
Abstract
Introduction
A number of attempts have been made to develop clinically new methods to enhance the process of the repair of damaged articular cartilage. The term low-level laser therapy (LLLT) is broadly applied to the therapeutic effects of laser. The clinical application of LLLT is growing rapidly, and several review articles on clinical applications of LLLT have been published. 2 LLLT with a He–Ne laser has been used in the treatment of musculoskeletal complications. 3 –8 In this regard, there were reports that LLLT with He–Ne laser can improve immobilized articular cartilage in vivo 3,6 and also that LLLT can increase the chondrocyte number in vitro. 7 Very recently, Peccin et al. 8 demonstrated that low-energy He–Ne laser is able to induce cartilage neoformation after 40 d following treatment. Since there have been no published reports on the effect of low-level He–Ne laser with a wavelength of 632.8 nm on repairing a 5 × 10 mm osteochondral defect in rabbits, the objective of the present study is to examine the potential therapeutic effect of LLLT with a He–Ne laser on the biomechanical parameters of repairing an osteochondral defect in rabbits.
Materials and Methods
Animal procedures
Forty-two adult white New Zealand rabbits aged 7 mo and weighing 3000 ± 300 g were used at the beginning of the experiment. All animals were fed a standard diet and given tap water ad libitum. The rabbits were divided equally into control and experimental groups. Each group was further divided into four subgroups: A, B, C, and D. Five rabbits from each group were selected randomly and sacrificed at 2 (A), 4 (B), and 8 wk (C) postoperative by inhalation of chloroform in a closed space, and six of the remaining rabbits from each group were sacrificed 16 wk (D) after surgery. All animal care, as well as experimental procedures, were conducted in accordance with the Medical Ethic Committee of Shaheed Beheshti University, M.C., code no. 3/5740. Surgery was performed on all rabbits under sterile conditions and after general anesthesia with ketamine hydrocholoride (50 mg/kg IM) along with diazepam (5 mg/kg IM). The right knee joint was approached through a medial parapatellar incision. The patella was dislocated laterally to expose the articular surface of the patellar groove. One circular defect 5 × 10 mm was drilled through the articular cartilage into the bleeding subchondral bone in the distal part of patellar groove with the use of a low-speed dental drill (Dental Fabriktreffurt, Delab, Germany). The joint capsule and skin were closed by 03 catgut and 04 nylon sutures, respectively. Antibiotic therapy with ceftrax (50 mg/kg IM, Jaber ben Hayyan, Tehran, Iran) was administered immediately before the operation and at 24 and 48 h after surgery. All animals were allowed to walk freely without any splint.
LLLT
Laser irradiation of the experimental rabbits was initiated following the creation of an osteochondral defect. Both femoral condyles of the right knee of the experimental rabbits received 148.4 J/cm2 He–Ne laser at 632.8 nm (IR 2000, Iranian Atomic Energy Agency, Bonab, Iran) applied transcutaneously by two shouts three times a week. The surface area of the laser beam was 0.0314 cm2, the laser shape was circular, and the duration of laser treatment for each shout was 466 s.
The rabbits were relaxed in a restrainer with an injection of one or two doses of anesthetizing drugs during laser irradiation. There were no methodological differences between the control and experimental groups, except for the use of LLLT. The rabbits in the control group received placebo LLLT with the laser equipment switched off. Due to the side effects of daily general anesthesia on rats, such as general body weakness and poor healing of wounds, which were observed in our pilot study, in the current study LLLT was performed three times a week. Bojard et al. 9 and Pinheiro et al. 10 have recommended daily laser treatment, with about 5 J/cm2 energy density for musculoskeletal disorders. In previous studies, we have demonstrated positive effects of He–Ne laser on immobilized articular cartilage with 5 J/cm2 energy density. 3,6 In these studies, 3,6 however, we did not consider the laser-beam surface area in order to calculate the energy density. In the present study, the laser delivery is the same as our previous studies 3,6 except this time we have calculated the energy density using the laser-beam surface area. 11 The energy density was therefore changed to 369.4 J/cm2.
Energy Density (J/cm2) = Power (W) × Time (s)/Area of irradiation (cm2). 11
Biomechanical test evaluation
At the end of the experimental periods, the rabbits were sacrificed by inhalation of chloroform in a closed space. The right femurs of the experimental and control groups were extracted by disarticulating the knee joint. The femurs were wrapped in gauze and soaked in physiologically balanced saline and frozen at −20°C for later biomechanical tests. 12 Before the biomechanical tests were conducted, the specimens were slowly thawed at room temperature and kept moist throughout the test. A flat nonporous indenter was attached to a mechanical testing machine (Model Z 2.5, Zwick GmbH & Co., Ulm-Einsingen, Germany). The indenter was lowered to make minimal contact with the cartilage of the patellar groove in order to zero the instrument display. Immediately, after 0.01 N preload, a stress-relaxation test was conducted by ramping up to 0.2 mm (50% of the cartilage thickness) and holding for 900 s to obtain an equilibrium state (the load did not change by more than 0.1% of the peak load). The deformation rate was set at 0.5 mm/min. The mechanical testing machine was connected to a computer for automated testing and data acquisition. The instantaneous stiffness (IS, N/mm) and maximum force (MF, MPa) were measured. The area under the curve (absorbed energy) was calculated in two parts: the first part of the energy absorption (FEA, MPa × s) was calculated up to the peak of the load-time curve; and the second part of the energy absorption (SEA) was calculated from the peak up to the equilibrium point. The equilibrium load (EL, MPa), FES, and SEL were determined using MATLAB software (Microsoft Corporation, version 7.02).
Statistical analysis
The normality of the data was analyzed using the Kolmogorov–Smironov test. An independent sample Student's t-test was conducted to determine differences between the control and experimental groups. Data within each group were subjected to one-way analysis of variance (ANOVA). Multiple comparisons were made by the least significant difference (LSD). The statistically significant difference was defined as a p value of less than 0.05. The data were expressed as mean ± SEM.
Results
General observations
Three rabbits died during the experiment for unknown reasons, and the knee of one rabbit became infected, so it was excluded from the study. Consequently, these rabbits were replaced with four new ones. The number of rabbits in each control and experimental subgroup was five, with the exception of the 16-wk study period (D) when there were six rabbits.
Results of statistical analysis between the control and experimental groups
The results of the statistical analysis between the control and experimental groups are illustrated in Figs. 1 –5. The mean of the biomechanical parameters of the experimental group was higher than for the control group in most cases. However, there was only one significant difference between the control and experimental groups: the SEA of the experimental group (56.11 ± 11.5) was significantly higher than that of the control group (18.9 ± 4) 4 wk after surgery (p = 0.015).
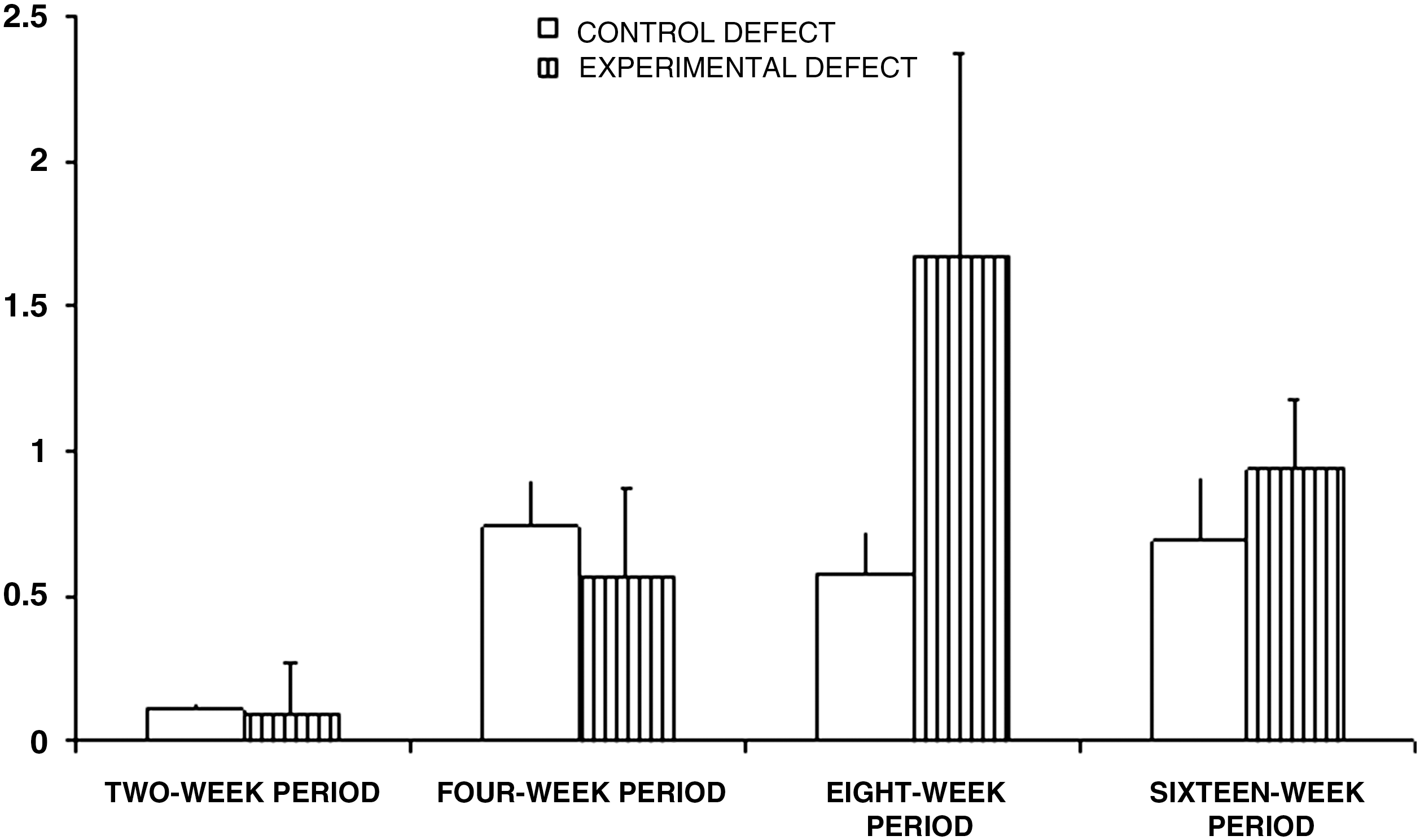
Mean ± SEM of the instantaneous stiffness (N/mm) of the studied groups. There were no significant differences between the studied groups.
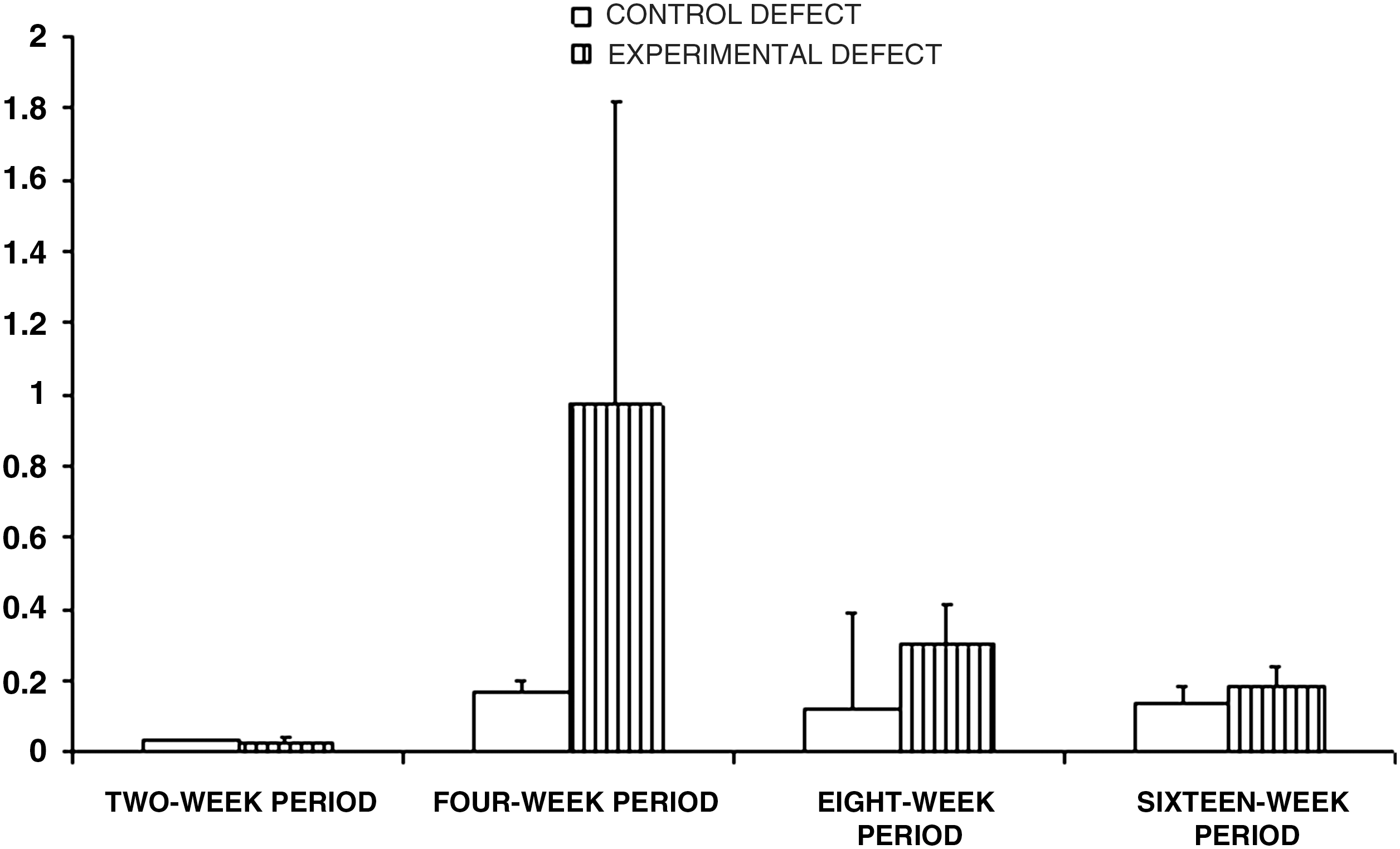
Mean ± SEM maximum force (MPa) of the studied groups. There were no significant differences between the studied groups.
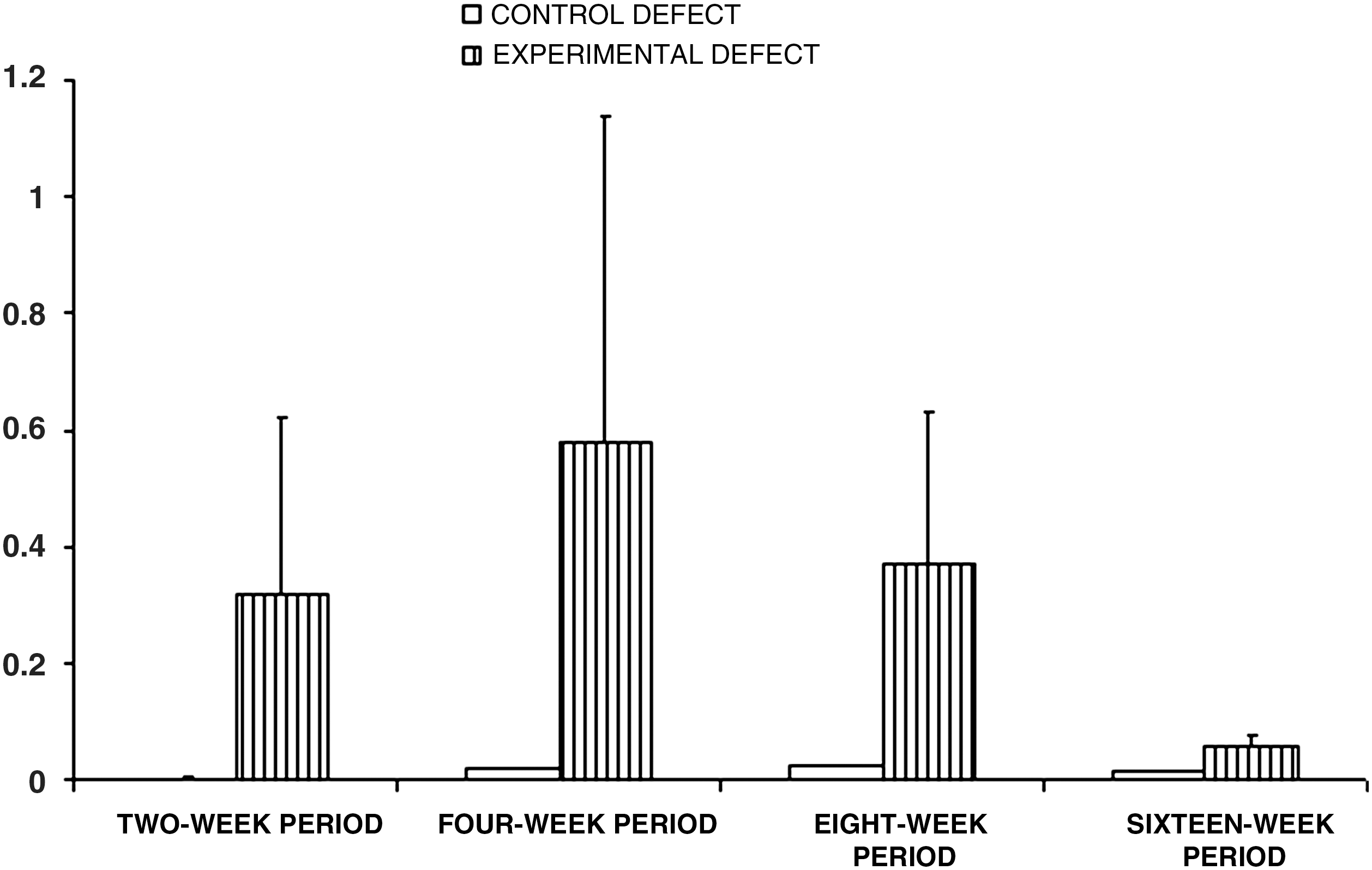
Mean ± SEM equilibrium load (MPa) of the studied groups. There were no significant differences between the studied groups.
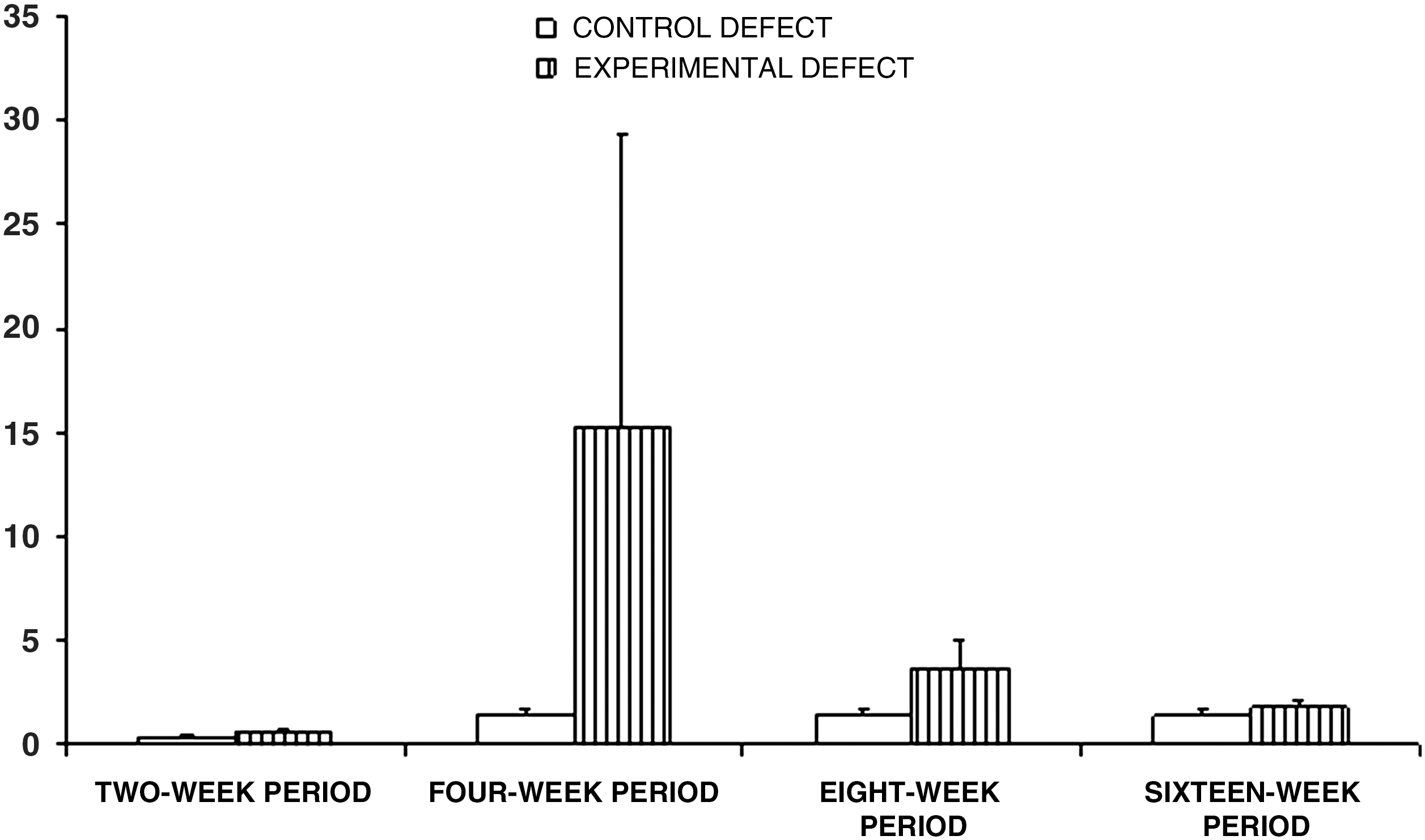
Mean ± SEM of the first part of the energy absorption (MPa × s) of the studied groups. There were no significant differences between the studied groups.
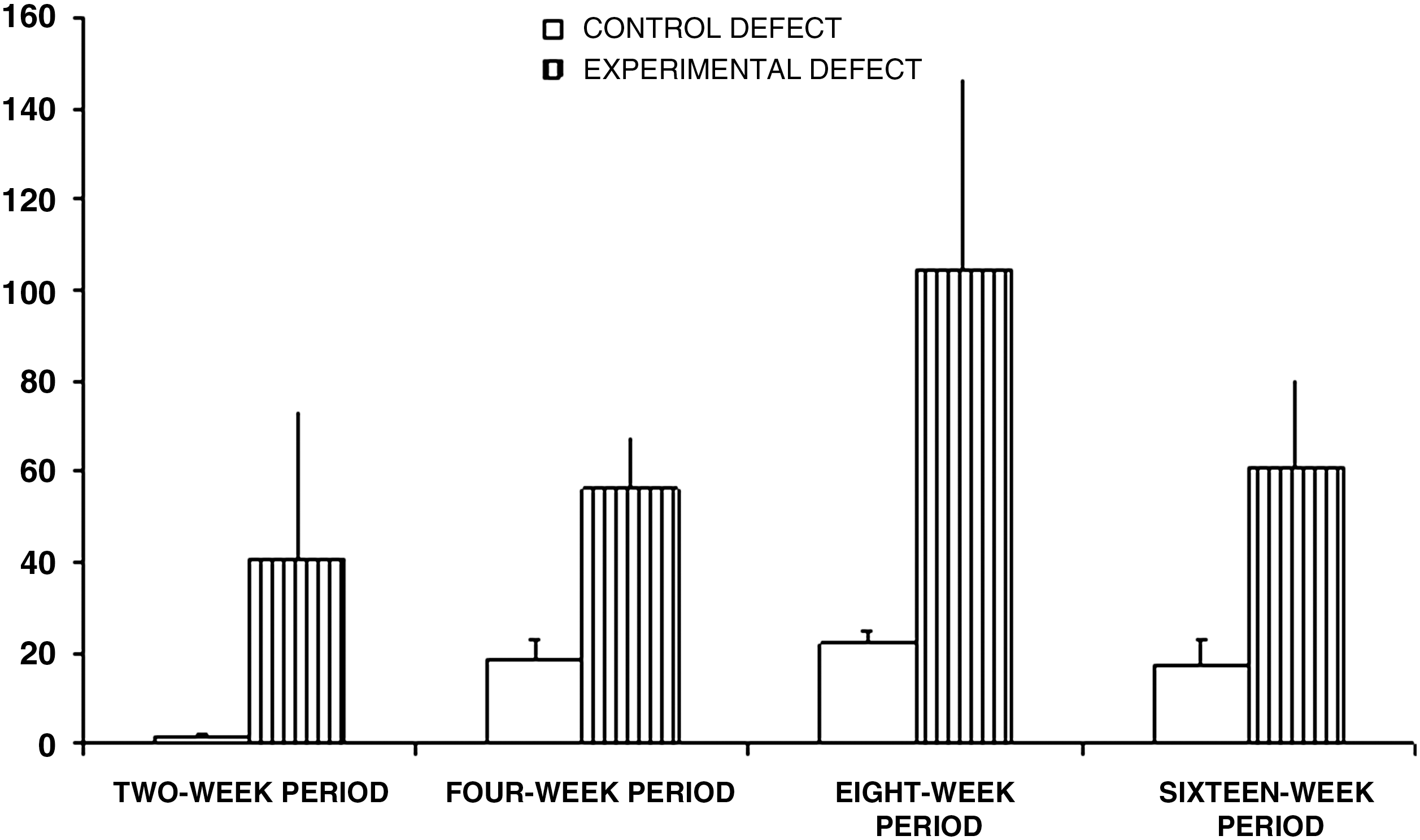
Mean ± SEM of the second part of the energy absorption (MPa × s) of the control and experimental groups. The second part of the energy absorption of the experimental group in the 4-wk study period was significantly higher than that of the relevant control group (p = 0.015).
The 2-wk study period
There were no significant differences in IS, MF, EL, FEA, and SEA between the control and experimental groups.
The 4-wk study period
There were no significant differences in IS, MF, EL, and FEA between the control and experimental groups. However, the SEA of the experimental group (56.11 ± 11.5) was significantly higher than that of the control group (18.9 ± 4) (p = 0.015).
The 8-wk and 16-wk study periods
There were no significant differences in any of the biomechanical parameters between the control and experimental groups.
Results of statistical analysis within study periods of control group
There were significant differences between the 2-wk study period compared with the 4-wk study period, and the 2-wk study period compared with the 16-wk study period in all studied biomechanical parameters:
The 4-wk study period vs. the 2-wk study period
The mean of IS, MF, FEA, SEA, and EL for the 4-wk study period were significantly higher than for the 2-wk study period (LSD test, p = 0.018, p = 0.013, p = 0.01, p = 0.01, and p = 0.018, respectively).
The 8-wk study period vs. the 2-wk study period
The mean of FEA, SEA, and EL for the 8-wk study period were significantly higher than for the 2-wk study period (LSD test, p = 0.009, p = 0.003, and p = 0.005, respectively).
The 16-wk study period vs. the 2-wk study period
The mean of IS, MF, FEA, SEA, and EL for the 16-wk study period were significantly higher than for the 2-wk study period (LSD test, p = 0.022, p = 0.041, p = 0.01, p = 0.014, and p = 0.044, respectively).
Results of statistical analysis within study periods of the experimental group
The mean of IS for the 8-wk study period was significantly higher than that for the 2-wk study period (LSD test, p = 0.003). The mean of EL for the 4-wk study period was significantly higher than for the 2-wk, 8-wk, and 16-wk study periods (LSD test, p = 0.03, p = 0.036, and p = 0.008, respectively).
Discussion
The literature indicates that radiation that is emitted by a He–Ne laser has greater coherence properties than other therapeutic lasers (diodes), 13 neutralizing the adverse effects of knee-joint immobilization 3,6 and inducing cartilage neoformation in a damaged articular cartilage mode. l,8
He–Ne laser irradiation with the energy-density and delivery parameters that were applied in the current study could significantly increase one of the important biomechanical parameters of repairing osteochondral defect 4 wk after surgery in comparison with the relevant control group. However, further studies with different energy densities and delivery parameters of He–Ne lasers are needed to demonstrate probable positive effects of the laser on repairing an osteochondral defect. Despite of the present study's failure to show a positive effect of LLLT on repairing the osteochondral defect from a biomechanical standpoint, further biochemical and molecular analysis may reveal a positive effect of the laser. In this regard, the positive effect of He–Ne laser on other models of cartilage damage have been shown. 3,6,8
Peccin et al. 8 have reported a positive effect of He–Ne laser on the healing of articular cartilage damage. Peccin et al. 8 used internal controls. However, the systemic effect of LLLT has been reported in previous studies. 14 –16 In this regard, Khadra et al. 16 have reported that LLLT can stimulate the release of substances such as growth factors and cytokines into circulatory systems, so the laser could affect the untreated side of experimental animals or subjects. 16 On the other hand, Peccin et al. damaged articular cartilage, whereas in the current study damage was penetrated deep into subchondral bone.
Results of the analysis between the control and experimental groups of the current study showed significantly higher energy absorption in the 4-wk study period of the experimental group in comparison with its relevant control group.
It seems that the results of a previous study by the current author, 12 who reported a significant increase in stiffness of an infrared (GaAs) laser-treated repairing osteochondral defect, was superior to the results of the present study. A comparison of the results in the present study with our previous study 12 suggests that infrared laser with a longer wavelength penetrates into the repairing tissue more deeply than He–Ne laser with a shorter wavelength. 11
The results of the current study also suggest that He–Ne laser irradiation does not penetrate deeply enough to produce a biostimulatory effect that would increase most of the biomechanical parameters throughout the study period to repair the osteochondral defect. The results of the current study are consistent with those of Calatrava et al. 17 Calatrava et al. made a lesion on the hind limb of normal rabbits. The animals were then divided into two groups: one group was treated with He–Ne laser and the other with infrared laser. Histological examination at the end of the treatment showed hyaline cartilage in the infrared laser group, fibrocartilage in the He–Ne laser group, and granulation tissue in the control limbs. Calatrava et al. 17 concluded that infrared laser produces better results in deep pathology than the He–Ne laser.
The results of our current study indicate a relatively high variation in biomechanical parameters between rabbits. This point is consistent with the results of Lyyra et al. 18 Lyyra et al. characterized the topographical variation of stiffness of human knee articular cartilage in vivo. They also reported a relatively high variation in cartilage stiffness between individuals. 18 In our study, the ANOVA test showed that, in the control group, there were significant differences between the biomechanical parameters of the 2-wk study period compared with the other study periods. At this point, the defect was filled with some mesenchymal cells assuming the rounded form of chondrocytes and beginning to synthesize ECM, which contains type-two collagen and a relatively high concentration of proteoglycan. 19 This is the reason for the significantly inferior biomechanical properties of this group. The results of the experimental group in our study showed that there were no significant differences in biomechanical parameters between the 2-wk study period and other study periods in most cases. As we have pointed out, these results may be due to LLLT-induced biostimulation of the chondrocytes in the defect to synthesize and release ECM and to improve the collagen network. So the biomechanical parameter values of the experimental subgroups did not show significant differences between each other in the most cases.
Conclusion
It is concluded that LLLT with a He–Ne laser of an osteochondral defect in rabbits cannot significantly accelerate the healing of the osteochondral defect from a biomechanical standpoint when compared with a control group. On the basis of the results of current study, it has also been indicated that LLLT could significantly increase only one important biomechanical parameters 4 wk after surgery in comparison with the control defect. However, further studies with biochemical and molecular analysis and/or different energy densities and delivery parameters of the He–Ne laser are needed to demonstrate the probable positive effects of the laser on healing an osteochondral defect.
Footnotes
Acknowledgments
We wish to thank the late Mrs. Jamileh Rezaei. We also take this opportunity to extend thanks to Mrs. Zahra Rezaian for her assistance in the biomechanical analysis; the Vice-Chancellor of Research at the Shaheed Beheshti University, M.C., for financial support (Grant no. 3/5740); and Miss Nasrin Khaterie for drawing the figures.
Author Disclosure Statement
No competing financial interests exist.