
Abstract
Introduction
One of the factors that can moderate caries development is the presence of fluoride in the oral environment. Fluoride acts by reducing the critical pH for enamel dissolution from 5.5 to 4.5, thus enamel is able to resist a higher acid challenge. 2 Fluoride may be found in drinking water, toothpastes, mouthwash solutions, and varnishes, and is also released from restorative materials. Fluoride-releasing restorative materials are indicated to prevent secondary caries development in high-risk patients. 3 –5
The potential cariostatic effect of restorative materials is described for research that has shown high cariostatic effect of conventional glass ionomer cements, moderate cariostatic effect of glass ionomer and composite resin hybrid materials, and no cariostatic effect of composite resin materials. 3,4,6,7
On the other hand, few studies have suggested the use of lasers to modify dental enamel structure and improve its acid resistance. The first laser recommended for caries prevention was the CO2 laser, followed by Nd:YAG, Er:YSGG, and Er:YAG lasers. 8 Because of coincident band absorption by water and hydroxyapatite, CO2 and erbium lasers efficiently heat the enamel surface to temperatures sufficient to inhibit acid dissolution and can prevent up to 80% of enamel dissolution in the face of an acid challenge with energy densities below the enamel ablation threshold. 9,10
Ablation is a phenomenon that occurs during laser irradiation when the laser energy is absorbed selectively by water molecules and hydrous organic components of biological tissues. This causes evaporation of water and organic components and results in thermal effects due to the heat generated by the process. Additionally, the production of water vapor increases the internal pressure within the tooth tissue, resulting in microexplosions that cause dental tissue removal. 11
Ablative parameters are used to perform cavity preparations, and although it requires more clinical time, patients perceived laser as more comfortable, without vibratory and auditory irritation and with a significantly reduced need for local anesthesia compared to mechanical means. 12 Fried et al. 9 suggested that an advantage of the Er:YAG lasers among high intensity lasers is the enamel ablation mechanism, which is primarily based on the principal absorber not being in hard tissue. They reported that primary absorption in water results in water-mediated ablation, and primary absorption in the bulk of enamel rods results in melting and vaporization. 9 The absorption of the Er:YAG lasers by inorganic components (hydroxyapatite) is much lower than that of other lasers, such as CO2 laser. 13 Thus, the absorption in water and hydrous organic components occurs rapidly before heat accumulation caused by absorption in inorganic components takes place, resulting in thermo-mechanical, explosive ablation. 13
Although the energy densities used for cavity preparation are higher than densities used for caries prevention, some heat is generated at the cavity margins during ablation. However, it is not known if this heat accumulation would be enough to thermally modify the enamel and improve its acid resistance. This theory can be extrapolated from the results of studies that showed a tendency towards increased caries resistance after subablative erbium laser irradiation 14 and low energy densities of Er:YAG laser can decrease enamel solubility, as well as a clinical trial that showed that after 6 months, cavities prepared with Er,Cr:YSGG presented no secondary caries at the margins of the preparation sites. 15
Many studies have shown the caries preventive potential of Er:YAG laser but the articles were focused on the use of subablative parameters. It is not known whether the heat accumulation during cavity preparation could provide some acid resistance to the enamel surface around cavity margins or whether this possible improvement in acid resistance could act synergistically with restorative materials that release fluoride for the prevention of caries development. Therefore, the aim of the present study was to investigate the effect in vitro of cavity preparation with Er:YAG laser on inhibiting enamel demineralization around fluoride-releasing adhesive restorations.
Methods and Materials
Since this study was performed using human third molars, the research protocol was submitted to the Research Ethics Committee of the Guarulhos University and was approved in accordance with the resolution CNS# 196/96 of the National Health Committee/Health Department (Brazil).
Experimental design
The experimental units consisted of 72 dental slabs (n = 12 per group) obtained from 40 unerupted human third molars. The factors under study were method of cavity preparation (at two levels) and restorative material (at three levels) in a factorial design (Table 1). The response variable was surface microhardness in Knoop hardness number (KHN).
Preparation of dental slabs
Following extractions, teeth were stored in a 0.1% Timol solution (pH 7.0) for no more than 30 d. 16 Soft tissues were removed using periodontal curettes (HU-FRIEDY do Brasil, Rio de Janeiro, Brazil) and cleaning was performed using a slurry of pumice in a webbed rubber cup applied with a slow-speed handpiece (Kavo do Brasil, Joinville, Brazil). The roots were removed, and the crowns were longitudinally and transversally sectioned by using double-faced diamond discs (no. 7020; KG Sorensen, São Paulo, Brazil) to obtain 72 dental slabs measuring 4 × 4 × 3 mm3.
Cavity preparation and restoration
Standardized circular cavities were prepared in the enamel slabs. Half of the samples were prepared with diamond burs. Cavities of approximately 1.6 mm in diameter and 1.6 mm deep were prepared at high speed with no. 2292 diamond burs (KG Sorensen, Barueri, SP, Brazil) under a constant water spray coolant.
The other half of the samples were irradiated using the Er:YAG laser (KaVo Key II; KaVo, Biberach, Germany) working at 2940 nm. The output power and pulse rate ranged from 60 to 500 mJ and from 1 to 15 Hz, respectively. Working at a distance of 12 mm from the tooth surface (focused mode), a handpiece (no. 2056) with a 0.63 mm spot size, and energy of 300 mJ with a repetition rate of 6 Hz was used to prepare the cavities under continuous water spray (5 mL/min). The energy density was approximately 47 J/cm2 and cavities were standardized by visual and contact comparisons to no. 2292 diamond burs used for mechanical preparation.
After the cavity preparations, the slabs were randomized among the restorative material subgroups (Table 1) and the cavities in 12 blocks were restored, with one sample of each group, in one increment, according to the manufacturer's instructions.
In cavities filled with Ketac-Fil, the Ketac conditioner was applied for 10 sec, rinsed, and dried for 10 sec. Ketac-Fil was prepared within 20–25 s, inserted in the cavity with a Centrix injector, protected with a mylar strip (Dentart, Polidental, São Paulo, Brazil; dimension 10 × 120 × 0.05 mm3) for 5 min, coated with Vitremer Finish Gloss and light-activated for 20 sec by an Optilux 501 light unit (Demetron/Kerr, Danbury, CT, USA). The power density was measured by placing the light tip at the radiometer of the light unit. The light curing unit had a light tip diameter of 11 mm with an irradiance of 700 mW/cm2.
In cavities filled with Vitremer, the Primer was applied for 30 sec, dried for 5 sec, and light-activated for 20 sec. Vitremer was prepared within 45 sec, inserted in the cavity with a Centrix injector, light-activated for 40 sec, coated with Vitremer Finish Gloss and light-activated for 20 sec.
In cavities filled with Z-250, the 3M Scotch Bond etchant was applied for 15 sec, rinsed for 10 sec, and air-dried. Two coats of 3M Single Bond were applied, air-dried for 5 sec, and light-activated for 10 sec. The composite resin was inserted and light-activated for 20 sec.
All restored slabs were stored in 100% humidity for 24 h and then polished using the Sof-lex (3M ESPE) disks system for 15 sec with each disk.
Thermal and acid challenge
The slabs were placed into separate bags with 1 mL of deionized water and thermal cycled together for 1000 cycles in water between 5 ± 2°C and 55 ± 2°C with a dwell time of 2 min in each bath and a 15 sec transfer time between baths. 3 All external surfaces of each slab were coated with wax, leaving a 1.5 mm wide margin around the restoration free of wax.
The test scheme for acid challenge was designed to model a daily demineralization challenge of a 6 h and a 18 h repair (remineralization) by saliva as described by Featherstone et al. 17 and Serra and Cury, 18 with the aim of simulating a high in vitro caries risk and producing artificial caries-like lesions around the restorations. 2,7,19,20
The demineralization stage used an acid buffer containing 2 mmol/L calcium, 2 mmol/L phosphate, and 0.075 mol/L acetate at pH 4.3. The remineralization solution contained calcium and phosphate at a known degree of saturation (1.5 mmol/L calcium, 0.9 mmol/L phosphate), to mimic the remineralizing properties of saliva, and 50 mmol/L KCl, 20 mmol/L tri-hydroxymethylaminomethane buffer at pH 7.0. 17,18 The slabs were immersed separately in 15 mL of demineralization solution for 6 h, immersed in 15 mL of remineralization solution for 18 h, washed, and again immersed in demineralization solution, thereby initiating a new cycle. The pH cycles were conducted for 14 d with 10 daily cycles. In the 6th, 7th, 13th, and 14th days of the cycle, the slabs were kept only in the remineralization solution.
At the end of the pH cycles, the wax was eliminated and the slabs were stored at 100% humidity until the microhardness test.
Microhardness test
The demineralization of the restored enamel slabs was assessed with a microhardness tester (PanTec, Panambra Ind. e Técnica SA, São Paulo-Brazil) and a Knoop indenter. The indentations were made keeping the long axis of the diamond instrument parallel to the outer-leveled enamel surface, using a 25 g load applied for 5 sec, and the value in micrometers of the higher diagonal was measured and automatically changed to KHN by the microhardness tester. Four measurements were made at 100 μm intervals around the restoration margins in the upper, left, right, and bottom sides (Fig. 1).
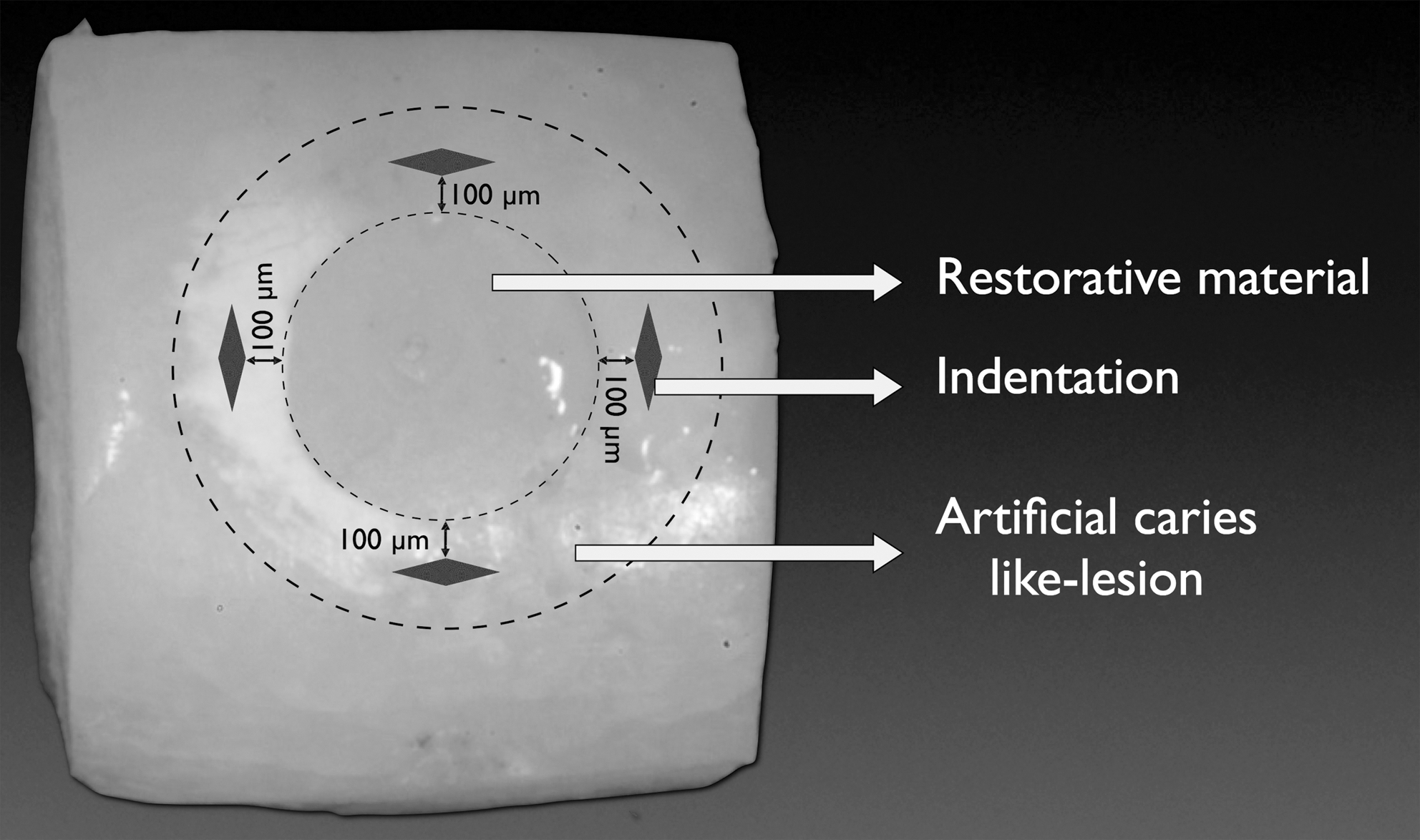
Location scheme for microhardness test.
Results
The mean microhardness values and standard deviations per restorative material in each cavity preparation are presented in Table 2. Data were changed to √x to obtain a normal distribution and were submitted to ANOVA considering the factorial 3 × 2 model to observe the factors and their interactions. There were statistical differences in the factors restorative materials and method of cavity preparation (p <0.00001); there was no interaction between the factors restorative materials and method of cavity preparation (p = 0.3181).
Means followed by the same lower case letters in the row indicate no statistical difference (Tukey's test, p < 0.05) and different upper case letters indicate mean values that are statistically different in the column (analysis of variance, p < 0.05).
The microhardness of enamel around cavities filled with glass-ionomer cement showed the highest microhardness values, differing significantly from the cavities restored with resin-modified glass-ionomer, which showed intermediate values. The cavities filled with composite resin showed the lowest value (Table 2). The cavities prepared with Er:YAG laser showed significantly higher microhardness values than the diamond bur cavities.
Discussion
Lasers with wavelengths that interact with water and hydroxyapatite allow the conservative removal of caries lesions and cavity preparation, and can also change the solubility of enamel, improving its acid resistance. 9,10,14,15 This study evaluated the development of artificial caries lesion on enamel around cavities prepared with diamond burs and Er:YAG laser, and filled with restorative materials with or without fluoride-releasing properties, using a dynamic cyclic model of demineralization and remineralization, whose acid challenge was correlated to patients with high caries risk. 17
The highest development of artificial caries lesions in this study was observed in groups restored with composite resin, which was expected because the composite resin or adhesive system used did not contain fluoride in their compositions. 3 This is consistent with reports from other studies, in which only composite resins and adhesive systems containing fluoride or antibacterial monomers were capable of showing an anticariogenic effect, which is lower than that of glass ionomers. 5,19
During acid challenges glass ionomer cements mobilize and release increased amounts of fluoride into the environment. The presence of fluoride continuously released by these restorative materials is an important feature for facilitating the reprecipitation of minerals, improving remineralization, or inhibiting demineralization. 2 This is the reason for less artificial caries lesion development around cavities restored with conventional glass ionomer cement. 18,20,21 Therefore, the protection rendered by the glass ionomer cement is extended for some distance from the restoration and it is greatest in the cavity preparation area. 6
To a lesser extent than in conventional glass ionomers, the smaller concentrations of fluoride released from resin-modified glass ionomer caused moderate development of artificial caries lesion, but in comparison with glass ionomer cement, it resulted in less inhibition. 4
The statistical analysis of the factor cavity preparation showed more artificial caries development in cavities prepared with diamond burs than in the cavities prepared with the Er:YAG laser. Numerous in vitro studies using a variety of laser wavelengths within subablative parameters have been conducted to investigate caries prevention and showed this effect. 14,22 They have shown the potential of some wavelengths to be absorbed by hydroxyapatite and water in enamel and dentin, and the conversion of the irradiated energy into heat. This heat increase is considered to be the cause of the microstructural and chemical changes occurring in lased enamel and dentin 22,23 and explains the increased acid resistance due to the reduction in permeability by the evaporation of the organic matrix.
However, the potential of the Er:YAG laser irradiation in an ablative parameter to improve the acid resistance of enamel around the cavity preparation was not totally clear. 24,25 Chimello et al. 24 revealed that the Er:YAG laser did not differ from conventional cavity preparation, but in the present study the enamel adjacent to cavities prepared with the Er:YAG laser showed less development of artificial carious lesion. 26 The mechanisms by which lasers can improve the tooth acid resistance may be due to the absorption of heat and penetration into the nonablated enamel layers adjacent to cavity wall whose enamel was ablated during cavity preparation. 26
Thus, it can be supposed that the penetration of heat into the adjacent layers around the cavity walls may act in the same way as in the outer enamel with a reduction in organic matrix and enamel vitrification. 26 However, the present study was conducted with water cooling, which is recommended and indeed indispensable in order to avoid temperature damage to the dental pulp. 25 It is also important to point out that the present study selected safe parameters with regard to temperature increase in the intrapulpal region. According to Geraldo-Martins et al. 27 the samples irradiated with the Er:YAG laser using the same parameters as the present study achieved an intrapulpal temperature increase of 1.45° ± 0.64°C. It can be also speculated that heat caused by laser is restricted to the superficial layers of the irradiated walls, which can be a limiting factor for obtaining high acid resistance at some extended distance from the restoration margins.
Although group 1 (glass-ionomer cement/Er:YAG laser) followed by group 2 (resin-modified glass-ionomer/Er:YAG laser) showed the highest numerical means, the interaction of factors cavity preparation and restorative materials expected to have a synergistic effect between fluoride release and the increase in the enamel acid resistance by the Er:YAG laser was not found in this study.
As observed in the in vitro results, the use of Er:YAG laser in cavity preparations may be a suitable option for patients at high caries risk, by the increase in the enamel acid resistance and other advantages such as its microbial reduction potential and smear layer removal. 28 Although cavity sterilization and conditioning are obtained by Er:YAG laser irradiation, 29 some researchers showed the presence of a laser-modified layer that may adversely affect enamel and dentin bonding. This layer may obliterate enamel micropores, thus blocking the intra- and interprismatic spaces, restricting resin interdiffusion into the enamel surface. 30 –32 Moreover, the more acid-resistant lased surface might reduce the effectiveness of acid etching, and hybridization may be compromised. 32,33 In dentin hybridization, subsurface damage initiated by Er:YAG ablation may alter the subsurface under the hybrid zone and remnant denatured collagen fibrils may not be resistant to the forces from the polymerization shrinkage. Fractures may occur, leading to microleakage. 30,31
A negative influence on marginal sealing of composite resin restorations with a total etch adhesive system after Er:YAG laser use has also been shown in microleakage studies. 30,31 However, results are poor and contradictory, and other research found no differences in the microleakage of composite resin, glass ionomer cement, or resin-modified glass ionomer restorations etched or prepared with Er:YAG laser. 34 –36 Only Hadley et al., 12 in in vivo research, observed the performance of composite resin restorations in 66 cavities prepared with Er,Cr:YSGG (68.1 J/cm2), in comparison with 66 cavities prepared with diamond burs. After 6 months all restorations were retained and no secondary caries were observed.
In order to avoid secondary caries, not only the improvement of dental acid resistance is necessary 4 but further studies are needed regarding Er:YAG laser parameters to achieve the ideal association with adhesive systems to produce an adequate hybrid layer to avoid the microleakage phenomena and improve dental acid resistance. However, the use of Er:YAG laser in cavity preparation may be useful and effective in the prophylaxis and management of patients at high risk for dental caries, and the present study showed less caries development around cavities prepared with Er:YAG laser than bur preparation. In vivo studies are necessary to confirm these in vitro results and to verify the performance of the restorative materials inserted in these cavities.
Conclusions
The cavity preparation with Er:YAG laser may lead to an increase in the acid resistance in the enamel layers surrounding cavity walls, irrespective of the presence of fluoride in the restorative material. The high cariostatic effect was observed with conventional glass ionomer followed by the resin-modified glass ionomer with a moderated cariostatic effect. The composite resin showed no cariostatic effect. No synergistic effect between glass ionomer cement and laser was observed.
Footnotes
Disclosure Statement
No competing financial interests exist.