
Abstract
Introduction
LLLT is a form of phototherapy that involves the application of low power light in the red or near-infrared wavelengths to mitigate and treat various diseases such as arthritis. 2,6 LLLT is used to increase the speed, quality, and tensile strength of tissue repair, resolve inflammation, reduce edema, and give pain relief. 2 Lasers and noncoherent light sources such as light-emitting diodes (LEDs) can be used for the stimulation of cell function. Visible or near-infrared photons are thought to be absorbed by chromophors within the cells, such as cytochrome c oxidase located in the mitochondria. 7 Alterations in the activity of cytochrome c oxidase results in increased production of adenosine triphosphate, a major source of cellular energy, which leads to normalization of cell function, pain relief, and healing. 8 Many reports have sought to identify the optimal optical parameters for wavelength, total fluence, irradiance (also known as fluence rate or power density), polarization state, coherence, and pulse structure for various experimental and therapeutic outcomes; however, there is little consensus on this complicated matter. There have also been many studies reporting negative results. 2
In the present work, a comprehensive analysis of the effect of LLLT and LED on the outcome of zymosan-induced arthritis in rats was performed, with a special focus on vascular permeability (VP), edema, and articular incapacitation (AI). In addition, we compared two GaAs laser wavelengths and LED to identify which is the best for arthritis treatment.
Materials and Methods
Laboratory animals
The experimental protocol was approved by our local ethics committee (protocol number A027/CEP/2006), which follows the guidelines of the Brazilian College of Animal Experimentation. Male Wistar rats weighting 250–280 g were housed in individual cages with free access to a standard laboratory diet and drinking water. Animals were kept in a 12:12 h light/dark cycle (lights on from 6:00 AM to 6:00 PM) in a temperature-controlled room (26°C). All experiments were designed to minimize animal suffering. Animals were randomly distributed into five groups with n = 18 for each experimental group. This sample size was determined by balancing the requirement of Animal Care National Regulations to use the minimum number of animals with the ability to obtain data whose SEM values averaged <10%.
Zymosan-induced arthritis
Rats received an intra-articular injection of 1 mg zymosan (Sigma Chemical Company, St. Louis, MO, USA ), dissolved in 50 μL of a sterile saline solution, into one rear knee (stifle) joint. The procedure was done under general anesthesia, using a mix of ketamine 80 mg/kg (Hospira, Inc., Lake Forest, IL, USA) and xylazine 20 mg/kg (Lloyd, Inc., Shenandoah, IA, USA) intramuscularly.
Light sources, doses, and treatment
A low-level semiconductor GaAs laser, Theralase D.M.C. (São Carlos, SP, Brazil), operating continuous wave either in 685 nm or 830 nm wavelengths was used through the whole experiment to irradiate the animals. The laser parameters for both wavelengths were 20 mW of power, 100 sec irradiation time, and 0.8 cm2 irradiated area, which corresponded to a laser dose of 2.5 J/cm2. The optical power of the laser was calibrated using a Newport multifunction optical meter (model 1835C, Newport Corp., Irvine, CA). That laser dose, low enough to avoid any thermal effect, was chosen on the basis of studies reported in the literature that had shown a beneficial effect of the low-level laser on the inflammatory process. 5,9
A 628 nm LED device (Model Super Red LED-RL5-R3545; Super Bright LEDs, Inc., St. Louis, MO, USA) was employed to irradiate animals. The LED parameters were 20 mW of power, 100 sec irradiation time, and 0.8 cm2 irradiated area, which corresponded to an irradiation dose of 2.5 J/cm2. The spectral bandwidth of the LED emission peak was 30 nm. For the sake of comparison, the same area size on the knee and dose were used for both laser and LED irradiation sources.
All of the rats received a zymosan injection to induce arthritis and were then distributed into five groups containing 18 animals each. The first group received no treatment at all. The second and third groups were irradiated using a laser at 685 nm and 830 nm, respectively, and the fourth group was irradiated with the LED. The fifth group received 4 mg/kg of dexamethasone dissolved in sterile saline intraperitoneally 1 h before the zymosan injection as an anti-inflammatory positive control (Sigma Chemical Company). Treated animals were irradiated 0, 1, and 2 h after induction of inflammation. 10
Each one of the five groups was divided into three subgroups of six animals each in order to perform the following tests: (1) evaluation of VP, (2) analysis of articular edema, and (3) evaluation of AI, respectively.
Evaluation of VP
Alterations in VP were evaluated by assessing the extravasation of Evans Blue dye (EB) into rat knee joint, 3 h after injection of zymosan. EB (20 mg/kg, intravenous) was injected 20 min before animals were sacrificed. After being euthanized, they were exsanguinated for assessment of extravasation. The knee joint cavity of each animal was washed with 200 μL of phosphate-buffered saline (pH 7.4) and centrifuged at 2000 g for 5 min. The concentration of EB in the supernatant was determined by recording the absorbance at 620 nm and comparing it to a standard curve of EB. 11 Results were expressed as micrograms of EB per milliliter.
Analysis of articular edema
For evaluation of edema, animals were killed and exsanguinated 3 h after induction of arthritis, by which time edema had reached its maximum as described by Rocha et al. 4 Next, the synovia was surgically removal and the wet weight (g) was recorded. This material was dried overnight at 80°C and the dry weight (g) was also recorded. The difference between the wet and dry weights was used to evaluate the synovial edema.
Evaluation of AI
In order to analyze the antinoceptive effect of laser, LED, and the anti-inflammatory dexamethasone in animals with experimental arthritis, we used the rat knee joint incapacitation test. 12 Briefly, after zymosan injection animals were set to walk over a steel rotary drum (30 cm wide × 50 cm diameter), covered with a fine-mesh nonoxidizable wire screen, which rotates at 3 RPM. Specially designed metal gaiters were wrapped around both hind paws. After fitting the gaiters into the animals they were allowed to walk freely over the drum for habituation. An electronic circuit was constructed to send a signal to a computer each time that the right rat paw was not in contact with the drum, whereas the gait on the left paw was used to maintain the animal equilibrium. The paw elevation time (PET) is the time during which, for a 60 sec period, the inflamed hind paw is not in contact with the cylinder. This is defined as the AI. The PET was determined hourly up to 5 h after zymosan injection, at which time the animals were sacrificed. Results are expressed as sec/1 min; i.e., in sec per 1 min test. The maximum PET occurred between 3 and 4 h after zymosan injection.
Statistical analysis
Results are expressed as mean ± SEM. Differences among groups were analyzed by one-way analysis of variance (ANOVA) followed by Tukey test. Values of probability lower than 5% (p < 0.05) were considered significant.
Results
Effect of LLLT, LED, and dexamethasone administration on VP
Injection of zymosan into the rat knee joint provoked an increase of VP, which occurred a maximum at 3 h after drug injection. Figure 1 displays the EB extravasation into the knee joint for untreated and treated groups 3 h after injection of zymosan. Treatment with GaAs laser at 685 nm and 830 nm significantly reduced (p < 0.05) the increase in VP compared to zymosan (untreated) group, while the group treated with LED had no significant effect in VP formation caused by zymosan. It was also observed that the administration of dexamethasone also significantly reduced the VP. A significant difference was not seen between treatment with red or infrared laser irradiation. Also, no significant difference was observed between the group treated with dexamethasone and those treated with laser and LED. The reduction of the VP increase for different treatments was 22.7% with 685 nm wavelength laser, 25.0% with 830 nm wavelength laser, 20.4% with 628 nm LED, and 29.5% with dexamethasone. A comparison of the different treatments showed that dexamethasone was more effective for reducing the VP than 685 nm laser, 830 nm laser, and 628 nm LED by 8.8%, 6.0% and 11.4%, respectively.
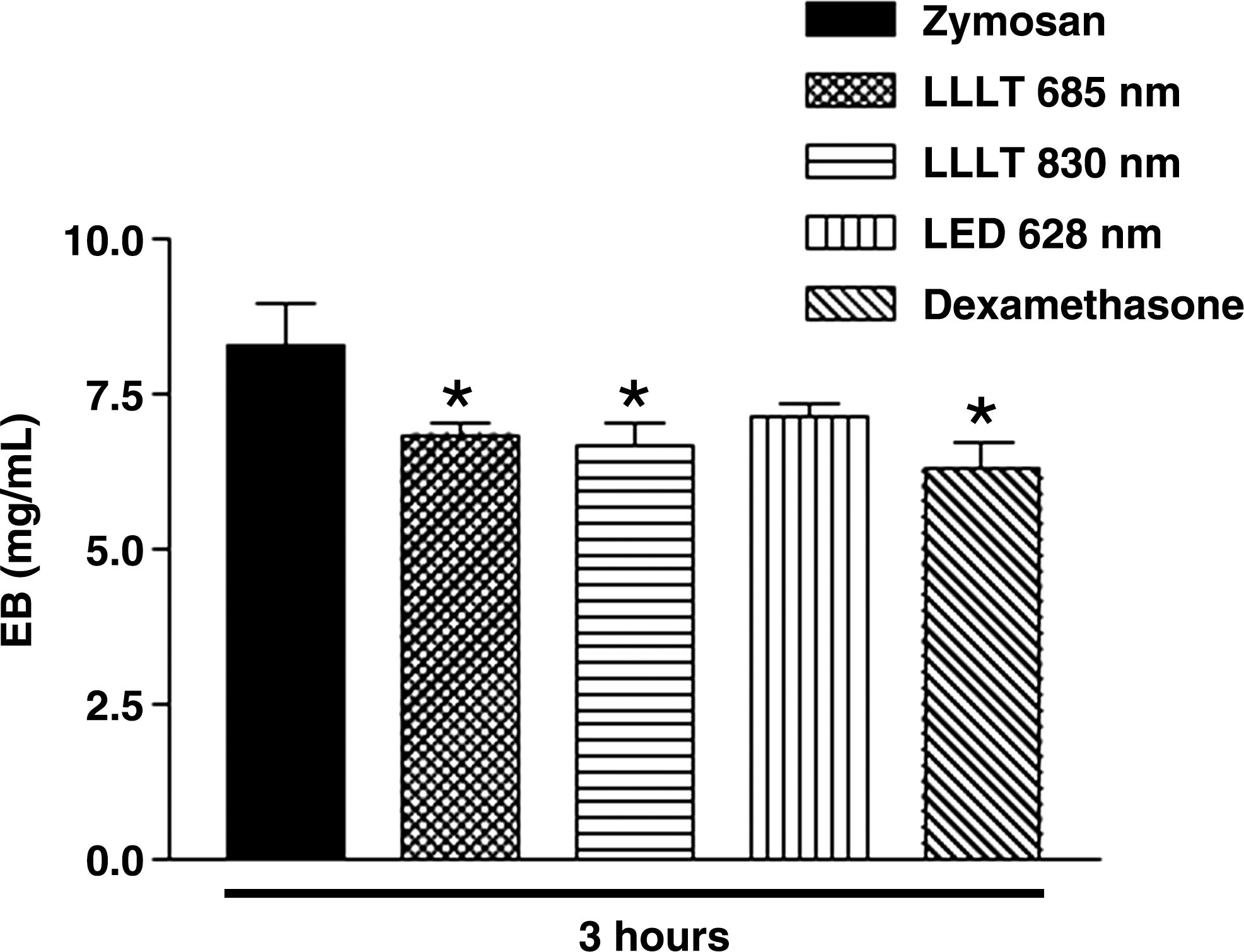
Effect of laser at 685 nm and 830 nm wavelengths, light-emitting diode (LED), and dexamethasone in reducing the vascular permeability induced by zymosan. Dexamethasone was used as an anti-inflammatory standard. Increase in vascular permeability was assessed 3 h after injection of zymosan. Data represent the mean ± SEM of six animals per group. *p < 0.05 compared to zymosan group without treatment.
Effect of LLLT, LED, and dexamethasone administration on edema formation
Red and infrared laser irradiation in wavelengths of 685 nm and 830 nm, respectively, caused a significant (p < 0.05) reduction in edema formation when compared to the untreated zymosan group (Fig. 2); however, no difference was found between the action of the two lasers. On the other hand, the group treated with LED had no significant reduction in edema formation (p > 0.05). A significant difference (p < 0.05) was obtained between treatment with dexamethasone, as compared to 685 nm laser, 830 nm laser, and LED. The percentage of edema reduction for the different treatments was 24.0% with the 685 nm laser, 22.2% with the 830 nm laser, 4.1% with the 628 nm LED, and 50.2% with dexamethasone. The anti-inflammatory drug was more effective in reducing edema than phototherapy by 34.5%, 36.0%, and 48.0% for 685 nm laser, 830 nm laser, and LED, respectively.
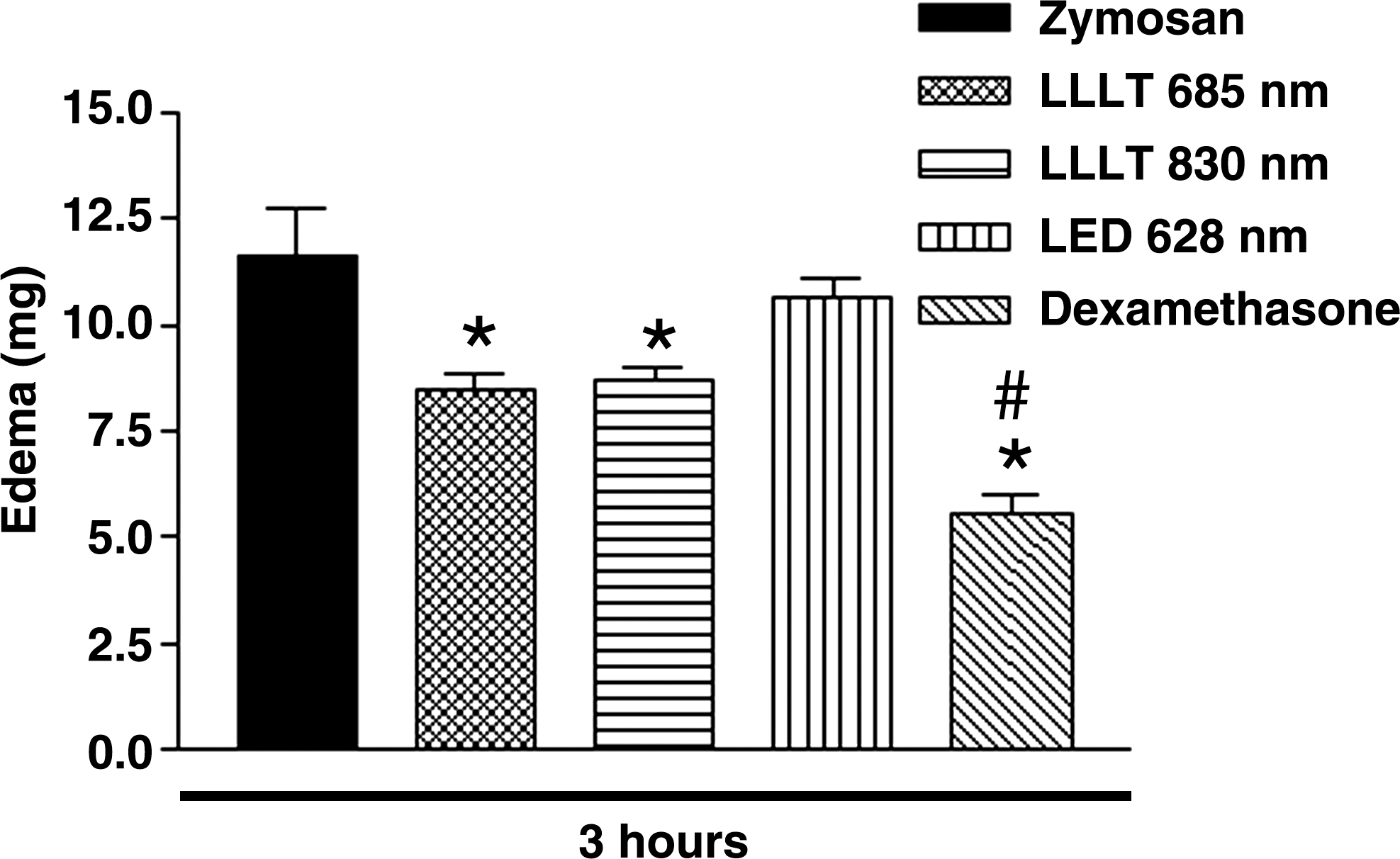
Effect of laser at 685 nm and 830 nm wavelengths, LED, and dexamethasone in reducing the edema induced by zymosan. Dexamethasone was used as an anti-inflammatory standard. Data represent the mean ± SEM of six animals per group. *p < 0.05 compared to zymosan group without treatment. # p < 0.05 compared to lasers and LED.
Effect of LLLT, LED, and dexamethasone administration on AI
Data on AI, evaluated 4 h after zymosan injection, are shown in Fig. 3. The two groups irradiated with laser in 685 nm and 830 nm wavelengths, respectively, as well as the one treated with dexamethasone had significantly reduced AI (p < 0.05), whereas no effect was seen on AI with LED irradiation. No significant difference was found between the dexamethasone and the three phototherapy treatments. The reduction of AI for the different treatments was 58.9% with the 685 nm laser, 58.9% for the 830 nm laser, 40.6% with the 628 nm LED, and 78.0% with the dexamethasone. On the other hand, dexamethasone was more effective than 685 nm laser, 830 nm laser, and LED treatments by 46.5%, 46.5%, and 63.0%, respectively.
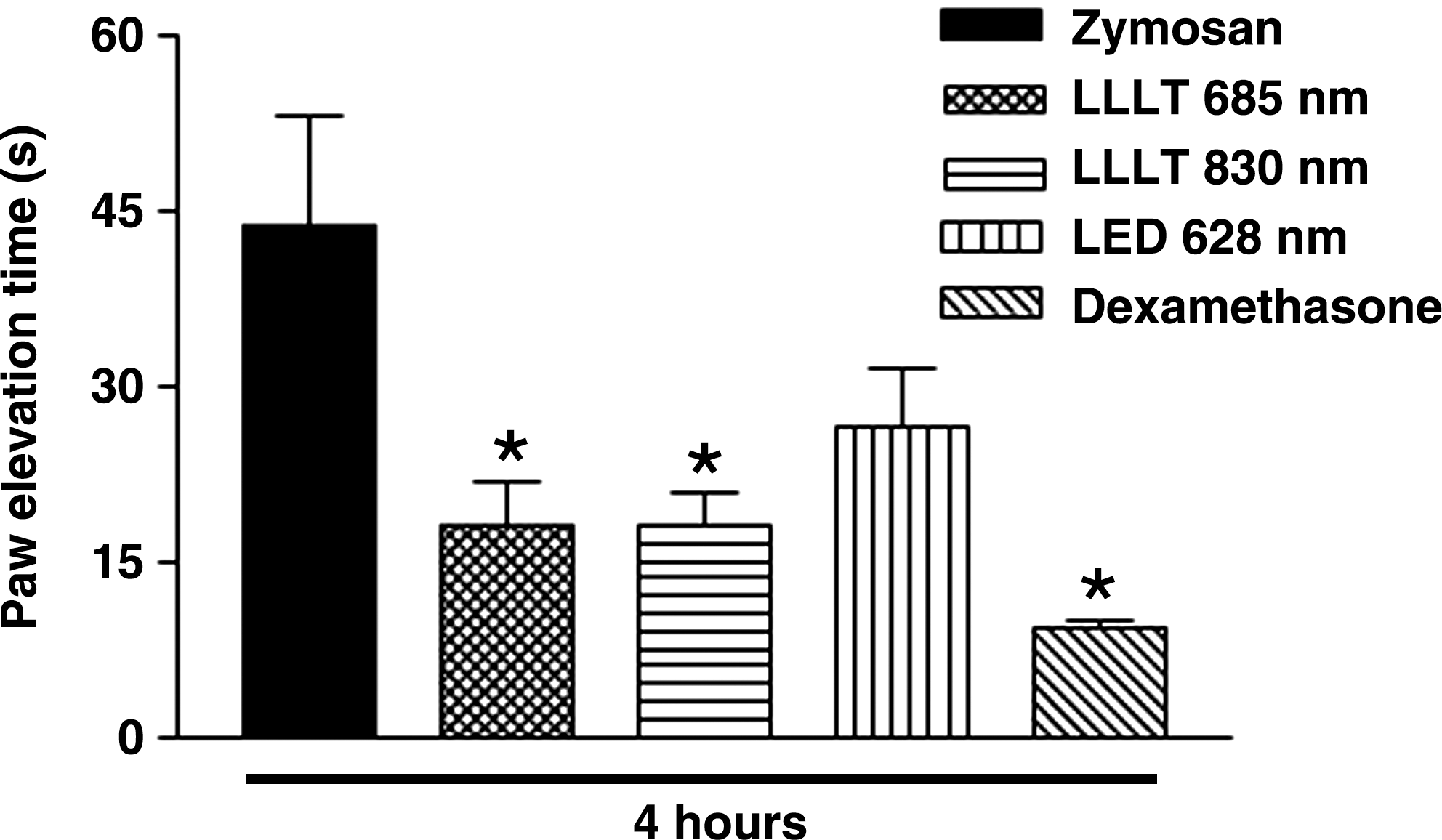
Effect of laser at 685 nm and 830 nm wavelengths, LED, and dexamethasone on the articular incapacitation in zymosan-induced arthritis. Dexamethasone was used as an anti-inflammatory standard. The paw elevation time (PET) was measured over a time period of 60 sec, 4 h after zymosan administration. Data represent mean ± SEM of six animals per group. *p < 0.05 compared to zymosan group without treatment.
Discussion
Arthritis, one of the most common joint diseases, is characterized by degraded articular cartilage and concomitant alteration of synovium and subchondral bone metabolism, leading to pain, joint edema, stiffness in joints, and impaired physical function. 13 Laser therapy was introduced as an alternative for noninvasive treatment for arthritis about 20 y ago, but its effectiveness is still controversial. 14 In this work, we investigated the use of low-level laser and LED therapies for the treatment of zymosan-induced arthritis in rats. A comparison between the effects of both treatments, for the same irradiation dose, was done.
Increased VP and edema are among the earliest events in the inflammatory response following by infiltration of leukocytes. These events are initiated and maintained by a sequence of inflammatory mediators of cellular and plasma origin. 14 In our study, zymosan caused an intense inflammatory reaction characterized by an increase of the VP, edema, and AI, 3 h after its administration. These results agree with findings by Rocha et al. 4 that show a maximum in VP and local edema 3 h after the arthritis induced by zymosan. In our experimental model, treatment with LLLT was effective in reducing the VP by 24%, edema formation by 23%, and AI by 59%, averaged over both laser wavelengths. The reduction of edemathogenic effect induced by carrageenan in rat paw tissue after LLLT has been reported by other authors. 10,15,16 On the other hand, treatment using LED radiation, for the same dose as the laser, had no effect in reducing VP, edema, and AI in zymosan-induced arthritis.
Reports in the literature seem to indicate that LLLT acts by reducing PGE2-levels and inhibiting cyclooxygenase-2 expression. 17,18 PGE2 is a potent mediator involved in inflammation and pain processes. It causes hyperalgesia and vasodilatation and, in combination with other agents, extravasation of fluids to adjacent tissues, which promotes edema formation. 19 The inhibition of PGE2 by LLLT could be, in our model, an important mechanism by which the laser reduces the increase in VP and edema formation associated with zymosan-induced arthritis, a hypothesis that needs to be addressed in future studies.
In our work, we employed the test for AI to study the hyperalgesia that occurs in zymosan-induced arthritis. AI is due to altered nociception occurring in articular structures. The inflammation caused by zymosan administration into joints, in addition to provoking edema and cell influx, also causes AI. 4 Using this experimental model, we observed significant functional improvement and inflammatory pain reduction after LLLT for both laser wavelengths. Nevertheless this was not observed for the group irradiated with the same dose of LED.
The exact mechanism of pain reduction by laser therapy is not completely understood. Some studies have suggested that laser irradiation could produce analgesia acting on K+ channels, 20 while another study showed that laser irradiation does not induce a photophysical effect but acts directly in the mitochondria without any effect on the cell mechanism. 21 Furthermore, Tascioglu et al. 1 have suggested that neuronal activity inhibition might be responsible for the therapeutic effect and the laser irradiation selectively inhibits nociceptive signals at peripheral nerves. 22 It was also suggested by Honmura et al. 17 that the anti-inflammatory effect of laser irradiation is due, at least partially, to certain mechanisms that do not involve the secretion of endogenous opioids. Additionally, Ferreira et al., 5 using a carrageenan model to induce hyperalgesia, demonstrated that the analgesic effect caused by laser does not involve a peripheral opioid receptor but rather later events of PGE2 release during the acute inflammation. PGE2 is a key mediator of inflammation and pain in arthritis. 23 It is possible that in our model the analgesic effect of both laser wavelengths was due to the inhibition of PGE2 release. An effective reduction in PGE2 concentration has been reported for active Achilles tendonitis in humans treated with laser in 904 nm. 25
Some laser parameters such as wavelength, duration of treatment, energy density, number of treatments, and mode of irradiation may be important for laser treatment of different pathologies. 26 It is rather difficult to determine the optimal dosage and treatment schedule for a laser therapy when the minimal effective dosage is in most cases unknown. A systematic study on the efficacy of physical interventions in osteoarthritis knee pain in humans was reported by Bjordal et al. 27
In our study, both 685 nm and 830 nm wavelengths of LLLT with an irradiation dose of 2.5 J/cm2 were effective in reducing the increase of VP, edema formation, and AI. No significant difference was observed between the effects of the two wavelengths. Although we did not find any statistically significant differences between the untreated and LED-treated groups, we cannot exclude the possibility that the LED therapy may be an effective treatment with other LED irradiation parameters.
The difference of efficacy between laser and LED irradiation for the same irradiation parameters may be due to LED emission having a larger spectral linewidth (30 nm) than the laser; because of that, energy from the LED could be less absorbed by the chromophors present in the biological tissue. Considering the results of this study, new inquiries may be carried out to evaluate the effectiveness of the LED irradiation for different wavelengths and higher doses, in order to assess the use of this type of low cost therapy in clinical applications.
In conclusion, the results of this study indicate that LLLT reduces inflammatory signs more effectively than LED irradiation with similar irradiation times (100 sec), average outputs (20 mW), and energy doses (2 J) in an animal model of zymosan-induced arthritis. The anti-inflammatory effects of LLLT appear to be a class effect that is not wavelength specific in the red and infrared parts of the optical spectrum. Data suggest that the LLLT in inflammatory arthropathies may be clinically relevant.
Footnotes
Acknowledgment
We thank MSc Leandro Procópio Alves for his laboratory assistance.
Author Disclosure Statement
The authors declare that no competing financial interests exist.