients in the laser group. Need for anesthesia is related to the pain reaction threshold of the patients and the dimensions of the lesion. Topical anesthetics control pain efficiently during procedures involving small and superficial lesions. However, large and, especially, deep lesions require local anesthetics.
Postoperative pain has been reported to be reduced in CO2 laser surgery procedures. 9,12 Our study results showed that patients treated with CO2 laser used significantly less analgesic, which is assumed to be related to minimal postoperative pain and functional complications, compared to scalpel surgery. This may be due to the protein coagulum that forms on the wound surface in CO2 laser surgery, thereby acting as a biological dressing and sealing the ends of the sensory nerves. Decreased postoperative pain in these patients may also be due to an altered inflammatory response in laser wounds.
Wound healing and the thermal effects of CO2 laser used on soft tissues have been reported to cause artifacts to form on the border of the biopsy specimen. This thermal injury has been reported to be minimal and wound healing to be appropriate in the long term, with no effect on diagnosis. 12,15,19 The thermal damage can be controlled and reduced by alternating the use of power settings, pulse duration, and pulse repetition rate. 20 –22
In our study, all 39 soft tissue biopsy specimens sent for histopathologic analyses could be evaluated and there were no misdiagnoses caused by the collateral thermal damage on the incision line. Our results are compatible with those of other researchers. 12
Authors comparing laser and scalpel mucosal wounds have found diminished collagen formation, decreased capillary proliferation, and delayed epithelization in laser wounds. It is believed that the thin layer of denatured collagen associated with laser wounds acts as an impermeable dressing that initially reduces the degree of tissue irritation; this delays inflammatory infiltrate migration and fibroblast formation. 9
Wounds created by CO2 laser healed more slowly than those created by scalpel surgery in this study. This may be due to delayed epithelial migration and decreased scar formation (possibly due to changes in collagen conformation at the wound surface).
Scalpel excisions may heal more rapidly and produce the least amount of tissue injury and inflammation with the fastest healing, as evidenced by earliest epithelization and collagen formation. The scalpel, however, produced significantly more bleeding than the laser. This may obscure the surgical field in a region where it may be difficult to get adequate exposure.
The CO2 laser produced adequate hemostasis but it was time consuming because of the numerous passes required to produce a complete incision. It also produced a significant amount of tissue damage. It is likely, however, that more precise removal of small amounts of tissue can be achieved with this instrument compared with the scalpel. CO2 laser is superior to scalpel incision surgery from the standpoint of hemostasis of small blood vessels in the operative field, maintenance of a sterile field (due to the high temperature of the laser beam), and reduction of acute inflammatory reactions and postoperative pain, which increases the comfort of the patient. Although the CO2 laser can be recommended for vascular lesions such as hemangioma, there may be some difficulty in its use. MacCaffrey and Cortese noted that the CO2 laser was more effective at cutting than coagulation, and because the straight-line open-tube delivery of the CO2 laser beam may not permit good visualization of the lesion, bleeding from the vascular lesion may be difficult to control. 23 Potassium titanyl phosphate (KTP) laser is also suitable for treating vascular lesions, but it can also have disadvantages, as there is the danger of transmural injury if the duration of the laser application is excessive. 24
The choice of the instrument must be tailored to the needs of the surgeon and the demands of the particular procedure. Although the results of this study are limited in value due to the small patient sample, they do show that CO2 laser can be effectively used as an alternative modality of treatment for soft tissue pathologies with promised convenient operation and acceptable results.
Footnotes
Acknowledgments
The authors are grateful to Assoc. Prof. Dr. Nurhan Guler for her kind support and valuable contribution in the preparation of this manuscript.
Author Disclosure Statement
No competing financial interests exist.