
Abstract
Introduction
Regarding the Er:YAG laser settings advised for cavity preparation, pulse energy and pulse repetition rate are the most important parameters, being directly related to the laser's ability to ablate dental substrates. 5 –7 Several studies 8 –10 using permanent teeth have attempted to settle and standardize basic workable parameters to yield optimal and safe ablation of dental hard tissues, but a consensus has not been reached.
Considering the differences between dentin of permanent and primary teeth such as hardness and mineral content; 11 that the peritubular dentin of primary teeth is approximately 2 to 5 times as thick as that of permanent teeth, and hence the dentin tubules of primary teeth have a smaller diameter; 12 and that primary teeth have greater tubular numerical density and hence lesser intertubular dentin area available, 13 it can be inferred that the interaction of laser with the dentin of primary teeth presents distinct ability to ablation.
In this context, it is of fundamental importance to establish parameters of energy and frequency of an Er:YAG laser specific for this substrate. The lack of studies evaluating laser ablation capacity in primary teeth and linking with the morphological appearance of the laser ablated teeth hamper the application of this technology with clinical parameters insurance.
The Er:YAG laser capacity of ablation dental substrates has been evaluated using different methodologies, such as volume measure using a three-dimensional sensor,
5
depth of ablation through optical measures using stereomicroscopy and scanning electron microscopy (SEM),
Thus, in view of the increasing approach of laser technology in dental practice and the structural and morphological differences between primary and permanent substrates, studies should be done to avoid extrapolation of results obtained with permanent teeth to primary teeth. 11,13
Therefore, the aim of this study was to assess different energies and pulse repetition rates of Er:YAG laser in primary dentin and, also, the surface morphology of the substrate irradiated.
Materials and Methods
The Ethics Committee of the School of Dentistry of Ribeirão Preto, University of São Paulo approved this study. Forty-eight sound primary molars exfoliated or extracted within a 6-month period were selected and stored in 0.4% sodium azide solution at 4°C.The teeth were cleaned with a scaler and a water-pumice slurry in dental prophylactic cups and examined under a 20X magnifier to discard those with structural defects and maintained for a week in distilled water at 37°C before entering the experiment.
Assessment of dentin mass loss
When present, roots were sectioned 2 mm below the cementoenamel junction using a water-cooled diamond saw (Minitom, Struers A/S, Copenhagen, Denmark). Next, crowns were fixed with wax in plexiglas plates and bisected longitudinally in the mesiodistal direction using a double-faced diamond disk (KG Sorensen, 7015, Barueri, SP, Brasil) mounted on a low-speed handpiece into 84 fragments with standard dimensions of 5mm x 5mm. The fragments were identified and individually stored in plastic containers with distilled water at 4°C.
Afterward, each specimen was individually fixed with wax in a cylindrical Teflon abutment and ground in a water-cooled polishing machine (Politriz DP-9U2, Struers, A/S, Copenhagen, Denmark) with #320- to #600- grit silicon carbide (SiC) paper (Buehler Ltd., Lake Bluff, IL) to remove the overlying enamel and expose a flat dentin surface area of at least 3 mm. The specimens were removed from the cylindrical abutment, cleaned, and re-immersed in distilled water at 4°C for 24 h, with the purpose of re-humidifying the substrate.
After this period, the fragments were kept at room temperature for 2 and then removed from water, dried with absorbing paper for 20 s, and individually weighed in a precision analytical balance (Mettler, H54, Switzerland) to six decimal places of accuracy to determine the initial mass in milligrams. Once the initial masses were recorded, the fragments were hydrated for 1 h at room temperature, with the objective of enabling simulated conditions of the oral cavity close to clinical reality.
Then the fragments were individually fixed with wax on plexiglas plates, using a parallelometer to ensure that the dentin surface was kept parallel to the horizontal plane. To demarcate the 3-mm-diameter ablation site, a piece of insulating tape with a central hole, made using a modified Ainsworth rubber-dam punch, was attached to the dentin surface.
The fragments were randomly assigned to four groups, corresponding to the Er:YAG laser energies used for cavity preparation (160, 200, 250, and 300 mJ). Each group was divided into three subgroups (n = 8) according to the pulse repetition rate setting (2, 3, and 4 Hz).
The Er:YAG laser device used was a Kavo Key Laser 2 (Kavo Dental GmbH & Co.KG, Biberach, Germany), emitting a wavelength of 2.94 (m. The laser beam (spot size =0.63 mm) was delivered in non-contact and focused mode with a fine water mist at 1.5 mL/min for 20 s. The energy densities were 51.3, 64.2, 80.2, and 96.23 J/cm2, respectively, for the energies of 160, 200, 250, and 300 mJ. The laser energy density was calculated using photographic paper, according to Meister et al. 12
Specimens were irradiated only once, using the #2051 handpiece attached to a flexible fiber delivery system. The irradiation distance of 12 mm was standardized using a custom-designed apparatus consisting of two parts: a holder, to fix the handpiece in such a way that the laser beam was delivered perpendicularly to the specimen surface, and a semi-adjustable base, on which the plexiglas plate was firmly fixed with wax. Two previously gauged operators manipulated the apparatus' micrometer screws in such a way that the semiadjustable base was alternately moved in right-to-left and forward-to-back directions, allowing the laser beam to provide accurate ablation of the entire dentin site.
Once the irradiation was performed, the fragments were removed from the plexiglas plates, thoroughly cleaned, and stored in distilled water for 1 h. Afterward, the final mass was recorded by weighing the specimens in the precision analytical balance, following the same protocol described above. Mass loss rate, in milligrams, was calculated by subtracting the final mass from the initial mass. Thus, the ablation capacity of Er:YAG laser (ablation rate) was determined according to the amount of dentin removed.
Mass loss averages and standard deviations were calculated, and data were analyzed using two-way analysis of variacne using a factorial design with energy and pulse repetition rate as independent variables. Multiple comparisons were made using the Tukey statistical test at a 0.05 significance level.
Morphological analysis
After weighing, the laser-ablated specimens were prepared for analysis using SM, according to the following protocol: immersion in 2.5% glutaraldehyde (Merck KGaA, Darmstadt, Germany) in 0.1M sodium cacodylate buffer at pH 7.4 (Merck KGaA) for 12 h at 4°C. After fixation, the samples were rinsed with 0.1M sodium cacodylate buffer solution several times, dehydrated in an ascending ethanol (Labsynth Produtos para Laboratório Ltda., Diadema, SP, Brasil) series (25% for 20 min, 50% for 20 min, 75% for 20 min, 90% for 30 min, 100% for 60 min), immersed in hexamethyldisilazane (Merck KGaA) for 10 min, placed on absorbing paper inside glass plates, and left to dry in an exhaust system.
Specimens were mounted on stubs with their lased surfaces facing up, sputter-coated with gold, and examined using SEM (Philips-FEG SEM, Philips Electron Optics, The Netherlands) belonging to the Laboratory of Structural Characterization, Department of Materials Engineering, Federal University of São Carlos operating at 15 kV. The most representative areas were recorded, and three examiners analyzed the morphological findings in a double-blind manner, by performing a visual and qualitative comparison of the Er:YAG-lased surfaces.
Results
Dentin mass loss
Regarding pulse repetition rate settings, at any given energy examined in this study, Er:YAG laser irradiation of primary dentin with 4 Hz provided the most effective ablation (4.15 mg), which was statistically different from that obtained with 2 Hz (2.19 mg) and 3 Hz (3.19 mg). These results could be summarized as follows: 4Hz > 3Hz > 2Hz.
Considering energy settings, irrespectively of the pulse repetition rate used, the greatest ablation of primary dentin was observed when pulse energy was set at 300 mJ (4.22 mg), different from those obtained with 160 mJ (2.17 mg) and 200 mJ (2.92 mg) and similar to that obtained with 250 mJ (3.38 mg), which were greater than that obtained with 160 mJ (2.17 mg) and similar to energy of 250 mJ (3.38 mg), this latter energy showed an ablation ability similar to that obtained with 160 mJ (2.17 mg). These results could be summarized as follows: 300 mJ > 200 mJ ≈ 160 mJ; 300 mJ ≈ 250 mJ; 250 mJ ≈ 200 mJ.
When the interactions between energy and pulse repetition rate were analyzed, the setting 300 mJ and 4 Hz provided the highest ablation rate, presenting averages different from all other groups (Table 1).
Same letters indicate statistical similarity (p < 0.05).
Surface morphology
The surface morphology of primary dentin irradiated with 160 mJ/2 Hz was characterized according to nonselective tissue removal, exhibiting an irregular topography with opened dentinal tubules. When this energy setting was employed with higher pulse repetition rates (3 and 4 Hz), the topography demonstrated the greater surface irregularities and greater ablation of intertubular dentin, leaving the peritubular dentin with a protruded appearance (Fig. 1A, B).
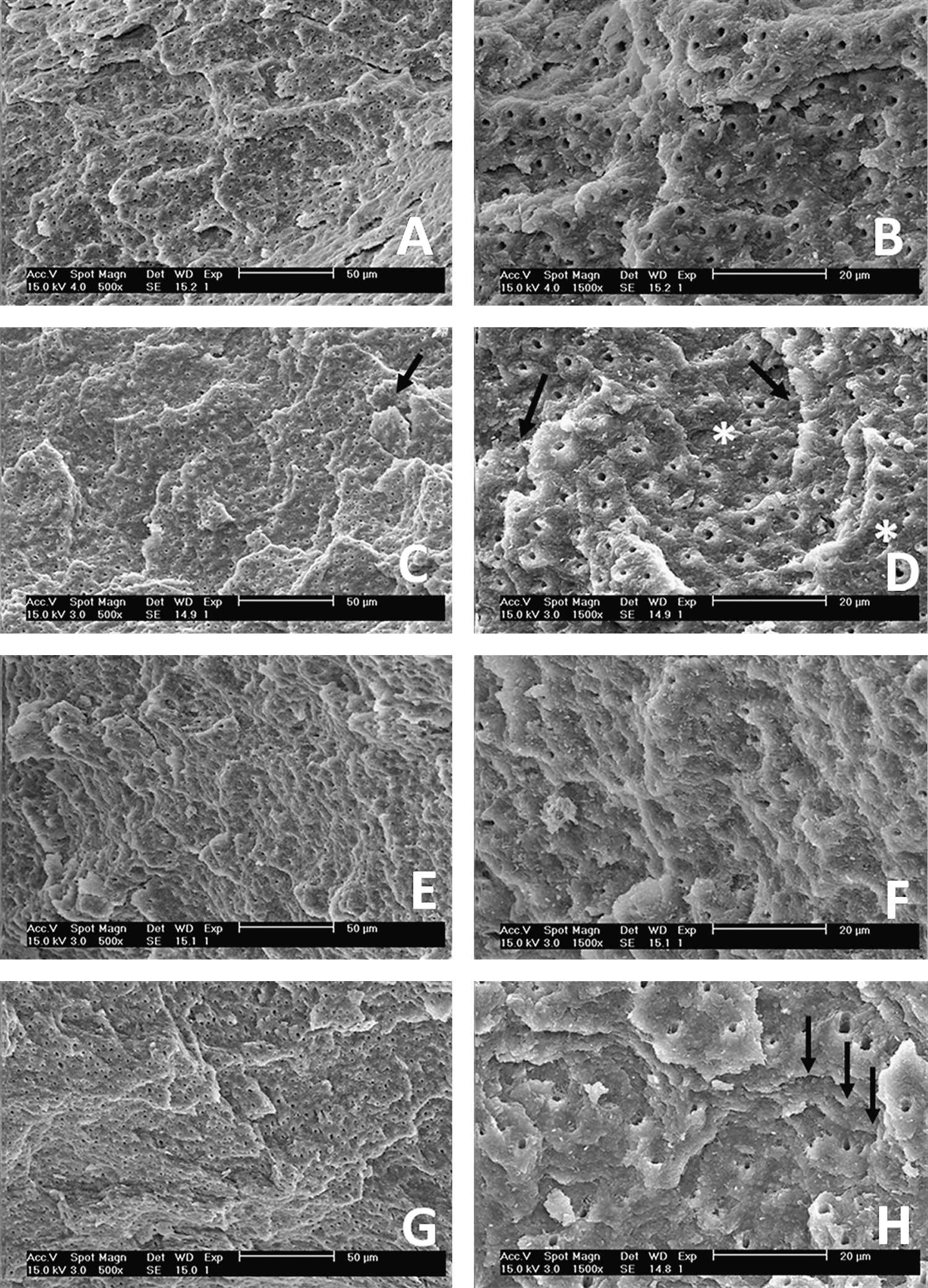
Surface morphology of primary irradiated dentin.
Er:YAG laser irradiation at 200 mJ provided a dentin surface more irregular and open but not widened dentinal tubules or protruding peritubular dentin (Fig. 1C, D). Faster pulse repetition rates yielded a surface topography with obliterated dentinal tubules and small gaps.
Parameter settings of 250 mJ and 2, 3, and 4 Hz resulted in greater surface irregularities, dentinal tubule obliteration, and gaps, producing an amorphous pattern (Fig. 1E, F).
Dentin surface irradiated with 300 mJ had greater dentinal tubule obliteration, larger gaps, and greater ablation of intertubular dentin, leaving the peritubular dentin with a protruded appearance. When the same energy setting was used with 4 Hz, the morphological appearance of the dentin revealed greater depth of ablation, gaps, and cracks, producing an amorphous dentin pattern (Fig. 1G, H).
Discussion
The higher water content and the relatively predominant organic composition of dentin potentiate the action of the Er:YAG laser. This is even more accentuated in primary tooth dentin 17 because of the structural, chemical, and morphological characteristics of this substrate. 11 –13
The findings of this study indicate that the ablation ability of Er:YAG laser in primary dentin is directly proportional to the rise of the pulse repetition rates employed. This outcome may be because the increase in pulse repetition rate inherently leads to an increment of the energy density that achieves the target surface per unit of time during irradiation. As a consequence, more microexplosions occur in the same time interval, and therefore more tooth substance is expected to be removed. 18,19
Using permanent teeth, a significantly greater rate of dentin ablation with the rise of the pulse repetition rates has been observed. 6,8,15 Others 20 have reported that an increase of the repetition rate from 5Hz to 10 Hz did not result in changes in surface morphology.
With regard to energy, at any given pulse repetition rate used, it was observed that a small increment in energy setting did not produce a significant increase in dentin mass loss rate. Some authors 7,21 havee demonstrated that the energy did not influence dental tissue ablation; therefore, a small change in this parameter did not promote a significant change in the ablation rate.
In this context, Li et al. 6 verified that the Er:YAG laser has a threshold ablation rate at which the rise in energy density (J/cm2) does not increase proportionally the depth of the cavity, and after this threshold is passed, the mass loss raises lineally according to the energy. In contrast to our results, Shigetani et al. 19 found a significant difference between energy settings of 50 and 100 mJ and between 150 and 200 mJ when the Er:YAG laser pulse repetition rate was set at 1 Hz.
Concerning the morphological aspect of the primary dentin after Er:YAG laser irradiation, it was observed that higher pulse repetition rates resulted in more-evident alterations in the surface morphology, such as greater ablation of intertubular dentin, obliterated dentinal tubules, gaps, and cracks, producing an amorphous pattern.
A likely explanation for such topographical pattern may be that the pulse repetition rate is described as the most important parameter in heat deposition on lased-irradiated tissue; therefore, the higher the pulse repetition rate, the lower the tissue cooling between every pulse. 21,22 This fact indicates a linear relationship between the ablation depth and the volume of tooth substance removed as a function of the pulse repetition rate employed. 6,23,24
Higher energies produced surface irregularities with greater ablation of intertubular dentin, which resulted in a protruded appearance of peritubular dentin and obliterated dentinal tubules. These results are in agreement with those of previously reported data, 25 –28 which indicate that Er:YAG laser interaction is more intensive on substrates with higher water content. Therefore, because the intertubular dentin has a higher percentage of water and organic constituents, mainly collagen fibers, it is much more ablated than the peritubular dentin. 24,27,29
Although the irradiation has been performed with a water flow of 1.5 mL/min, the occurrence of an amorphous dentin pattern may be attributed to the methodology adopted in this study. In this methodology, the laser beam was applied to an established area until forming a cavity, in a such a way that the irradiation was repeated more than once on a same site, increasing the heat deposition on the substrate.
Nevertheless, the analysis and comparison of the results obtained in this study regarding the ablation capacity of Er:YAG laser on primary dentin and the morphology of the irradiated surface are unsure because of the lack of research on this subject. Moreover, the literature is conflicting concerning the irradiation parameters of the different lasers.
The validity of Er:YAG laser for cavity preparation in primary teeth has been discussed more and been more accepted because of the advantages of this technology over conventional methods. Since 1999, after Food and Drug Administration approval for Er:YAG laser use in children, clinicians use this technology more safely.
However, the working parameters of the Er:YAG laser for preparing primary dentin is not well established. New studies should be performed in an attempt to establish the ideal parameters of the Er:YAG laser for ablating primary enamel and dentin. The current data available for permanent teeth should not be extrapolated to primary teeth so that this new technology may become routine in pediatric clinical practice.
Conclusion
Based on the results obtained in this study, it can be concluded that the ablation ability of Er:YAG laser in primary dentin and surface morphological damage were higher as energy and pulse repetition rate settings increased and that the setting 200 mJ and 2 Hz promoted a good ablation rate with fewer surface alterations in the substrate.
Footnotes
Disclosure Statement
No competing financial interests exist.