
Abstract
Introduction
Since Milligan and Morgan's surgical description of open hemorrhoidectomy, many methods have focused on curing hemorrhoids including rubber band ligature, 3,4 cryosurgery, 3,5 photocoagulation, 1,6 –9 and stapling, 10,11 depending on the severity of the disease, 12 which is not easily defined.
The use of laser in proctology began in the 1960s, when the Nd:YAG laser was first used for anorectal surgery. After that, new lasers such as the CO2 laser and new technologies such as the pulsed and the scanned laser resulted in improved outcomes. 13,14 Laser action on biological tissues is not yet a “closed” issue, however, and the use of laser energy on hemorrhoidal tissue remains controversial despite recent improvements in technology. 15
Plapler et al. 16 studied 350 patients submitted to CO2 laser open hemorrhoidectomy during the course of a year, in terms of pain and local healing. They concluded that laser has advantages compared to “conventional” surgery, specifically less postoperative pain and a more aesthetic scar.
Zahir et al. 17 published a retrospective study in 2000 comparing 50 patients, half of whom had laser therapy and half who had conventional hemorrhoidectomy. They concluded that laser leads to minor postoperative pain even though it is an open surgical techniques like the “traditional” surgery, which requires the extraction of the hemorrhoidal tissue, leaving an exposed surface.
A new technique permits surgeons to treat varicose veins of the inferior limbs with a diode laser applied inside the vein. 18 This endovascular technique allows enlarged veins to be treated without requiring several skin cuts, and it can be performed as an ambulatory surgery.
Plapler et al. 19 studied the effect of the diode laser (810 nm wavelength) on interstitial tissue of the anal region of rats and showed that the diode laser leads to minimum alterations, as long as the laser–tissue interaction rules are obeyed. Additionally, Plapler 20 showed that diode laser can be used to treat hemorrhoidal disease in monkeys.
In a clinical trial, Karahaliloglu 21 described the submucosal application of the diode laser (980 nm) to treat first and second degree hemorrhoids in 105 patients and stated that the method is painless and results in total recovery.
We investigated if endovenous ablation of hemorrhoidal veins using an 810 nm diode laser improves the outcome of operated patients.
Materials and Methods
This project was approved by the Ethics in Research Committee at UNIFESP/HSP, CEP protocol number 001/2007.
Fifteen patients, 25 to 45 years old, with second and third degree hemorrhoids were admitted at Hospital Municipal Vereador José Storopolli of Federal University of São Paulo (UNIFESP). Eight patients had three piles, six patients had two, and one patient showed a circular prolapse after sedation.
Patients received an intravenous injection of Propofol® 2.0 mg/kg (Biosintetica, São Paulo, Brazil) and local injection of 2% xylocaine. Medications were controlled by an anesthesiologist throughout the entire procedure.
Once the piles were identified, they were punctured and the laser energy (diode laser, Synus Laser Inc., São Paulo, Brazil) was delivered through an optic fiber of 600 μm (Fig. 1), emitting a wavelength of 810 nm, with nominal power of 5 W, frequency of 5 Hz, and energy fluence of 19 J/cm2, pulling the fiber gradually until the pile shrunk. Total amount of energy was 4 to 10 Joules.

Laser application inside the hemorrhoid.
Ten patients with hemorrhoids of the same degree received treatment by the conventional “cold scalpel” technique (Milligan–Morgan) and served as controls.
All procedures were performed by the same surgeon.
Results
Patients were discharged 3 h after surgery and followed for 1 month. They were instructed to resume normal activities 1 d after surgery. They were also instructed to take only sodium diclofenac (Voltaren®, Novartis, São Paulo, Brazil) 100 mg twice a day if they felt unbearable pain. No dressing, no antibiotics, and no special diet were prescribed.
Follow-up
Patients returned every week. There were no complaints of diarrhea or straining.
Pain
Pain scale ranged from 0 (no pain) to 10 (maximum pain) on a visual analog scale (VAS). All patients were instructed to check how much pain was felt every day on a standard table. For the laser group, the mean score was 0.84 ± 1.13 SD for the entire 28 d period. Two patients experienced intense pain; one at the first postoperative day and one showed an atypical curve pattern (Fig. 2A). Drug intake varied from once or twice a day for the first 3 d. Pain intensity mean for the patients of the conventional surgery group was 1.78 ± 0.68 SD (Fig. 2B) and drug intake varied from two to three tablets a day for at least 5 d. This difference was statistically significant by Mann–Whitney test (Table 1).
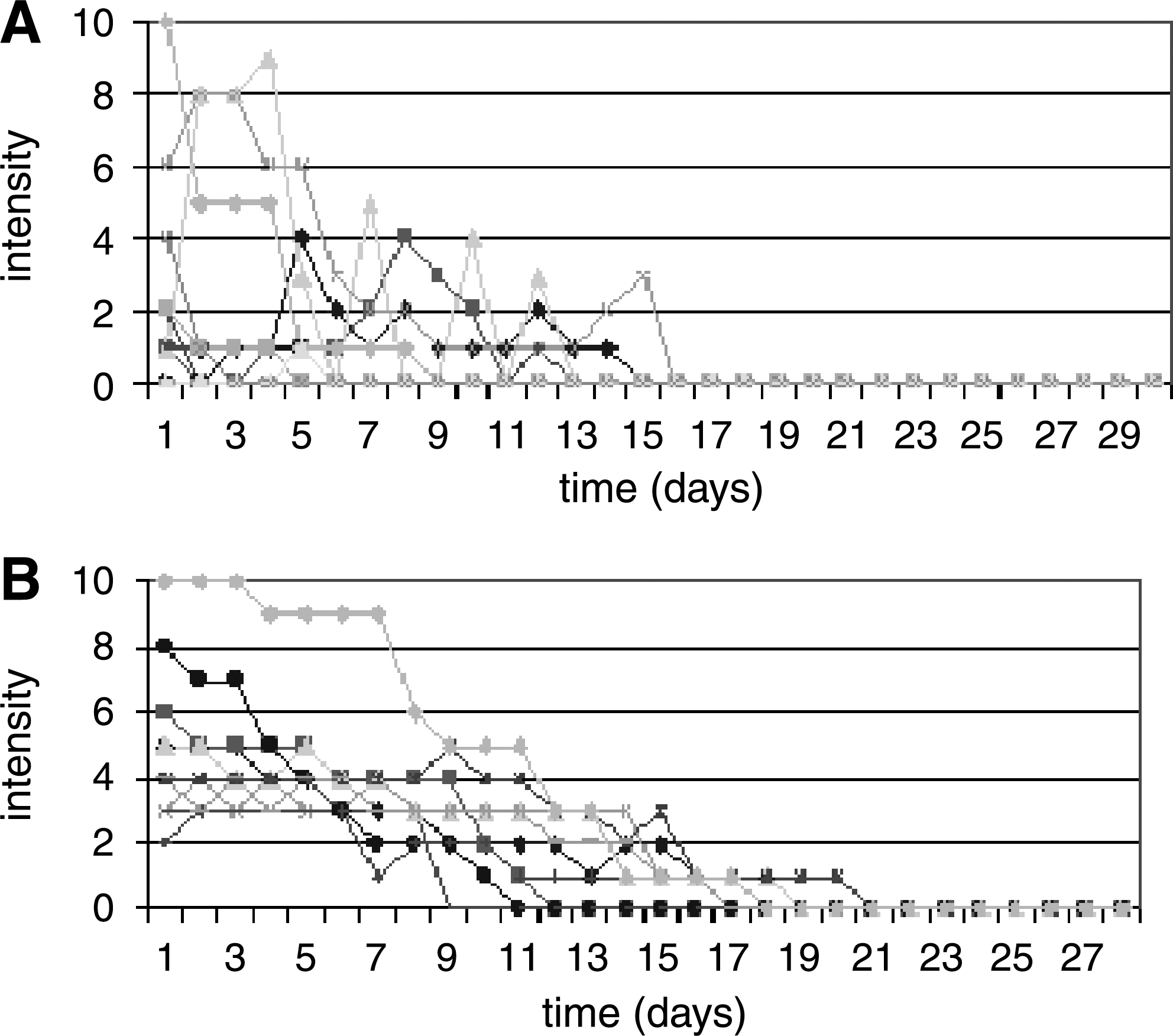
Intensity of postoperative pain: (
Average score over 28 days.
Mann–Whitney test.
IL, inferior limit; SL, superior limit; CI, confidence interval; SD, standard deviation.
Comparing the pain score between three different times (0–3, 4–11, and 12–28 d), the endolaser group showed significantly lower values (p = 0.001) compared to the conventional surgery group (Table 2). Both groups showed a reduction of the pain intensity score by the Friedman test (Fig. 3). 22
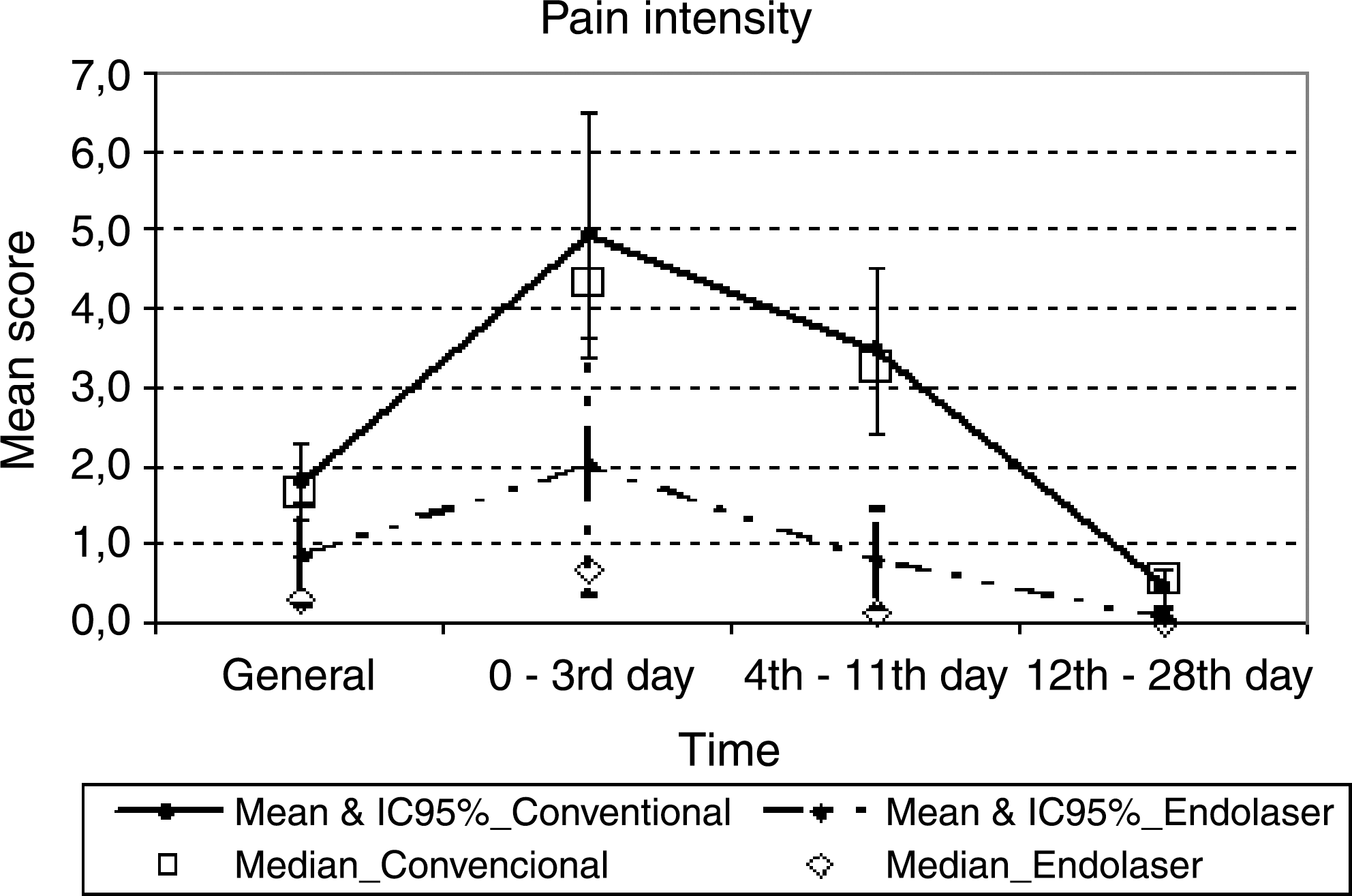
Median, mean, and 95% confidence interval (95% CI) of the mean score for pain intensity for each time interval (0–3, 4–11, 12–28 d postoperative) and for each group.
Mann–Whitney test.
Scars
Four patients in the laser group had postoperative scars which healed after 1 week (Fig. 4). Patients from the conventional surgery group had no scars (surgical bed was laid open).

Postoperative scar.
Plicoma (skin tag)
Plicoma was the most common complication and occurred in five patients (Fig. 5) from the endolaser group. No patient from the conventional group experienced this complication.

Postoperative plicoma (skin tag).
Discussion
Since Milligan et al. 23 described their open surgical technique, surgeons have disagreed about the best method to treat hemorrhoids. Surgical techniques have included rubber band ligation, stapling, liquid nitrogen, infrared light, ultrasonic scalpel, conventional open or closed surgery, and laser therapy. All aim to decrease pain and to improve healing in the postoperative period.
Endovenous ablation of varicose veins 24 is a new concept in vascular surgery. This technique could be used in all veins and opens up new possibilities for treating lesions such as “port wine” hemangiomas and even hemorrhoids. Navarro et al. 18 and Min et al. 25 achieved 100% and 99% sealing of the safena magna, respectively, using this technique. Plapler, 20 in an experimental model, achieved 100% shrinkage of three hemorrhoidal piles in monkeys.
In the present study, the resolution index was 93.4%, although five patients remained with plicoma. No plicoma occurred in the control group, since in the open technique this would happen only weeks after healing. Plapler et al. 12 reported a 20% incidence of plicoma in 350 open hemorrhoidectomies using a CO2 laser.
Scars occurred because of burn lesions in four patients. No other authors have reported this complication, but it is clear that experience leads to expertise. The more energy is applied for too long or too close to the mucosa, the greater the chance of causing damage. However, even these patients felt no unbearable pain during the entire study period.
Pain is the most important symptom after hemorrhoid surgery. All but two patients reported little or no pain, even those left with scars or plicoma. One patient reported intense pain on the first day and another presented an inconsistent pattern of pain. Compared to standard technique, pain was significantly less in the endolaser group, mainly at the first 3 postoperative days. Between the 4th and 11th day pain decreased for both groups, with the endolaser group consistently showing significantly lower scores. After the 12th day, the healing process tended to be equal.
Karahaliloglu 21 suggested submucosal rather than endovascular application of a laser to treat hemorrhoids. In fact, the tortuous dilated veins that form hemorrhoids do not allow laser energy to be delivered inside the vessels; rather, it is delivered into the interstitial tissue. 19,26 Tissue retraction around the vessel immediately after laser application leads to a proper resolution of hemorrhoids.
Nd:YAG laser (wavelength = 1064 nm) is more often used to treat veins, but no author has used it intravenously. This laser energy penetrates up to 4 mm in depth, which could lead to serious damages to the sphincter and to the surrounding structures. Diode laser (wavelength = 810 nm) penetrates up to 2 mm, is better absorbed by hemoglobin, and consequently causes less damage to the surrounding tissues. A new 1470 nm diode laser will be tested soon.
Surgical treatment of hemorrhoids remains an open field and more experimental and clinical studies are needed for better analysis. Endolaser techniques must be improved, and surgeons must become familiar with them. Although another group served as controls, the techniques were not really comparable since they dealt with different healing processes.
Conclusion
Intrahemorrhoidal laser application enabled a decrease in patient's discomfort with apparently little postoperative pain. It is a good method for small and medium size hemorrhoidal piles, but is not the best choice for big piles.
Footnotes
Acknowledgments
We are grateful to Prof. Dr. Rita de Cássia Rodrigues, Director of the Hospital Municipal Vereador José Storopolli of Federal University of São Paulo (UNIFESP) and her staff.
Disclosure Statement
No competing financial interests exist.