
Abstract
Introduction
Materials and Methods
We retrospectively reviewed the clinical and radiological data of fourteen patients with discal cysts of which the pathologies were confirmed between May 2005 and July 2008. Eleven of the patients were men and three were women, with a mean age of 35.5 (range, 14 to 70) years. All patients had had radicular pain or numbness along the dermatome, corresponding to the nerve root. The average duration of symptoms was 15.4 (range: 3 to 27) months. All of them had preoperative radiography and lumbar CT scans, as well as magnetic resonance imaging (MRI) of the lumbar spine. The patients were assessed using the visual analogue scale (VAS) and Oswestry Disability Index (ODI). All patients were followed postoperatively and underwent repeated physical examinations for pain, function, and neurological damage. Complications after surgery were assessed as infection (deep or superficial), any permanent residual neurological damage, dural tears, or other complications.
A paired Student's t test was used to compare preoperative and postoperative clinical outcomes, and p < 0.05 was considered to indicate a statistically significant difference.
Surgical technique
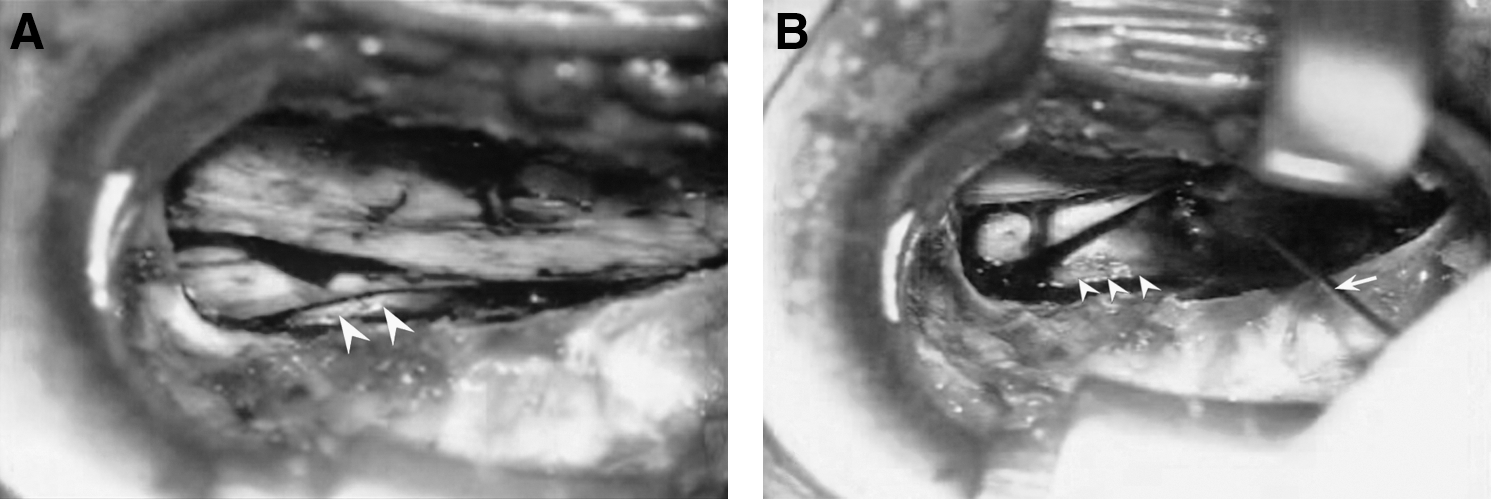
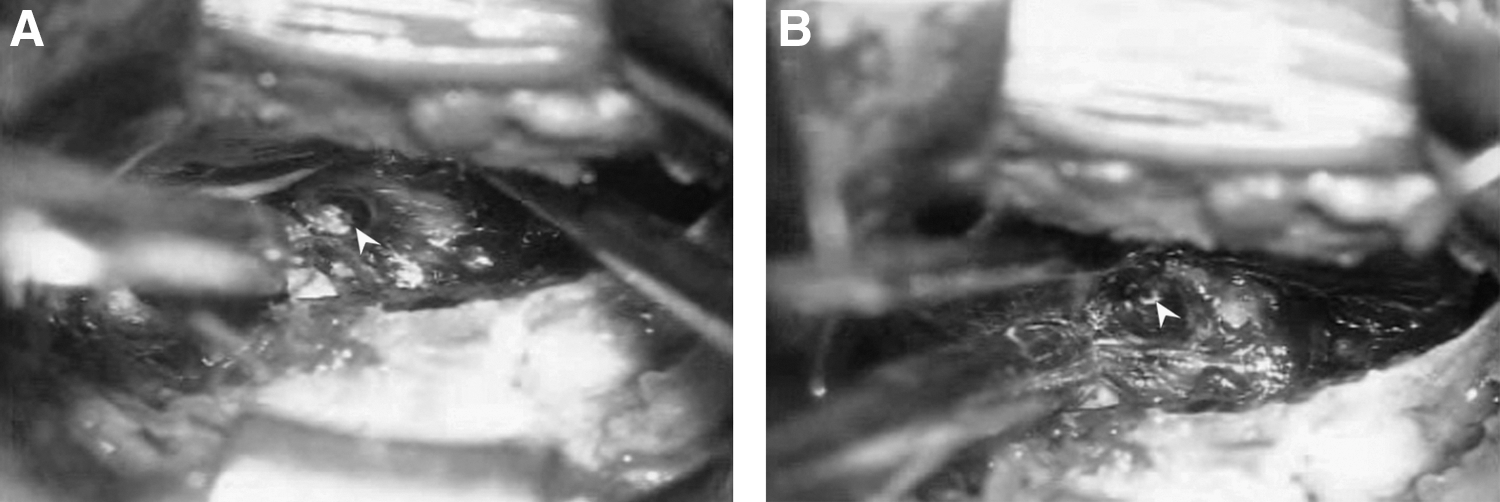
Most procedures were similar to those of conventional microdiscectomy. A small partial laminectomy, with or without foraminotomy, was performed under the operating microscope. The ligamentum flavum was removed and the affected discal cyst was exposed by gentle retraction of the thecal sac and traversing nerve root. Most epidural veins around the discal cyst were coagulated by a bipolar coagulator, and the traversing nerve root and discal cyst were exposed (Fig. 1A). Using a mixture of radio opaque dye (Telebrix), indigo carmine (Carmine), and normal saline mixed in a ratio of 2:1:2, discography was performed. Just after injection of the dye into the disc space, the reddish fluid-filled discal cyst turned to the purple color of indigo carmine, meaning that there is communication between the discal cyst and the protruded disc (Fig. 1-B). Using a 22-gauge needle and a CO2 laser (Sharplan 30C, Lumenis, Yokneam, Israel), the discal cyst was penetrated. Then, the contents and wall of the discal cyst were removed with pituitary forceps. The surgeon then found a small hole between the discal cyst and the protruded disc (Fig. 2). By extension of this hole using the CO2 laser, the surgeon removed the extruded disc fragment and subsequent pulled-out disc fragment through this extended hole after pushing the disc space with a right-angled probe. No additional central discectomy was made in any case. Finally, annuloplasty was done to avoid disc reherniation through this hole.
(
(
Results
Illustrative cases
(
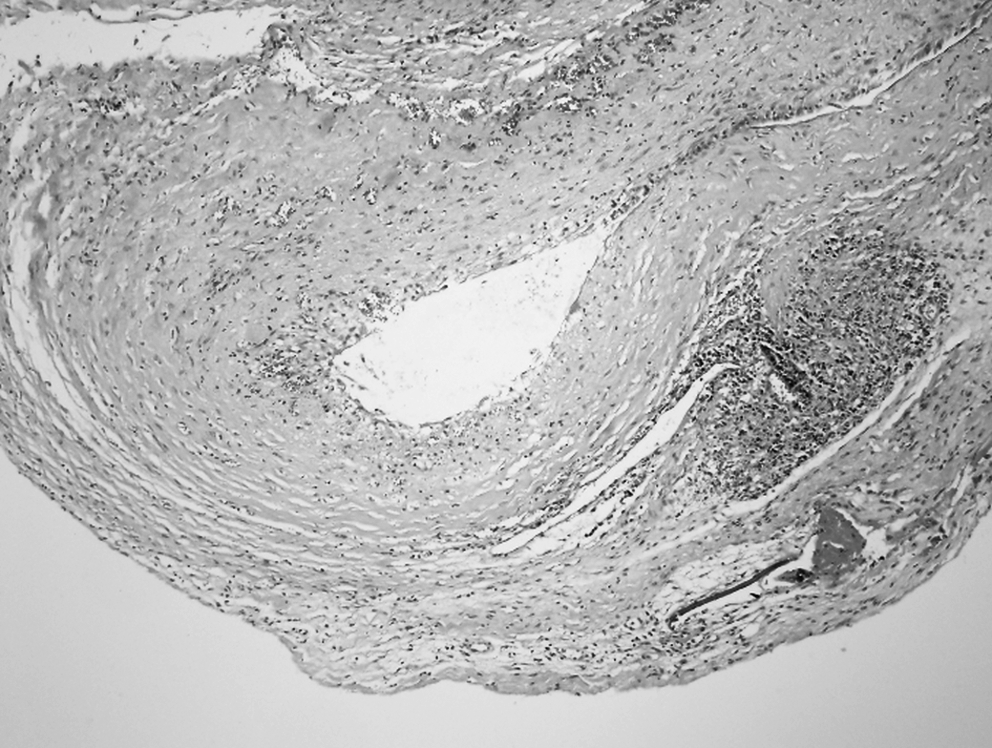
Histopathologic finding of cystic wall consisting of dense fibrous connective tissue without specific lining cells (H & E, × 10).

(
Clinical results for all patients are summarized in Table 1. The major symptoms were leg pain in all 14 patients (100%) and back pain in eight patients (57.1%). All patients presented with complaints of radicular pain in the affected dermatome. Physical examination demonstrated a positive straight leg raising sign on the lesion side in all patients. There was objective weakness of the leg muscle in the affected nerve root in 11 patients out of 14 (78.6%). One patient (No. 6) presented transient numbness and dysesthesia due to adhesion, which subsided after a selective root block procedure.
Abbreviations: asp, CT-guided aspiration; mos, months; F, female; M, male; LBP, low back pain; transf, transforaminal percutaneous approach.
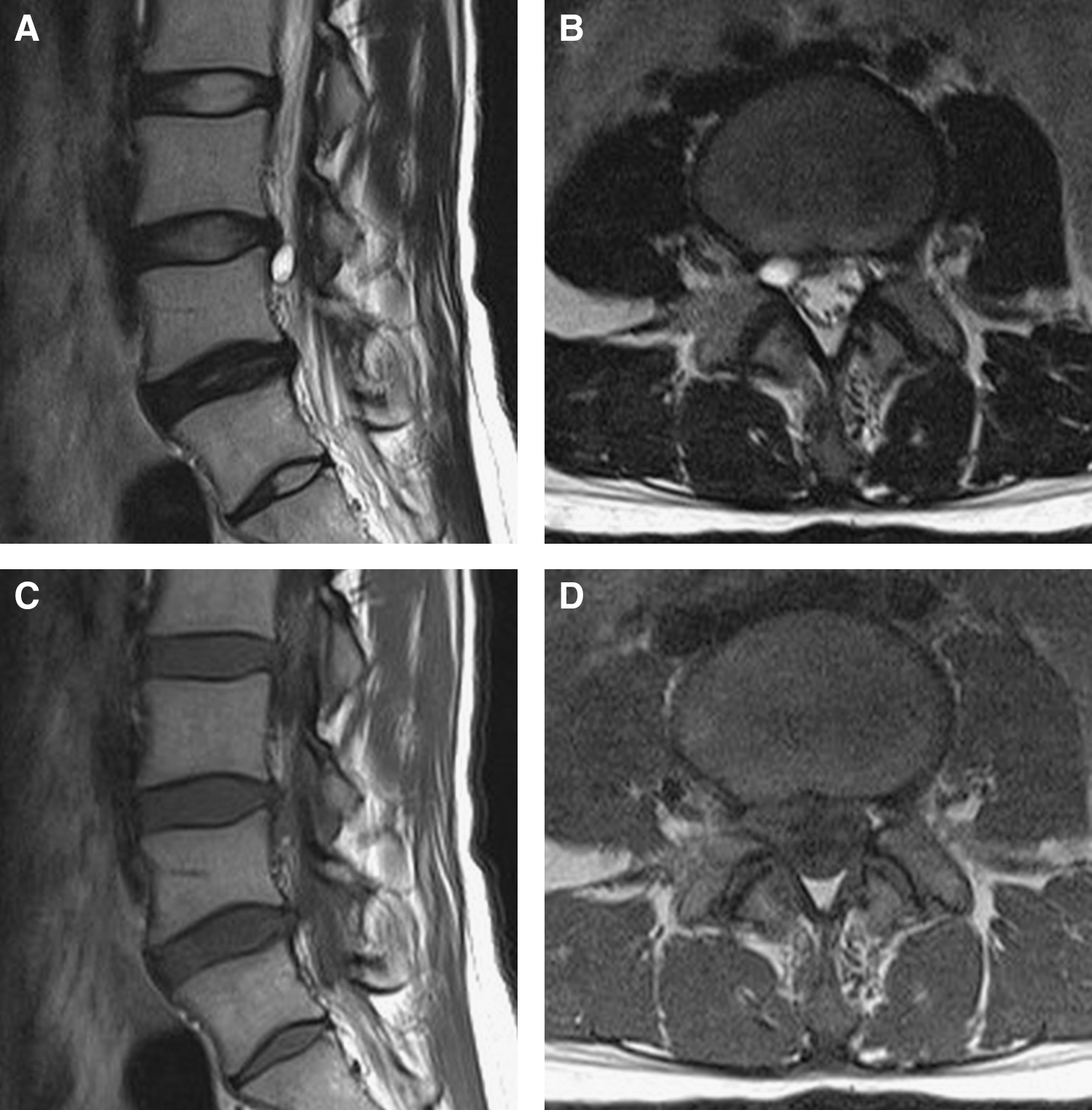
The cysts were located at the L4-5 level in six patients, at the L5-S1 level in four patients, at the L3-4 level in three patients, and at the L1-2 level in one patient. In all but three cases, the cysts were extradural oval masses with low signal intensity on T1-weighted MRI and high signal intensity on T2-weighted MRI. Three cysts showed high signal intensity on both T1- and T2-imaging and hemorrhagic content within these cysts was found during surgery. All surgically confirmed cysts were present in the ventrolateral extradural space under the corresponding nerve roots with mild adhesion to the dura mater or root. All the cysts had a reddish or white thick fibrous capsule and the content was serous or bloody fluid. We detected the presence of communication of the cyst with the adjacent intervertebral disc in all cases. One patient underwent CT-guided aspiration due to the remaining cyst.
All patients except for one (93%) who underwent partial hemilaminectomy and cyst resection successfully recovered. The success rate of the treatment method was 93% in the open surgical removal group. The mean preoperative VAS for leg pain was 8.1; this improved to 1.8 (p < 0.001), and the patients' mean score on the Korean version of the ODI had improved from 46.47% to 14.81% (p < 0.001) at the last follow-up. No complications occurred during follow up.
Discussion
Many kinds of cystic lesions have been reported in degenerative spine disorders, including synovial cysts, arachnoid cysts, perineural cysts, cysts of the ligament flavum, ganglion cysts, and discal cysts. 1,4 –9 Most cystic lesions develop in the connective tissue around the peripheral joint and tendon. However, discal cysts are not common and have rarely been reported in the literature. 3,10 –13
The clinical symptoms of a discal cyst are variable. However, the symptoms and signs of most of our series were indistinguishable from a lumbar disc herniation causing radicular leg pain. This was because most of the cysts were located ventromedially to the nerve root, compressing the root dorsolaterally.
According to the literature, 9 the characteristics of discal cysts are as follows. (1) All of the cysts are located caudally to the disc space. (2) The discs adjacent to the cysts also show degenerative bulging. There is associated disc degeneration and disc bulging in all cases. (3) In many cases, the direction of the cyst coincides with the direction of disc bulging.
It is supposed that disc degeneration plays an important role in the formation of the discal cyst. These findings are nearly compatible with our series. However, in patient 1, MRI demonstrated that the direction and location of the discal cyst was just cranial to the disc space. Hence, according to our series, “all” cysts appearing just caudal to the disc space should be changed to “most” cysts being just caudal to the disc space.
Chiba et al. 3 proposed that discal cysts arise first from an underlying intervertebral disc injury that causes an annulus fibrosis fissure in the posterior intervertebral disc. Hemorrhaging from the peridural venous plexus with a rich blood flow occurs in the space between the peridural membrane and the vertebral body because of the mechanical force transmitted by the annular fissure. In our series, three patients had experienced a definite trauma history: traffic accidents, lifting injuries, and slipping while playing sports. Three patients had occupations that required physical activity: basketball player, soccer player, and soldier. The mean age of the other patients was 35.5 years (range: 14 to 70); thus, the discal cyst developed at a physically active age. Interestingly, one patient (patient 8) who had experienced a trauma history already had disc protrusion at the initial MRI and had a traffic accident during the follow-up period; after this traumatic event, he was re-evaluated due to severe radicular pain, which demonstrated a newly developed discal cyst at the level of disc protrusion. This series strongly suggests that trauma on the degenerative disc may cause discal cysts, which corresponds to Chiba's hypothesis.
Many kinds of surgical methods have been introduced for the treatment of discal cysts. To date, surgical treatments, including open surgical excision 3,10 –12 and percutaneous CT-guided aspiration with or without steroid injection, 13–14 have been reported; the clinical outcomes of these treatments have been considered favorable. Other investigators 15 described the spontaneous regression of a discal cyst after epidural injection and a selective nerve block procedure. However, most reported discal cysts have been treated surgically or with some direct intervention such as CT-guided aspiration and steroid injection. Recently, it was reported that a discal cyst was treated with a minimally invasive technique, using the METRxTM (Medtronic Sofamor Danek, Inc., Memphis, TN) microendoscopic discectomy system; 16 a synovial cyst of the facet joint in the lumbar spine was treated using a percutaneous endoscopic transforaminal approach. 17 The researchers noted that excellent pain relief was achieved in patients by these minimally invasive procedures.
Since the first trial of Neodymium: Yttrium-Aluminum-Garnet (Nd: YAG) during lumbar disc surgery in 1986, 18 many reports about the usefulness of different kinds of lasers on disc surgery have been reported. 19 –22 Nerubay et al. reported that 50 patients with low back and radicular pain were successfully treated by percutaneous laser nucleolysis with a CO2 laser, 22 and successful vaporization of the disc was accomplished in animal models. 23
Considering the similarity between the disc and the meniscus, 24 we can cite studies on the effect of a CO2 laser on the meniscus. According to these researchers' results, there was a considerable proliferation of cells resembling chondrocytes after 2 weeks of CO2 laser treatment and there was definite increased production of ground substance and immature collagen fibers after four weeks; the collagen had become well reorganized into a logical orientation, resembling the normal architecture of fibrocartilage, after 10 weeks. 25
These animal studies and clinical studies strongly support the claim that CO2 lasers could safely and feasibly be used for the removal of discal cysts and protruded discs. Moreover, the CO2 laser, when attached to an operating microscope, allows for the quick and easy removal of the discal cyst and, if needed, easy vaporization of disc material.
There may be some debate as to whether the protruded disc is vaporized or not using the CO2 laser after removal of the discal cyst. Considering the pathogenesis of discal cysts, disc degeneration, including disc protrusion and bulging with annular tearing, may play an important role in the formation of the discal cyst. Preoperative MRI in our series always showed a degenerated disc with bulging or protrusion in conjunction with the discal cyst. Thus, after removal of the discal cyst, the authors found the communication hole between the cyst and protruded disc. They then used heat energy by CO2 lasering and removed the pulled-out disc fragment, if it existed, after pushing into the disc space with a right-angled probe. If there was no subsequent disc fragment after pushing the posterior annulus, no additional disc was removed.
Conclusion
In this study, fourteen cases of discal cyst that caused the same symptoms and signs as those of lumbar disc herniations were excised successfully with open surgery using a CO2 laser.
Footnotes
Acknowledgments
This study was supported by a grant from the Wooridul Spine Foundation.
Disclosure Statement
No competing financial interests exist.