
Abstract
Introduction
In recent years, low-level laser therapy (LLLT) has gained considerable recognition and importance among treatment modalities for various medical problems including wound repair processes, musculoskeletal complications, and pain control. 9,10 The literature indicates that laser photobioactivation modulates the level of prostaglandin, enhances the action of macrophages, promotes fibroblast proliferation, facilitates collagen synthesis, fosters immunity, and even accelerates the healing process. 11 Previous studies have shown that such therapy may be of great benefit in the treatment of chronic wounds that occur as a complication of diabetes mellitus, 12 and other studies suggest that laser photostimulation has a beneficial effect on wound healing in diabetic mice. 13
Laser systems used for photostimulation and in soft-tissue surgical procedures are carbon dioxide lasers, neodymium-doped yttrium aluminium garnet (Nd:YAG) lasers, and diode lasers. Many studies comparing scalpel with laser in wound healing have been performed. 14 –16 With laser irradiation, the major advantages are the production of local hemostasis, creating a virtually bloodless surgical field, bacterial elimination, and contact-free incision. 17,18 After surgery, patients report less discomfort and fewer functional complications (speaking and chewing) and require fewer analgesics than do patients treated with conventional scalpel surgery. 19 Postoperative pain is also notably minimized with laser incisions. 20 Studies have described equivalent or better healing results with laser incisions than in scalpel wounds. 21,22 Although some studies have demonstrated that diode lasers have positive effects on wound healing, their effects on diabetic wound healing has not been studied adequately, especially with photostimulation. The aim of this study was to investigate effect of LLLT on healing of skin incisions made using a diode laser in diabetic rats.
Material and Methods
Eighteen Wistar rats weighting 250 to 300 g (Ataturk University Faculty of Veterinary Animal Care Unit) were initially used for this study. The rats were housed two animals per cage in a room with a 12-hour light/dark cycle. All animal care and surgery were conducted in accordance with an approved protocol reviewed by the Ataturk University Faculty of Veterinary Animal Care and Use Ethic Committee. Animals were given regular standard rat chow and water ad libitum throughout the experiment.
Diabetes was chemically induced using streptozotocin (STZ; Sigma, St. Louis, MO), 50 mg/kg, dissolved in citrate buffer (pH 4.5) and administered as a single intraperitoneal injection in all rats. Two days after STZ injection, blood glucose levels were measured using a glucometer and test strips (Optium Xceed Glucometer; Abbott), and all STZ-injected animals with a blood glucose of 250 mg/dL or more were included in the protocol.
Before surgery, the blood glucose level of each rat was checked again. Each rat was anesthetized with ketamine (10 mg/kg) and xylazine (3 mg/kg) intraperitoneally. The hair on the dorsum of all rats was shaved. The operative site was prepared aseptically. Three incisions (approximately 15 mm in length) were made on the dorsum of each rat. One incision was performed on the left side of the dorsum using a diode laser, and the other two incisions were performed using a steel scalpel (Rockwell number 15) and a diode laser on the right side of each rat. The tissues were incised without any elevation of a full-thickness flap. The incisions were then sutured with 3-0 polyglycolic acid. The incisions performed using a steel scalpel were used as a control group. The wound on the left side of each rat received laser stimulation. Rats were assigned to 3 experimental groups: Group 1: scalpel (n = 18); Group 2, diode (n = 18); Group 3, diode + biostimulation (n = 18).
The Doctor Smile erbium diode laser (Lambda Laser Products, Italy) was used to induce diode laser incision and LLLT. The laser used was a gallium-aluminum-arsenide (GaAlAs) laser, 808 nm wavelength (laser source power, 20W; laser Class IV; medical Class IIB; network frequency, 50 Hz; input power supply, 230 ± 10% V alternating current). The handpieces of the diode fiber (for cutting tissues) and biostimulation (for LLLT) are different that connecting to the main unit. The system of programs allows the user to choose from preset treatments, such as power level, type of pulse.
A continuous-mode diode laser was employed on the skin of rats at 4 W output power with a pencil-size handpiece containing 300-μm lasing fiber for cutting tissues. After procedures involving diode laser incisions, biostimulation spot was connected to the main laser unit for LLLT. LLLT was applied with a power density of 0.1 W/cm2. Laser irradiation was maintained within a 1-cm2 biostimulation spot. LLLT was started immediately after surgery and was repeated on days 2, 4, 6, and 8 (5 sessions) after surgery at 10 J/cm2 (total dose). Laser energy was applied 20 s (2 J/cm2) per session (total 100 seconds) and approximately 1 cm from the surface of the wound. Nine rats were killed to compare the degree of reepithelialization and inflammation at day 10. Nine other rats were killed to compare the degree of reepithelialization and inflammation at day 20.
Histopathologic Study
The specimens were embedded in paraffin and sectioned in a plane perpendicular to the incision. The specimens were stained with hematoxylin and eosin, examined at magnification of X40, and studied by two independent observers. Observers were blinded for the study of the specimens. To measure the degree of reepithelialization, the criteria established by Sinha and Gallagher 16 were used (0 =reepithelialization at the edge of the wound; 1 = reepithe-lialization covering less than half of the wound; 2 = reepithelialization covering more than half of the wound; 3 = reepithelialization covering the entire wound, irregular thickness; 4 = reepithelialization covering the entire wound, normal thickness). The degree of inflammation was measured using the resolution phases of inflammatory processes described by Cotran et al. 23 (1 = acute inflammation (with membrane formation), 2 = predominance of diffuse acute inflammation (predominance of granulation tissue), 3 = pre-dominance of chronic inflammation (fibroblasts beginning to proliferate), 4 = resolution and cicatrization (reduction or disappearance of chronic inflammation, although occasional round cells may persist)).
Data were analyzed using SPSS 11.0 for Windows (SPSS. Inc., Chicago, IL). Arithmetic means of data (two observers' data) were used for statistical analysis. The differences between groups were analyzed using the Kruskal-Wallis test. The Mann-Whitney U-test for pair-wise comparisons was performed when the Kruskal-Wallis test indicated significant differences.
Results
There was a significant difference between the three groups in reepithelialization at day 10 (p = 0.001) (Table 1). According to the Mann-Whitney U-test, there was a statistically difference between Groups 1 and 2 (p = 0.005) and between Groups 1 and 3 (p = 0.005). In Group 1, reepithelialization was at the edge of the wound (Fig. 1), but in Groups 2 and 3, reepithelialization was covering less than half of the wound (Fig. 2 and 3).
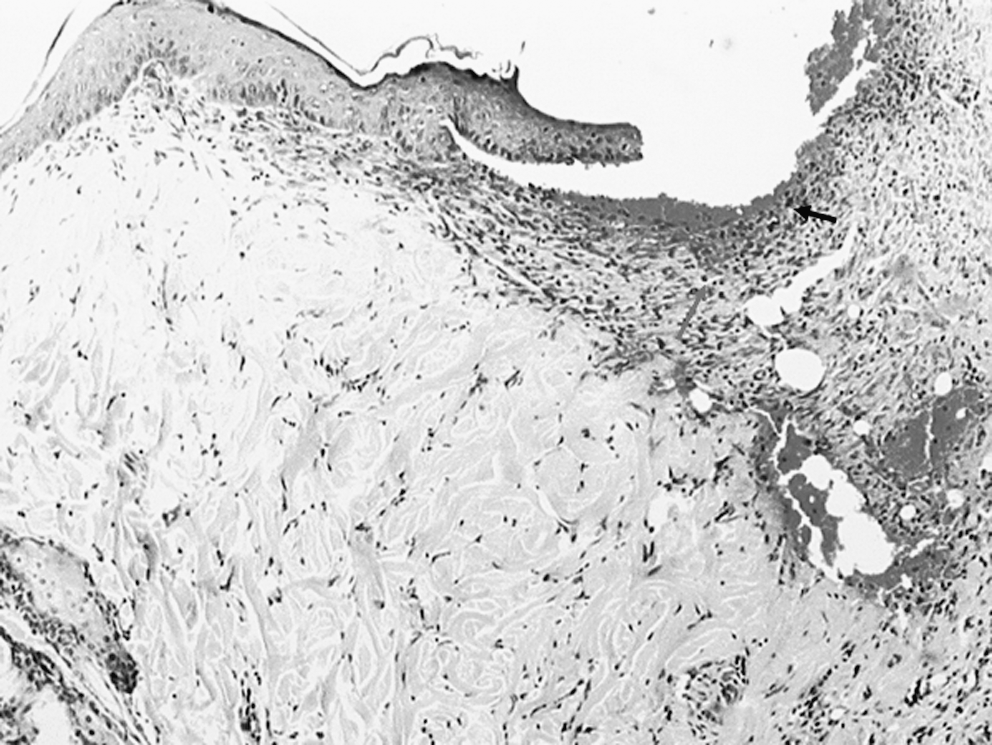
Photomicrograph of a tissue sample from an animal in the scalpel group 10 days after surgery. Reepithelialization (upper arrow) and inflammation (bottom arrow) can be seen (hematoxylin and eosin (H&E), original magnification X40).
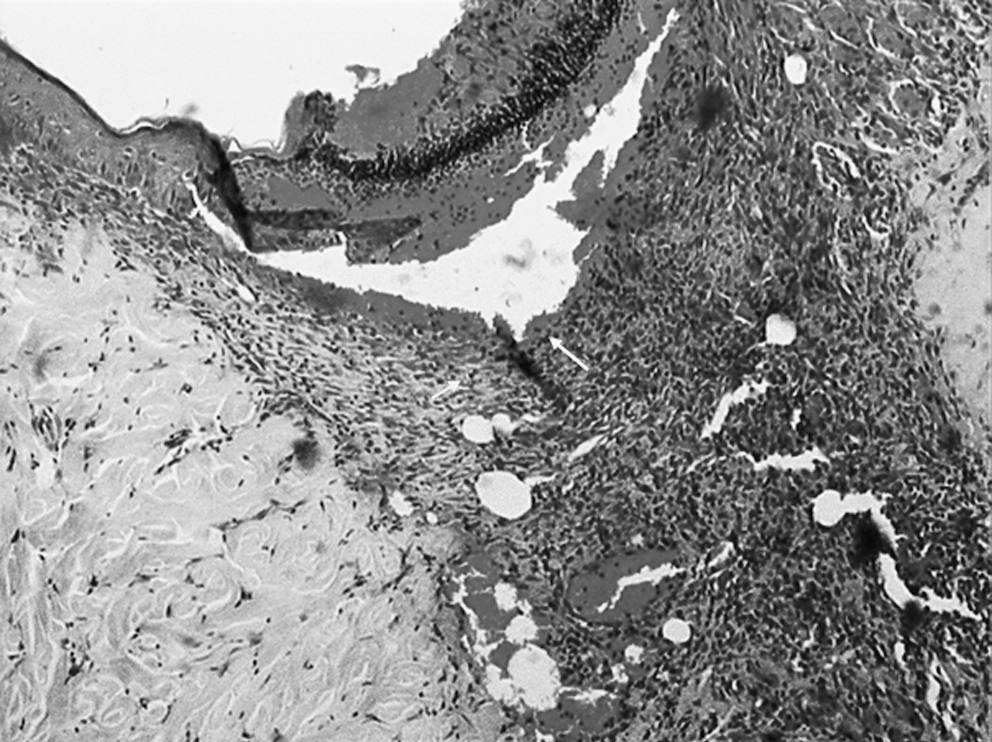
Photomicrograph of a tissue sample from an animal in the diode group 10 days after surgery. Reepithelialization (upper arrow) and inflammation (bottom arrow) can be seen (H&E, original magnification X40).
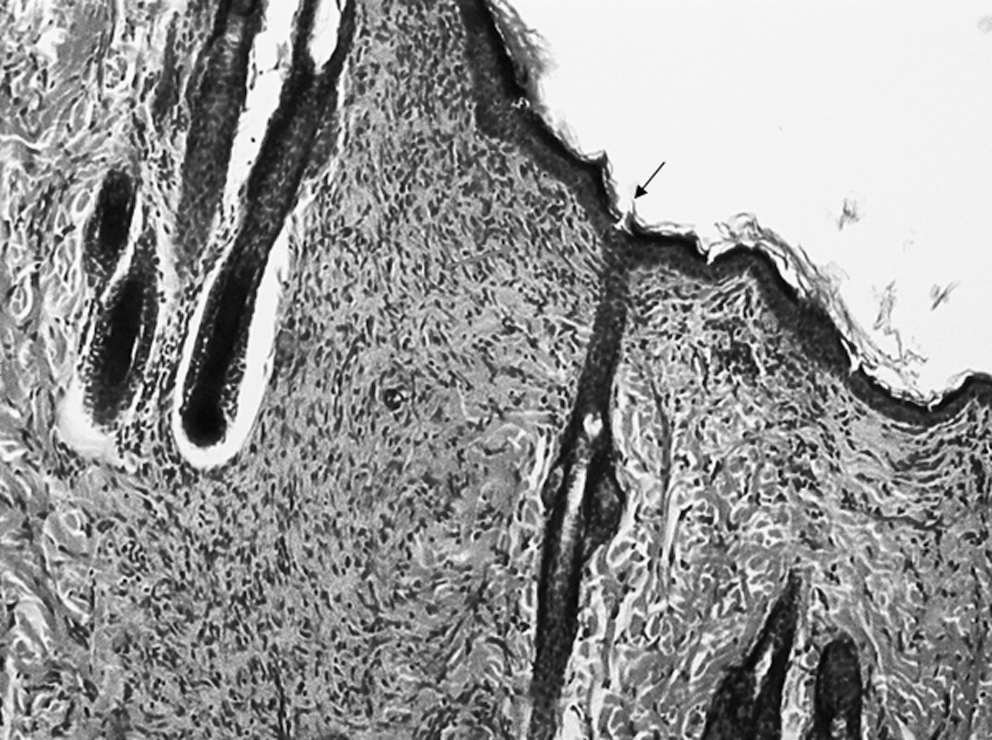
Photomicrograph of a tissue sample from an animal in the diode + biostimulation group 10 days after surgery. Reepithelialization (upper arrow) and inflammation (bottom arrow) can be seen (H&E, original magnification X40).
Statistically significant.
There was a significant difference between the groups in inflammation at day 10 (p = 0.04) (Kruskal-Wallis test) (Table 1). The post hoc Mann-Whitney U-test for pair-wise comparisons was performed when the Kruskal-Wallis test indicated significant differences and the Mann-Whitney U-test indicated a significant difference between Groups 1 and 3 (p = 0.03) and between Groups 2 and 3 in inflammation at day 10 (p = 0.04). By the end of 10 days, acute inflammation was observed in Groups 1 and 2 (Fig. 1). In Group 2, some histological results were characterized by fibroblasts with proliferative activity (Fig. 2). In Group 3, in most of the histological results, fibroblasts were beginning to proliferate (Fig. 3).
There was no statistically significant difference between the groups in inflammation and reepithelialization at day 20 (p > 0.05) (Table 2). In all groups, reepithelialization was covering the entire wound and the highest number of wounds of irregular thickness occurred at day 20. There were more normal-thickness wounds in Groups 2 and 3 than in Group 1. By the end of 20 days, a predominance of chronic inflammation (fibroblasts beginning to proliferate) was observed in all groups.
Discussion
The diode laser became commercially available and has been widely applied as an alternative to the scalpel. D'Arcangelo et al. 20 found that, although traditional surgical procedures allow an incision without loss of tissue, the laser surgical procedure guarantees good healing and has shown important clinical advantages, especially the excellent ability of incision and good bleeding control. Fukuda et al. 24 reported that the increase in the number of dividing cells and in the expression level of inducible nitric oxide synthase, keratinocyte growth factor, and keratinocyte growth factor receptor may facilitate earlier and thicker reepithelization in laser wounds than in electrocautery and scalpel wounds. In minor oral surgical procedures, diode laser therapy is less invasive and presents some indisputable advantages such as the elimination of bleeding and suturing and minimal postsurgical pain and edema. 20 Gulsoy et al. 25 found that a 980-nm diode laser system was a potential alternative tool to conventional suturing technique with its full-thickness skin-welding capability. Other studies have found that irradiation with a diode laser facilitates considerable bacterial elimination, which could positively influence the healing repair mechanism. 26 The literature documents many studies of diode laser advantages over the scalpel, but diode lasers use is not documented concerning the biostimulation application after diode laser surgery in diabetics. In our study, the energy of the diode laser used was in accordance with previous studies' average density in animals. 25,27 and it was determined that the diode laser stimulates wound healing in diabetics. Reepithelialization was faster in Group 2 (4-W output) than Group 1 at day 10 in diabetic rats. The effect of LLLT on diode laser incisions in diabetics was also evaluated in this study. LLLT advantages include acceleration of wound healing, enhanced remodeling and repair of bone, restoration of normal neural function, and modulation of the immune system. 28 –31 Many studies have focused on the effects of laser biostimulationon on wound healing. For wound healing, experimental protocols and parameters such as dose, waveform, treatment time, and treatment frequency of photostimulation are still controversal. In the present study, three wounds were made in the same individual animal. There is the possibility of systemic effects of laser treatment, which is not limited to the site of application by the liberation of biological mediators, but the results from pilot experiments have indicated that laser treatment had no systemic effects on contralateral wound healing. 32 Yu et al. 12 found that treatment with a 630-nm argon dye laser at a fluence (amount of energy passing through a unit area) of 5 J/cm2 enhanced the percentage of wound closure over time in genetically diabetic mice. Stadler et al. 33 examined the effect of daily irradiation with an 830-nm diode laser on the tensile strength of wounds. They discovered that, with a fluence of 5 J/cm2, wound strength was greater in genetically diabetic and nondiabetic mice. Kawalec et al. 13 discovered that treatment with the 980-nm GaAlAs diode laser at 5 W (18 J/cm2) had a beneficial effect on wound healing in diabetic mice. In the present study, the energy of LLLT employed was in accordance with the average fluence (10 J/cm2) used in these studies, and it was determined that there was a difference between the groups in reepithelialization and inflammation. Group 1 had lower degrees of reepithelialization than the other groups at day 10. The wounds of the groups incised with a diode laser cicatrized more rapidly than the group in which a scalpel alone was used. By the end of 10 days, acute inflammation was observed in Groups 1 and 2, whereas Group 3 was in a phase in which diffuse acute inflammation predominated (predominance of granulation tissue).
There was no statistically significant difference between the groups in inflammation and reepithelialization at day 20.
Scalpel incisions heal more slowly than diode and diode +biostimulation incisions in diabetic rats. Wound closure was significantly enhanced with a diode laser in diabetic rats, and we can suggest that diode laser + biostimulation may produce the least amount of tissue injury, with faster resolution of inflammatory response in diabetic rats. Diode laser incision (4 W) with 10 J/cm2 (808-nm wavelength) LLLT seems to have beneficial effects on skin incisions in diabetic rats.
Footnotes
Acknowledgments
This study was supported by Ataturk University Scientific Research Projects Fund.
The authors thank Dr. Havva Erdem and Dr. Cemal Gundogdu (Department of Pathology, Medical Faculty, Ataturk University, Erzurum, Turkey) for their evaluation of the histology slides.