
Abstract
Introduction
Complications in flap viability can arise from several causes. For example, damage to the nutrient vessel of an axial pattern flap can result in ischemia or venous congestion, and hematoma formation or infection can lead to necrosis of all or part of the flap. 2 Attempts to maximize flap survivability include interventions such as improving the nutritional status of the patient, avoiding excessive electrocautery, ensuring adequate hemostasis, and avoiding crush injury or shearing forces to the flap from rough handling. 2 Innovative therapies, mainly with the aim of increasing blood flow to the flap, have been investigated including low-level laser therapy (LLLT). 3
Many authors have showed the positive effects of LLLT on the viability of skin flaps. 3 –5 The effects of laser are based on the stimulation of mitochondrial activity by the light, which increases cell proliferation, promotes fibrin absorption from injured tissue, and enhances the conversion of myofibroblasts from fibroblasts, which could explain the enlarged surviving area of the skin flap after laser irradiation. 6 Moreover, it has been demonstrated that laser irradiation can stimulate angiogenesis in the flap area and produce an adequate blood perfusion, 3,7 which is an essential part of the healing process. Additionally, the re-establishment of the circulation at the injury site limits ischemic necrosis and permits repair. 8,9
In spite of the number of works demonstrating the positive effects of LLLT on skin flap viability, a standard treatment protocol is lacking and a wide range of doses is used by different authors. For example, some of the works 4,5 found a decrease in the necrotic area with doses as low as 3 J/cm2 while others 3 found the same effect using higher doses, such as 24 J/cm2. Consequently, the optimal dose and wavelength able to increase flap viability are still controversial.
The use of LLLT on skin flap regeneration has increased in recent years; however, the knowledge about the mechanisms by which laser therapy acts remains limited. 9,10 Moreover, studies exploring the effects of different power, energy densities, and wavelength dependency, especially in in vivo models, are rare. 11,12 Before LLLT can be used with confidence as a therapeutic modality, it is necessary to investigate the effects and dose–response characteristics of this therapy to definitively determine its safety and efficacy.
We were not able to find any study investigating the effects of higher doses on skin flap viability. Thus, the aim of this study was to determine the necrotic area of the skin flap in rats after 660 nm and 780 nm laser irradiation at doses of 30 and 40 J/cm2.
Methods
This study was conducted in accordance with the Guide for Care and Use of Laboratory Animals and approved by the Animal Ethics Committee of the Federal University of São Carlos. Sixty adult male rats (Wistar, 12 weeks old, 260–320 g) were randomly divided into five groups, with 12 animals each: group 1 (control group), group 2 (irradiated with 660 nm laser, 30 J/cm2), group 3 (irradiated with 780 nm laser, 30 J/cm2), group 4 (irradiated with 660 nm laser, 40 J/cm2), and group 5 (irradiated with 780 nm laser, 40 J/cm2).
All animals were anesthetized with ketamine (95 mg/kg) and xylazine (12 mg/kg) intraperitoneally and depilated. A random skin flap measuring 10 × 4 cm was raised with a cranial base on the back of each rat. 5 A plastic barrier with the same dimensions was placed between the flap and its donor site. Flaps were closed with simple nylon 4-0 stitches (Fig. 1).

Skin flap.
Laser irradiation was performed immediately after the surgery and on days 1, 2, 3, and 4 post-surgery. A low-energy 660 nm and 780 nm laser (Twin Laser®, MM Optics, São Carlos, Brazil), continuous wave (CW), 4 mm beam diameter, 40 mW was used. The laser irradiation was made at the fluences of 30 J/cm2 (30 sec, total energy of 28.8 J) and 40 J/cm2 (40 sec, total energy of 38.4 J). Twenty-four points on the skin flap surface and surrounding it were irradiated through the punctual contact technique (Fig. 2). Irradiation was performed with a plastic template on the skin flap with demarcation points for each group. 3
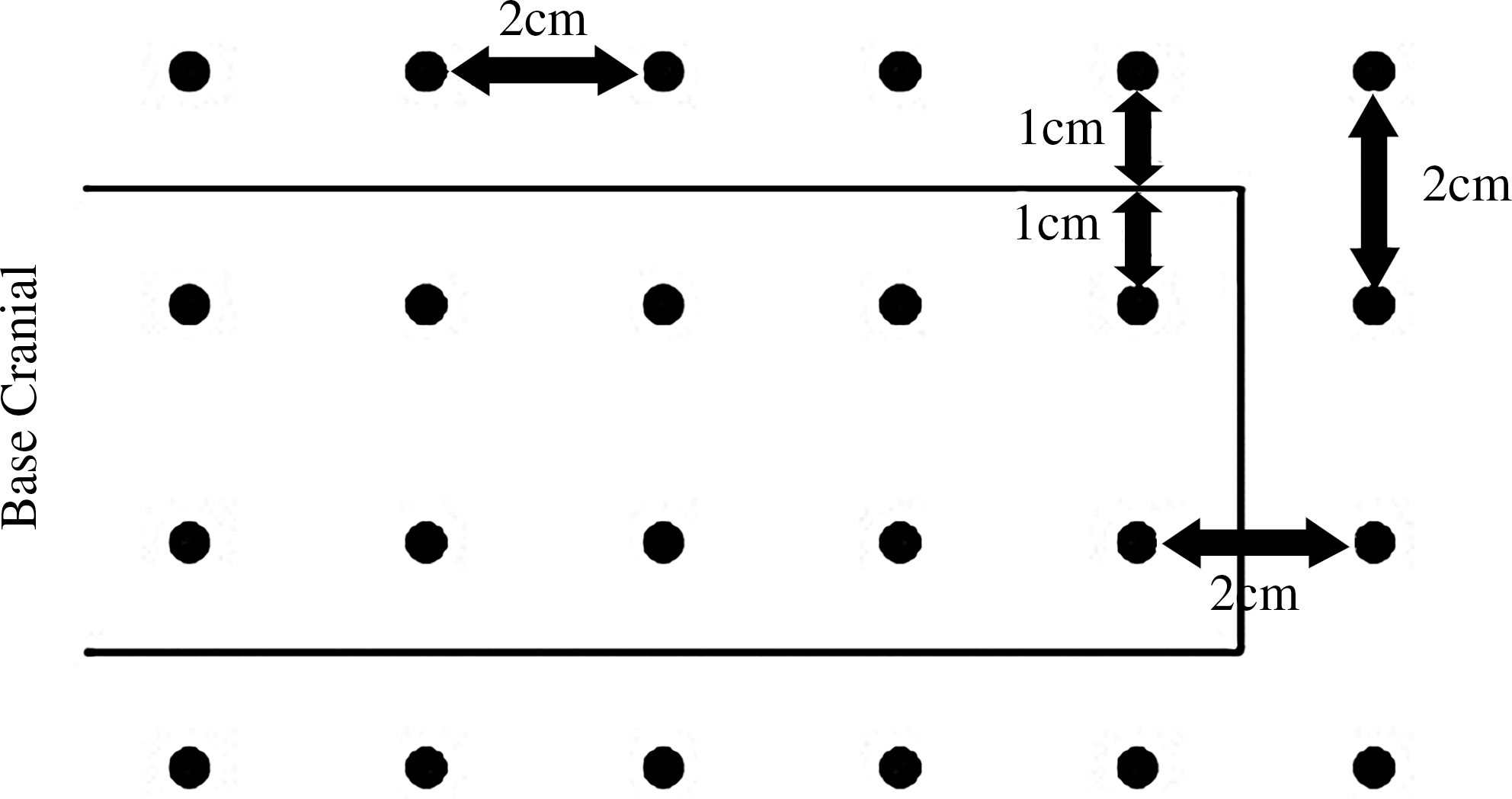
Scheme of laser irradiation on 24 points.
Analysis
Skin flap necrosis
The percentage of the skin flap necrotic area was calculated on the seventh post-operative day through the paper-template method. Rats were sedated and the limit between viable tissue characterized by soft skin (reddish, warm, and haired) and necrotic tissue (stiff, dark, cool, and hairless) was demarcated on the animals.
3
A mold of the entire flap and the necrotic area was drawn and cut in transparent paper, which was checked in a precision balance (0.001 g error). After that, the following equation was used:
After this procedure, the rats were humanely killed by an overdose of general anesthetic to verify the area of necrosis.
Statistical analysis
The results are given in means and standard deviations. The ANOVA (variance analysis) was used to verify the differences among the groups. A p level of ≤0.05 was considered statistically significant.
Results
Table 1 shows the means and the SD of the necrotic area found for each group and the results of the statistical analysis. Nonirradiated animals (control group) showed a mean necrotic area of 62.83%. Interestingly, no statistically significant differences were seen among the irradiated treated groups and the control group (p = 0.1737). The 780 nm laser at 30 J/cm2 (group 3) produced a minor, through consistent, trend towards a decrease in the necrotic area (54.6%); however, the value was not statistically significant.
G1, control; G2, 660 nm, 30 J/cm2; G3, 780 nm, 30 J/cm2; G4, 660 nm, 40 J/cm2; G5, 780 nm, 40 J/cm2.
NS, nonsignificant.
Discussion
We have investigated the effects of the two different laser wavelengths and two different doses on skin flap viability. Unfortunately, our results showed that none of the wavelengths and doses used produced any effect on the necrotic area of the flap.
Our findings do not corroborate those studies found in the literature, which have demonstrated that laser therapy effectively decreases the necrotic area of the flap and increases flap viability. 3 –5 Pinfildi et al. 5 and Amir et al. 13 found decreased tissue necrosis of the skin flap after 632.8 nm laser irradiation at a fluence of 3 J/cm2 and 2.9 J/cm2, respectively. Bossini et al. 3 investigated the effects of different 670 nm laser fluences in the necrotic area and in blood vessel growth, using the same protocol used in the present study, and demonstrated a dose–response curve for flap viability. They found a lower necrotic area and a higher number of blood vessels after the irradiation with 3, 6, 12, and 24 J/cm2, with the better response at the higher dose. 3
In spite of our lack of results after laser irradiation, our findings further support the notion of cell/tissue and dose/wavelength specificities in response to laser therapies. For example, Meireles et al. 14 found that a laser with 660 nm energy at a dose of 20 J/cm2 was more effective than the 780 nm laser on accelerating the healing of third-degree burns in diabetic rats. Moore et al. 15 observed increased fibroblast proliferation after 665 nm and 675 nm laser irradiation, whereas a 810 nm wavelength was inhibitory. In another study, Pinheiro et al. 16 reported that 635 nm laser irradiation did not stimulate proliferation of laryngeal carcinoma cells whereas 670 nm laser irradiation did.
Laser therapy involves a wide range of complex parameters such as wavelength, total fluence, fluence rate, coherence, pulse structure, and continuous wave. 11,17 One of the most important points that has been demonstrated by multiple studies in cell culture, 12,18 animal models, 19 and clinical studies is the concept of a dose–response relationship with the total delivered light energy density. 11 In addition, it has been postulated that there is an optimal dose of light for any particular application, and doses lower or higher than this optimum value will have a diminished therapeutic outcome and higher doses may even result in a negative outcome. 11,18
It is possible that the 670 nm and 780 nm laser irradiation may not have triggered any change in tissue metabolism in the skin flaps, thus failed to demonstrate alterations in the necrotic area of the treated groups compared to the controls. Also, we can suggest that the amount of energy administered to the tissue was higher than the optimum dose necessary to produce an increase in flap viability. As observed in a previous study by our group, 3 the dose of 24 J/cm2 was effective for increasing flap viability. The dose of 30 and 40 J/cm2 may have been excessive and could have promoted an inhibition of fibroblast cell proliferation and neoangiogenesis, consequently preventing an increase of skin flap viability.
Despite our results, we consider the methodology employed in this study comparable with previous reports found in the literature. 3 –5 The plastic film used between the flap and the donor site avoid the revascularization of the flap through donor site vessels, assuring homogeneous ischemia. 20,21 In addition, the paper-template method and the punctual contact technique of irradiation used were also adequate. 3
We should point out some limitations of our work. Many authors suggest that laser therapy increases the development of new blood vessels and blood flux. 19,22 These effects are an essential part of the healing process and the re-establishment of the circulation at the injury site limits ischemic necrosis and permits repair. Therefore, the inclusion of the measurement of the formation of new blood vessels (arteries or capillaries) and the blood flux would give more specific information about the distribution of the blood flow.
Our data are useful for establishing treatment parameters; however, they highlight the need for further investigations about the mechanisms of action of laser and the safe dosage regime and wavelength combinations for clinical application.
Conclusion
The present study demonstrated that 660 nm and 780 nm wavelength irradiation at the doses of 30 and 40 J/cm2 did not have any effect on skin flap viability. These data highlight the importance of using adequate laser wavelength and dosage to elicit the best tissue response. Studies investigating the effects of different fluences of laser on tissue repair are important in determining the efficacy of laser therapy. Further studies are required to investigate possible response mechanisms of action that may explain the effects of laser on skin flap viability.
Footnotes
Disclosure Statement
No competing financial interests exist.