
Abstract
Introduction
High intensity lasers have been proposed as an adjunct to conventional endodontic therapy, due to their capacity to reduce microorganisms present in root canals and increase dentinal permeability by not forming the smear layer. 4 –7 Dentinal permeability is directly related to the search for efficient cleaning and smear layer removal. The permeability of dentin allows intra-canal medication to diffuse across the tubules, improving the effectiveness of the treatment. 8,9
Initial studies have shown laser irradiation to cause major thermal side-effects, such as melting and cracking of dentinal tissues and pulpal damage. Recently, new equipment capable of removing dentin and enamel without causing thermal damage has been introduced. 10 –12 The Er:YAG and Er,Cr:YSGG lasers provide a wavelength that coincides with the maximum absorption wavelength of water and hydroxyapatite and due to these properties, the surrounding tissues are minimally affected.
The literature shows that smear layer removal after Er,Cr:YSGG laser irradiation is efficient without causing dental tissue carbonization or melting. 10,11 Moreover, the average temperature rise on root surfaces has been reported to be less than 8°C, and the Er,Cr:YSGG laser has been shown to be effective for soft-tissue surgery as well as for cutting enamel, dentin, and bone. 11,13 –15
The Er,Cr:YSGG laser uses a pulsed-beam system, fiber delivery, and a sapphire tip bathed in a mixture of air and water spray. When dental hard tissue is irradiated by the Er,Cr:YSGG laser with water spray, not only is the temperature suppressed, but also cutting efficiency is increased. 14 Morphologically, scanning electron microscopy studies indicate that after Er,Cr:YSGG laser irradiation, the appearance of dentin cavities is described as a molten lava-like appearance with an irregular structure and many microholes. 14
Although many characteristics of laser irradiation are well-known, few studies in the literature report the use of Er,Cr:YSGG laser in endodontic treatment. Thus, the aim of this study was to evaluate the permeability of root canal walls with respect to intracanal medication penetration into the cervical, middle, and apical thirds, after conventional instrumentation and Er,Cr:YSGG laser irradiation with different settings.
Materials and Methods
Tooth selection
Fifty-two extracted human single-rooted teeth were used after obtaining the approval of the Research Ethics Committee of the local institution (protocol 88/05). Initially, the teeth were stored in 1% thymol solution to prevent dehydration.
Sample preparation
Crowns were sectioned at the enamel-cementum limit with double-face diamond discs (KG Sorensen, Barueri, Brazil). Radiographs were taken to confirm the absence of abnormal root canal anatomy and a #10 K-file was inserted into the root canal so that a working length of 1 mm of the apical foramen could be established. Canal orifices were flared with #1 and #2 Gates-Glidden drills (Maillefer Dentsply, Petrópolis, RJ, Brazil) and the debris were removed with a Hedströen file. A 0.5% NaOCl solution applied with a hypodermic syringe was used to irrigate the root canal up to the working length. Chemical-surgical preparation was performed with type-K (Dentsply/Maillefer, Tulsa, OK) files up to #60 (diameter of 0.6 mm) to allow the entry of the laser fiber up to the apical area. Irrigation with 0.5% NaOCl was used. Final irrigation was then carried out with 15 ml of 17% EDTA-T solution (Fórmula e Ação, São Paulo, SP, Brazil) and all samples were kept at 37°C to avoid dehydration and contamination.
Laser irradiation
After sample preparation, teeth were randomly assigned to four groups (n = 13). Group 1 (G1) served as a control and was not irradiated. Groups 2, 3, and 4 (G2, G3, and G4) were irradiated with Er,Cr:YSGG laser (Biolase Technologies, San Clemente, CA, USA), at a wavelength of 2.78 μm, 20 Hz repetition rate and 140 μs pulse duration. Laser parameters were set at: 0.75 W (G2), 1.5 W (G3), and 2.5 W (G4). During irradiation, samples were kept constantly cooled with water spray (24%) and air (34%). The delivery system was a flexible fiber with a tip of 400 μm (Z4). Irradiation was delivered by introducing the tip along the entire length of the root canal, irradiating the dentin wall from the apical to cervical region, with helicoidal movements at 2 mm of root surface per second, according to the technique previously described by Gutknecht et al. 16 in 1996. This procedure was repeated four times and the samples were kept at room temperature for 20 seconds between each irradiation. All irradiations were performed after measuring the output power of the laser equipment (Power/Energy Meter, model 841-PE, Newport, Irvine, CA) to ensure stable and standardized power outputs.
Dentin permeability assessment
Next, the apical foramen was sealed with wax, and the roots were externally sealed with ethyl cyanoacrylate.
The dye solution used to test dentin permeability was Rhodamine B, dissolved in a solution of the intracanal medication NDP (dexamethasone phosphate, paramonochlorophenol, and polyethyleneglycol; Fórmula e Ação Pharmacy, São Paulo, SP, Brazil) at a concentration of approximately 20%. 17 The root canals were filled with the dye combined with NDP solution up to 1 mm from the apical foramen with a hypodermic syringe. After 20 seconds, the solution was removed by means of suction cannulae and absorbent paper. After the dye penetration test, the specimens were left in a humidifier at 37°C.
Sample analysis
Using a low-speed sectioning machine (Labcut 1010, Extec, Enfield, CT), seven 2 mm thick transversal cuts were made in each specimen, which resulted in eight slices per sample (Fig. 1). The first two slices, corresponding to the cervical and apical thirds, were disregarded. The others, two from the cervical third (C1 and C2), two from the middle third (C3 and C4), and two from the apical third (C5 and C6), were used for the study.

Images of the six slices obtained after transversal cuts and dye solution penetration for G4 (irradiation with Er,Cr:YSGG laser, 2.5W). The first two slices correspond to the cervical third (C1 and C2), the next two correspond to the middle third (C3 and C4), and the last two correspond to the apical third (C5 and C6).
The images were digitalized using ImageLab 2.3 software (Softium Informática Ltda., São Paulo, SP, Brazil) to assess the dye-NDP solution penetration by measuring the dyed area. The percentage of the dyed area in relation to the total root canal area was calculated for each cut. After that, the average was calculated for C1, C2, C3, C4, C5, and C6 values.
Scanning electron microscopy
Four samples were prepared for scanning electron microscopy (SEM) analysis. They were fixed in 2% glutaraldehyde for two hours, and underwent three washes of five minutes each using a 0.1 M sodium phosphate buffer solution. They were dehydrated with a graded series of ethanol: 30%, 50%, 70%, and 90%, and finally with absolute ethanol. Samples were then gold sputtered and mounted on metal stubs. Data obtained were then submitted to statistical analysis. The Kruskal-Wallis test was used to determine if there were differences among the groups. The Student-Newman-Keuls test was used to determine the statistical differences and results of dentinal permeability according to each third.
Results
The results are presented in Table 1. It can be observed that the samples from the control group presented less infiltration when compared with the samples of the groups that received laser irradiation. Comparisons were made between the three different regions, apical, medium, and cervical. It can be observed that for all regions, G4 presented the highest infiltration values, differing from the other irradiated groups and the control group.
Vertically superscripted letters indicate statistically equal means.
In the apical third, G1 and G2 presented no statistically significant differences; however, G4 differed significantly from the other groups. In the middle region, G3 and G4 presented more infiltration than G1 and G2. In the cervical region, G4 also demonstrated more infiltration than G1, G2, and G3.
For all regions, G2 presented no statistical differences from the control group, meaning that for all thirds, irradiation with 0.75 W was statistically similar to the non-irradiated samples represented by G1.
Scanning electron microscopy analysis
Two micrographs were taken for each third (apical, middle, and cervical) of the specimens for all groups. G1 (Control) presented dentinal tubules covered by a smear layer that was formed during the procedure. Fig. 2 illustrates the SEM analysis of the control group in all thirds.
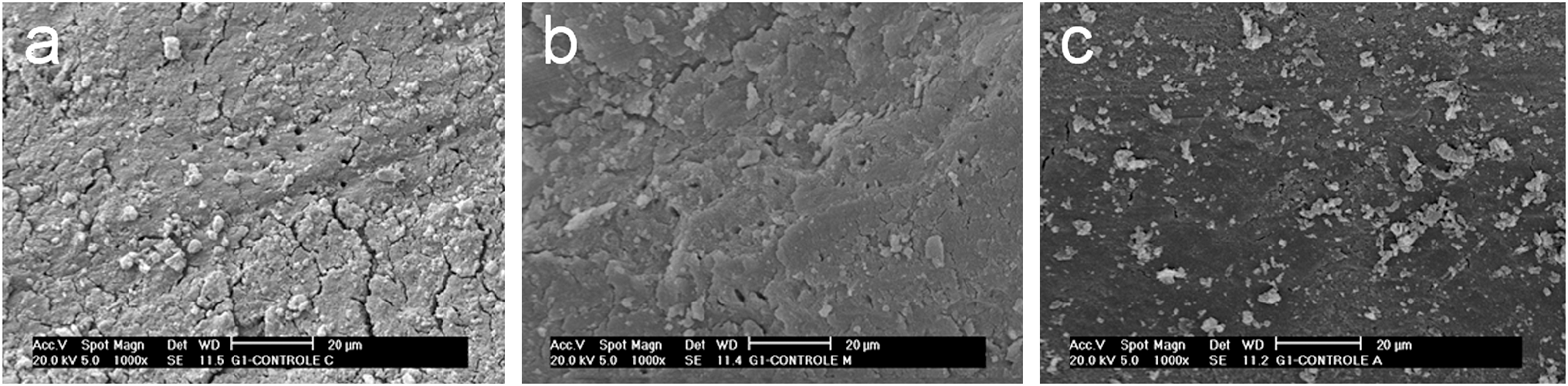
Scanning electron microscopy analysis of the control group in all thirds (
G2 (0.75 W) did not show any morphologic difference from the control group. This result is in accordance with the statistical analysis for dentinal permeability (Fig. 3).

Scanning electron microscopy analysis of samples irradiated with Er,Cr:YSGG laser, 0.75W, in all thirds (
In G3 (1.75 W) and G4 (2.5 W), root canal surfaces were free of a smear layer, with evidently open dentinal tubules and no signs of melting and carbonization (Figs. 4 and 5). However, some areas also showed inefficient cleanliness, presenting occlusion of dentinal tubules by a smear layer due to irregular laser irradiation.
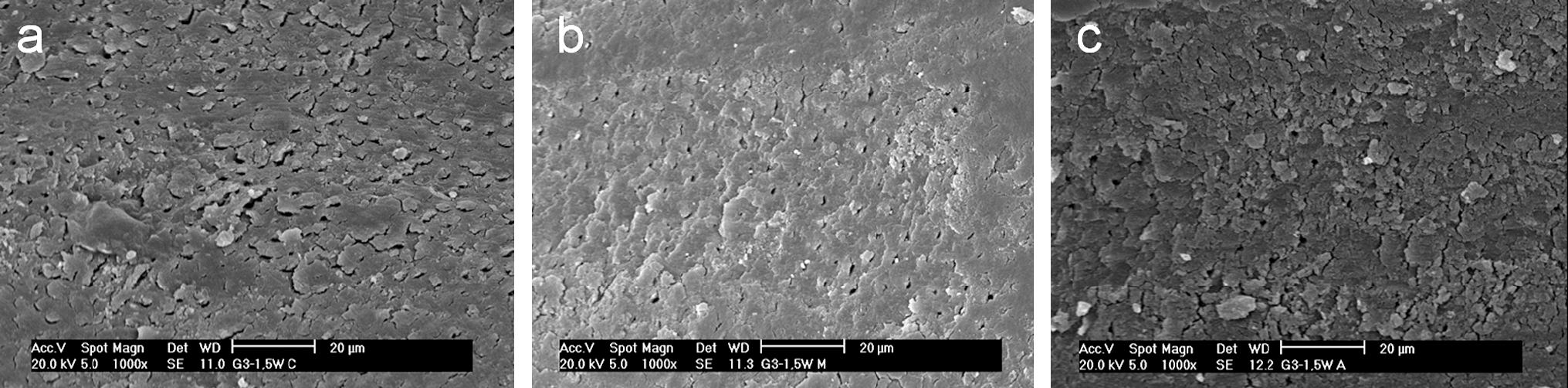
Scanning electron microscopy analysis of samples irradiated with Er,Cr:YSGG laser, 1.5W, in all thirds (
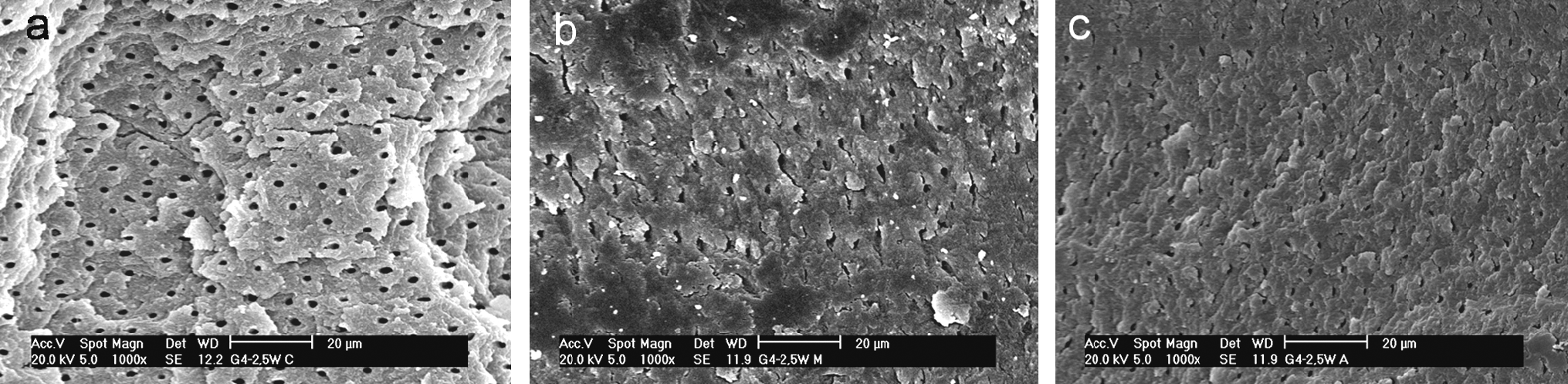
Scanning electron microscopy analysis of samples irradiated with Er,Cr:YSGG laser, 2.5W, in all thirds (
Discussion
The main goal of endodontic therapy is the removal of all organic material from the root canal. It has been demonstrated that mechanical instrumentation creates a smear layer of calcified detritus that adheres to the dentinal surface. In order to decrease the amount of smear layer on dentin root canal surfaces, rinses and antiseptic agents are used, enhancing the effect of hand instrumentation and improving the efficacy of the sodium hypochlorite. However, studies have shown that a combination of NaOCl and EDTA remove the smear layer only partially. 2,18 –20
The use of lasers in the field of endodontics is an innovative approach to disinfecting the root canal, opening dentinal tubules, and increasing dentin permeability. Increased dentin permeability can lead to the beneficial spreading of intracanal medications such as NDP, essential for the maintenance of a microorganism-free environment for the root canal during endodontic treatment. In general, dental lasers provide access to formerly unreachable parts of the tubular network due to their more efficient penetration into dental tissues, compared with rinsing solutions. 4,21
This study aimed to evaluate the dentin permeability and morphology of root canal walls irradiated with Er,Cr:YSGG laser with three different power settings, after conventional endodontic instrumentation. The determination of a protocol is essential for achieving satisfactory results when considering laser therapy. In endodontics, the search for a specific wavelength and dose is crucial for the safety of the procedure.
In the present study, the increase in dentin permeability observed in G3 (1.5W) and G4 (2.5W) is in agreement with the literature, and it is an accepted hypothesis that the Er,Cr:YSGG laser can cause ablation of the mineralized tissue and produce dentinal tubule exposure and smear layer removal. 14,22 Irradiation with Er,Cr:YSGG laser in root canal walls can be effectively used to remove pulpal debris left in root canals and to increase dentin permeability. This use is supplementary to manual instrumentation and considered to be helpful in cases where intracanal medications are used. 23
Morphological findings from other studies have indicated that after irradiation without water spray, carbonization is recognized in enamel and dentin, associated with an irregular structure with many microholes. 4,11,22 Irradiation with water spray, however, should cause a temperature rise of less than 8°C, and is effective in smear layer and debris removal from root canal walls. 10 During laser irradiation, the use of water spray directed at the ablation site increased the ablation depths, so water can play an important role in initiating ablation in dental hard tissues. 11,13,14
It should be emphasized that in addition to applications related to the intracanal medication phase, the bactericidal effect of high intensity lasers is also interesting for endodontic treatment and should be mentioned and considered. 10,24
In the present study, despite the satisfactory results for dentin permeability, micrographs showed that irradiation was irregular for all settings, in agreement with other descriptions in the literature. 25 The irradiation technique used appears not to distribute the radiation homogeneously. The fiber optic used in the helicoidal technique promotes irregular irradiation. However, a novel radial-firing tip for the Er,Cr:YSGG laser equipment has been designed to allow more homogeneous laser irradiation of root canal walls, and preliminary results have shown that the Er,Cr:YSGG laser in conjunction with this radial-firing tip is a suitable tool for the elimination of bacteria in root canals and for the removal of smear layers. 26 The same authors discuss the analysis of temperature, and mention that the procedure should be performed such that the thermal impact of Er,Cr:YSGG laser irradiation is ensured. The results of Yamazaki et al. 11 (2001) indicated that Er,Cr:YSGG laser irradiation with water spray cooling is a useful method for removal of the smear layer and debris from root canals. Also, Ishizaki et al. 10 (2004) suggested that rises in temperature during Er,Cr:YSGG laser irradiation caused minimal damage to periodontal and bone tissues. Moreover, they suggested that the procedure can efficiently remove the smear layer and debris without causing any carbonization or melting.
The results of the present study suggest that, within the limitations of an in vitro study, the Er,Cr:YSGG laser is useful for removing the smear layer from root canals and increasing dentin permeability, and can be recommended for clinical use.
Conclusion
Although Er,Cr:YSGG laser irradiation was not homogenous along the root canal length, the power settings of 1.5 W and 2.5 W provided morphologic changes favorable for increasing dentin permeability, with superior statistical results when compared with the control group.
Footnotes
Acknowledgments
The authors would like to express their gratitude to the Special Laboratory of Lasers in Dentistry (LELO) at the University of São Paulo (Brazil) and to thank State of São Paulo Research Foundation (FAPESP) for financial support (grants CEPID/CEPOF 98/14270-8 and 05/53737-4).
Disclosure Statement
No competing financial interests exist.