
Abstract
Introduction
Low-level laser therapy (LLLT) has been widely used to treat soft tissue injuries. 5,6 Recent studies have showed that LLLT can reduce muscle fatigue induced by electrical stimulation in rats 7 and reduce pain in patients with DOMS. 8 However, negative results have been reported in a few clinical trials examining LLLT treatment of DOMS. 9 –11 The efficacy of LLLT for the treatment of DOMS is still controversial.
Eccentric exercise-induced muscle injury is similar in pathological change and pathogenic mechanism in humans and animals. 12 Downhill running in rats has been effectively used as an animal model of eccentric exercise-induced muscle injury. 12 The purpose of this study is to investigate the effects of low-level He-Ne laser irradiation at different doses on rat muscle injury after downhill running and to provide an experimental means to study LLLT treatment for human DOMS.
Materials and Methods
Animals and experimental groups
Seventy-two female Sprague-Dawley rats weighing 180–250 g from the Central Animal House of the Medical College of Sun Yat-Sen University were used in this study. The rats were kept in individual cages with standard food and water ad libitum in proper environmental conditions. The rats were randomly divided into five groups as follows: 1) sedentary control group (n = 8); 2) exercise control group (n = 16); 3) three exercise-plus-laser groups: low-dose laser group (n =16), medium-dose laser group (n = 16), and high-dose laser group (n = 16). Each of the four exercise groups was further divided into two subgroups: a 24 h post-exercise subgroup and a 48 h post-exercise subgroup (n = 8 for each subgroup).
Exercise protocol
All rats in the four exercise groups were familiarized with treadmill running by exercising on a motor-driven treadmill for two days (5–10 min/day, at 0° and 5–10 m/min). Having acclimatized to the treadmill, each rat in the four exercise groups performed a bout of downhill running (at −16° and 16 m/min) to exhaustion. The exhaustion standard was that the rats were unable to maintain pace with the treadmill and stayed in the rear 1/3 part of the treadmill despite humane encouragement for 10 sec more than three times. The rats in the sedentary control group did not exercise.
Laser irradiation
A low-level He-Ne laser (Model HN-1000, Guangzhou, China) with 632.8 nm wavelength, 0–40 mW adjustable and continuous power output with 0.5 cm beam diameter was used. The rats of each exercise-plus-laser group were lightly anaesthetized intraperitoneally with sodium pentobarbitone (20 mg/kg) and immobilized on a rodent fixation device with their legs stretched. He-Ne laser irradiation was then applied directly to the previously shaved skin of the bilateral gastrocnemius muscle middle bellies. The laser beam was kept perpendicular to the irradiation surface. The rats in low-dose, medium-dose and high-dose laser groups received transcutaneous irradiation at doses of 12, 28, and 43 J/cm2 (powers: 4, 9, and 14 mW, intensities: 20, 46, and 71 mW/cm2, irradiation time: 10 min), respectively. The rats of the 24 h post-exercise subgroup received two subsequent laser irradiations at 0 and 18 h after exercise. The rats of the 48 h post-exercise subgroup received three subsequent laser irradiations at 0, 18 and 42 h after exercise. The rats in the sedentary control group and the exercise control group received no laser irradiation.
Tissue processing
The rats in the 24 h post-exercise subgroup and the 48 h post-exercise subgroup of the four exercise groups were anesthetized with 40 mg/kg sodium pentobarbitone at 24 and 48 h after exercise, respectively. The bilateral gastrocnemius muscles were dissected and cleaned for histological and biochemical studies and the blood samples were taken by means of cardiac puncture for creatine kinase (CK) analysis. The animals were then sacrificed by overdose of anesthesia. The animals in the sedentary control group were anesthetized and sampled in the same way as those in the four exercise groups.
Left gastrocnemius muscles for histopathological examination were immediately immersed in 4% phosphate buffered paraformaldehyde fixative for three days and then transferred in 20% sucrose overnight at 4°C for cryostat section.
Right gastrocnemius muscles for biochemical assays were immediately stored in liquid nitrogen until analysis. After rapid thawing and weighing, muscle samples were manually homogenized on ice with a glass-Teflon homogenizer, in 9 volumes of ice-cold physiological saline. Homogenates were centrifuged for 15 min at 3500 rpm (Eppendorf 5801R centrifuge, Germany), and the resultant supernatants were collected for superoxide dismutase (SOD) and malondialdehyde (MDA) analysis.
Immediately after sampling, blood specimens were centrifuged for 10 min at 3,000 rpm for serum separation. Serum specimens were stored in an ultra-low temperature freezer (Thermo Forma 725) at −80°C for later analysis.
Histology and semi-quantitative analysis
Following dehydration in 20% sucrose, muscles were longitudinally cut at 10 μm using a cryostat (Leica, Germany). Alternate serial sections were obtained in the muscle middle belly and stained with hematoxylin and eosin (H&E).
The sections were morphologically analyzed by light microscope. The degree of inflammatory cell infiltrate was semi-quantitatively assessed according to the following criteria: 1) unmarked infiltrate: less than 1 focus (a focus was defined as >10 inflammatory cells clustered together), 13 none or few inflammatory cells per low power field (× 10); 2) marked infiltrate: from 1 to 5 foci per low power field; 3) large infiltrate: more than 5 foci or diffuse (more than 30 inflammatory cells clustered together) per low power field.
Biochemical assays
Serum CK activity was measured by the method of colorimetric phosphorus determination. The serum CK activity was expressed in units/liter (U/l), with one unit of activity causing the phosphorylation of one micromole of creatine per minute, at 25°C.
Muscle SOD activity was detected by xanthine oxidase assay. SOD activity is expressed in units per milligram of protein (U/mg protein). One unit (U) means 50% inhibition by SOD of nitric ion production.
Muscle MDA content was determined by thiobarbituric acid assay (TBA). MDA content was expressed as nanomoles per milligram of protein (nmol/mg protein).
All kits for CK, SOD, and MDA were provided by Nanjing Jiancheng Bioengineering Institute, Jiangsu, China.
Statistical analysis
Data are expressed as mean ± standard error of the mean (SEM). Differences between means were tested for statistical significance by a one-way ANOVA post hoc test. The statistical level of significance was set at P < 0.05.
Results
Time to exhaustion
The time to exhaustion was 240 ± 81 min. There were no significant differences between the four exercise groups.
Muscle histology
In the sedentary control group, muscle fibers exhibited visible cross striations and juxtaposed into well-organized fascicles, with neither vascular congestion nor inflammatory cell invasion in the perimysium.
In the exercise control group, there was a remarkable inflammatory reaction in exercised muscles. At 24 h after exercise, interstitial vascular congestion was observed, and numerous neutrophils, monocytes and macrophages were seen in localized areas of the muscular interstitium and in some degenerating muscle fibers (Figs. 1A and 2A). The infiltrate of inflammatory cells, especially macrophages, at 48 h after exercise was more marked than that at 24 h after exercise (Figs. 1, 2A, and 3A).
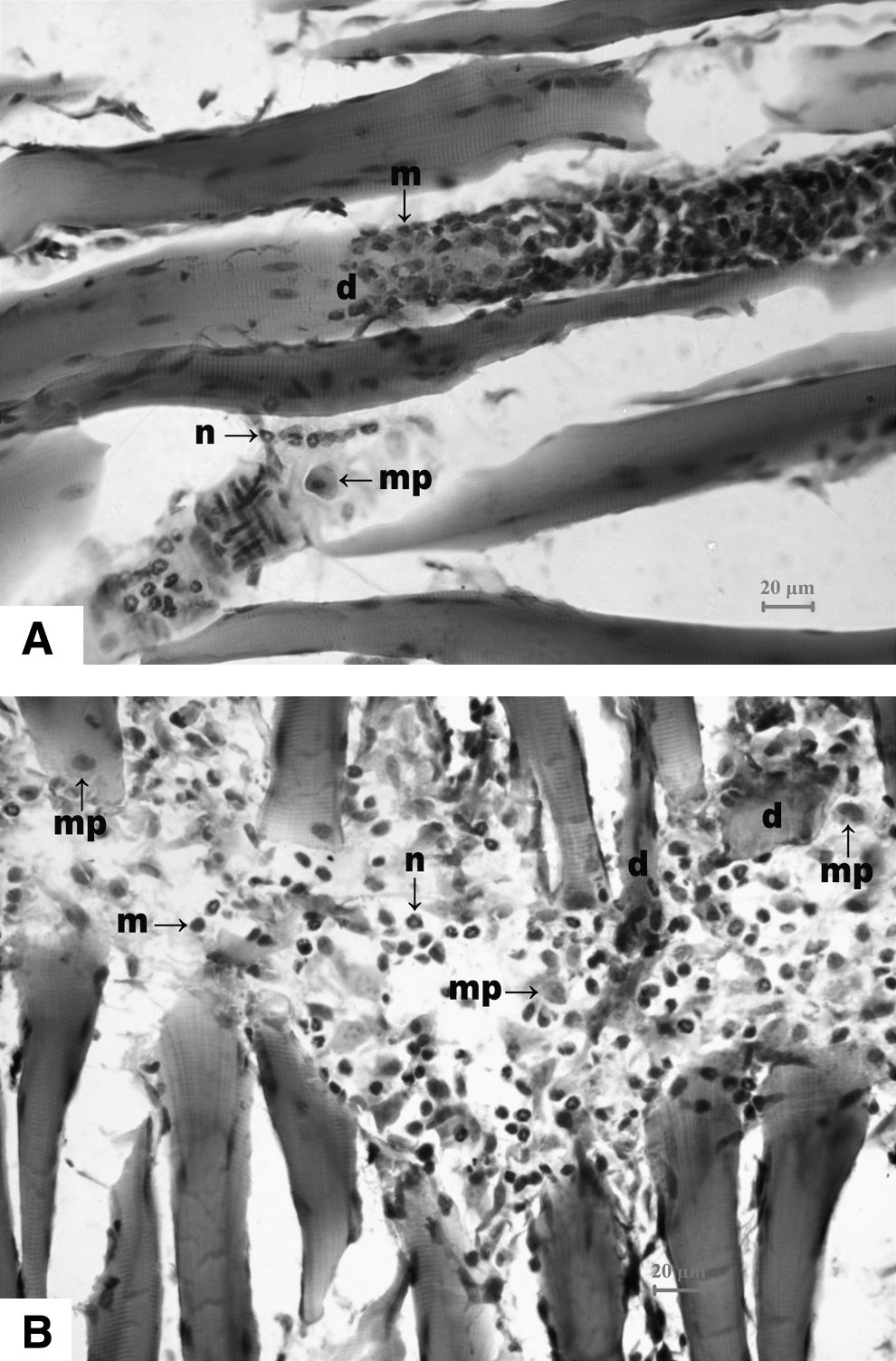
Longitudinal sections of unirradiated gastrocnemius muscle at (
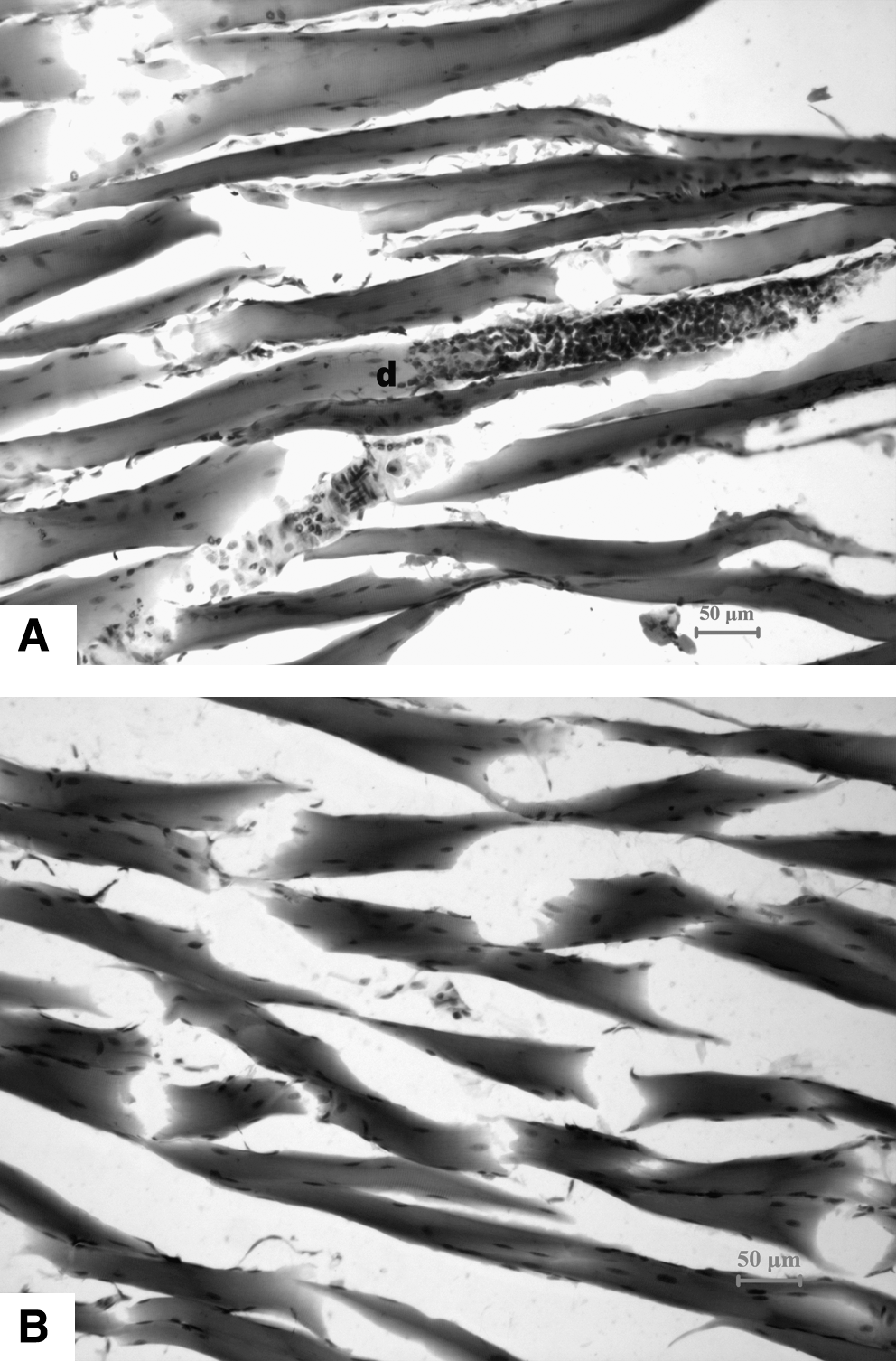
Longitudinal sections of gastrocnemius muscle at 24 h after exhaustive downhill running (
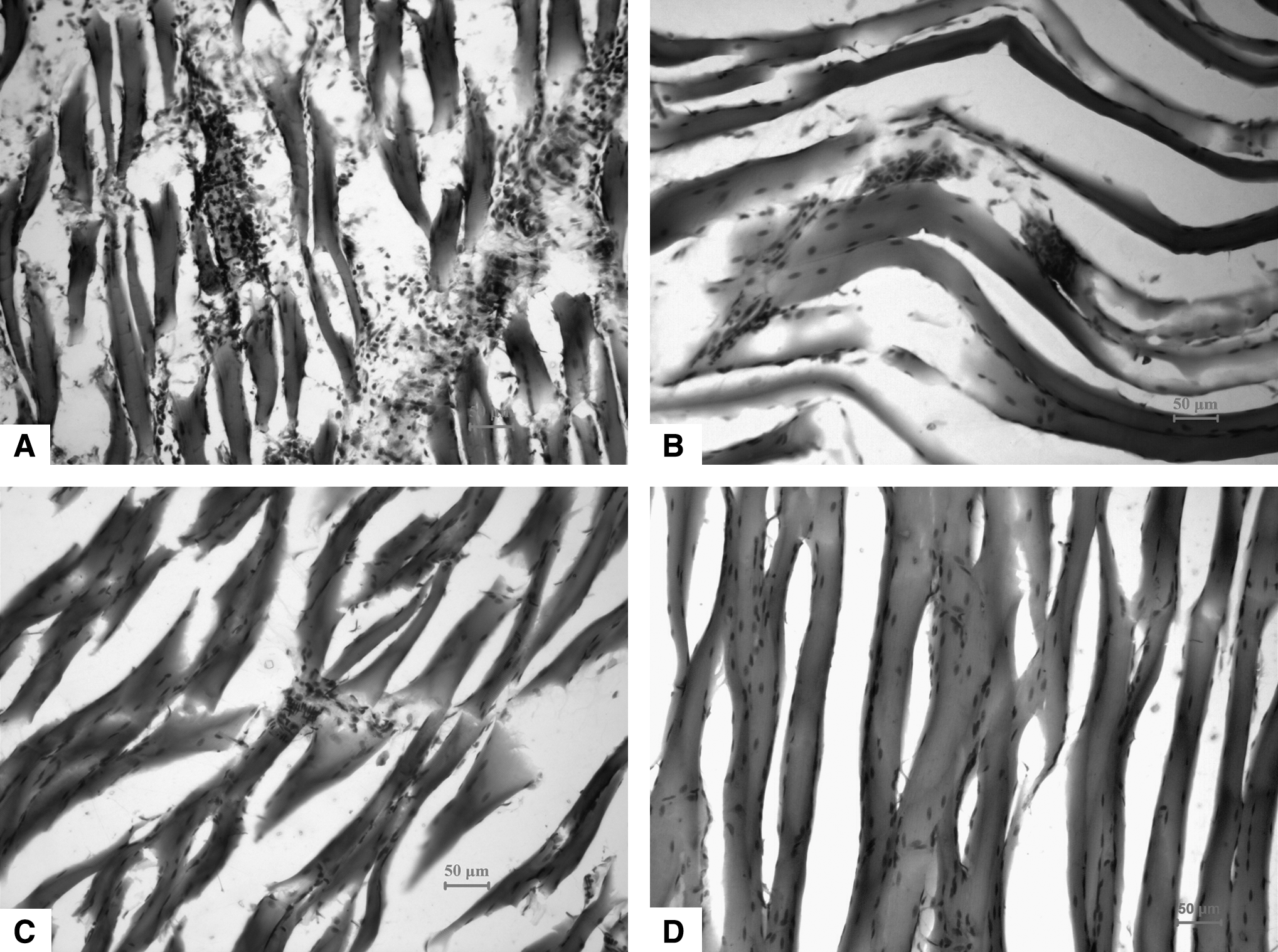
Longitudinal sections of gastrocnemius muscle at 48 h after exhaustive downhill running (
In the three exercise-plus-laser groups, muscle inflammation was attenuated and the extent of muscle damage was reduced at both 24 and 48 h after exercise (Figs. 2 and 3). There was a qualitative difference in the amount of fibers undergoing necrosis between the exercise control group (Figs. 2A and 3A) and either the high-dose laser group at both 24 (Fig. 2B) and 48 h (Fig. 3D) after exercise or the medium-dose laser group at 48 h after exercise (Fig. 3C). In the high-dose laser group, fibers undergoing necrosis were hardly seen at both 24 (Fig. 2B) and 48 h (Fig. 3D) after exercise. Semi-quantitative analysis for inflammatory cell infiltrate showed that the highest dose of 43 J/cm2 had the strongest inhibiting effect on inflammatory cell infiltrate and the lowest dose of 12 J/cm2 had the weakest inhibiting effect at both 24 and 48 h after exercise among the three doses used (Table 1).
Serum CK activity
In the exercise control group, serum CK activity significantly increased, by 123%, at 24 h after exercise and further significantly increased, by 232%, at 48 h after exercise over the sedentary control level. Serum CK activity in the high-dose laser group was significantly lower than that in the exercise control group at both 24 (P < 0.05) and 48 (P < 0.01) hours after exercise, and was not significantly different from the sedentary control level at the same times (Fig. 4). The low-dose and medium-dose laser groups showed significantly lower serum CK activity than the exercise control group at 48 h after exercise only (P < 0.01) (Fig. 4).
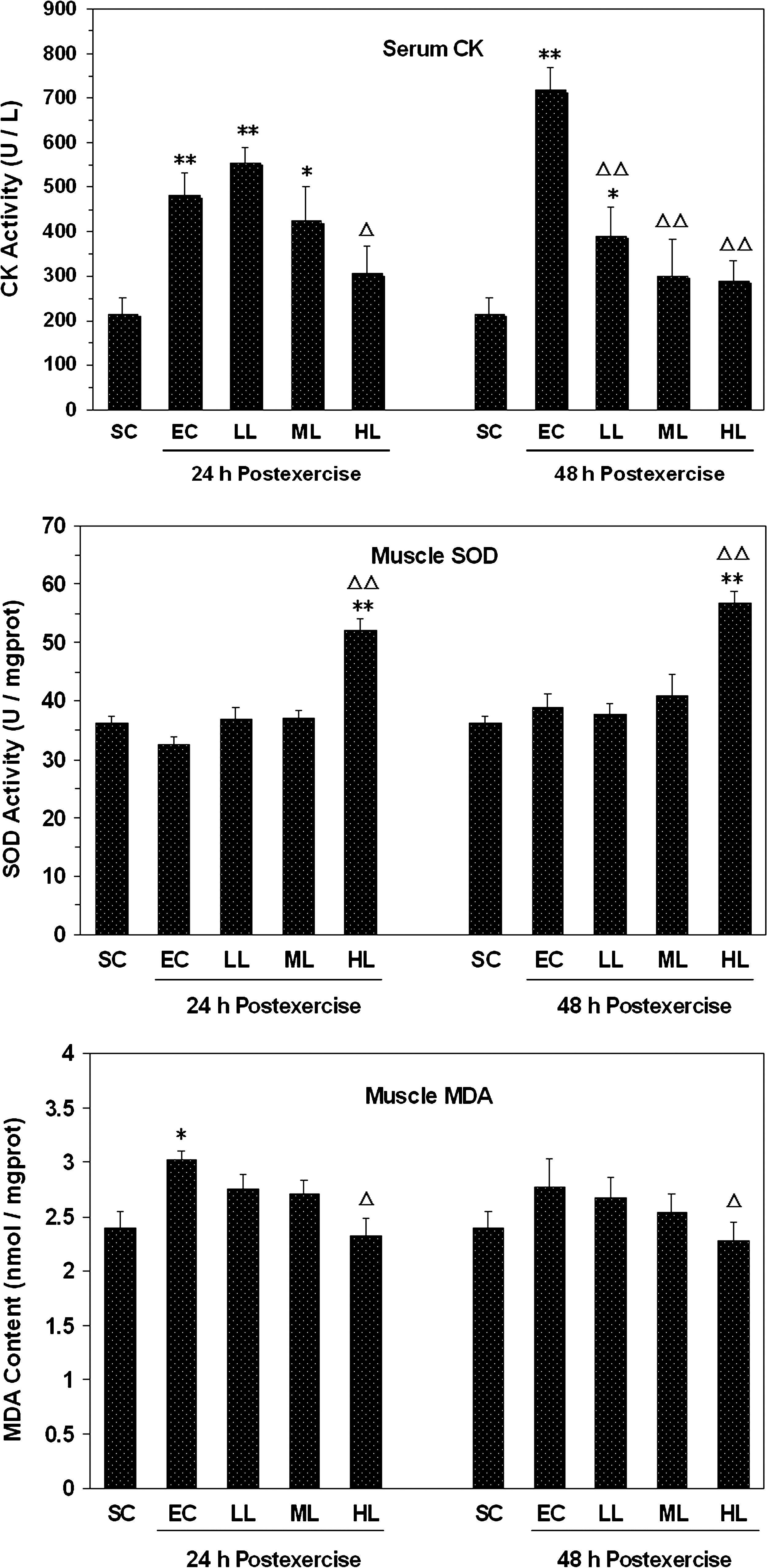
Serum creatine kinase (CK) activity, muscle superoxide dismutase (SOD) activity and muscle malondialdehyde (MDA) content in sedentary control group (SC), exercise control group (EC), low-dose laser group receiving 12 J/cm2 (LL), medium-dose laser group receiving 28 J/cm2 (ML) and high-dose laser group receiving 43 J/cm2 (HL) at 24 and 48 h after exhaustive downhill running. Asterisks indicate significant differences from the sedentary control group (*P < 0.05, **P < 0.01). Triangles indicate significant differences from respective exercise control subgroup (ΔP < 0.05, ΔΔP < 0.01).
Muscle SOD activity
Muscle SOD activity in the exercise control group was slightly lower at 24 h after exercise and slightly higher at 48 h after exercise than the sedentary control level, but the differences at both 24 and 48 h after exercise were not significant. In the high-dose laser group, muscle SOD activity increased by 44% at 24 h after exercise and by 58% at 48 h after exercise over the sedentary control level. The high-dose laser group showed significantly higher muscle SOD activity at both 24 and 48 h after exercise than the exercise control group (P < 0.01) (Fig. 4).
Muscle MDA content
In the exercise control group, muscle MDA content increased significantly, by 26%, over the sedentary control level at 24 h after exercise, and was close to the sedentary control level at 48 h after exercise (Fig. 4). At both 24 and 48 h after exercise, muscle MDA content in the high-dose laser group was significantly lower than that in the exercise control group (P < 0.05), but not significantly different from the sedentary control level (Fig. 4).
Discussion
The present study demonstrates that LLLT with He-Ne laser brought about photobiomodulation on eccentric exercise-induced rat muscle injury and that the dose of 43 J/cm2 (71 mW/cm2, 10 min) was the most efficient among the three doses applied (12, 28, and 43 J/cm2).
Our results showed that inflammatory cell infiltrate in gastrocnemius muscle (Figs. 1, 2A, and 3A, Table 1) and the elevation of serum CK activity (Fig. 4) were marked at 24 h after downhill running and more marked at 48 h after downhill running, which was consistent with the observations of previous reports. 12,14 The imbalance between oxidation and anti-oxidation in the exercise control group was obvious at 24 h after downhill running (Fig. 4). Eccentric exercise-induced muscle injury has been generally considered to include both a primary damage phase and a secondary damage phase. 1,3 The initial injury may be induced by mechanical damage of muscle cell structures 12,15 and the secondary damage may result from excessive free radicals in muscular tissue which may be generated through three main pathways: mitochondrial production, ischemia-reperfusion, and inflammatory response. 16,17 Our results support the viewpoint that excessive free radicals might mediate the secondary damage after exhaustive eccentric exercise.
In this study, low-level He-Ne laser irradiation provided several beneficial effects for eccentric exercise-induced muscle injury. The exercised muscles irradiated with the 43 J/cm2 dose (71 mW/cm2, 10 min) showed less inflammatory cell infiltrate and fewer necrotic fibers than the unirradiated exercised muscles at both 24 and 48 h after exercise (Figs. 2 and 3, Table 1). The histopathological findings were consistent with the biochemical CK data, which may be used as an indicator of muscle damage, 1 since the serum CK level in rats irradiated with the 43 J/cm2 dose had a significant reduction over the exercise control level at both 24 and 48 h after exercise (Fig. 4). These results indicated that low-level He-Ne laser irradiation could reduce eccentric exercise-induced muscle injury in rats. In several animal experiments using other muscle injury models, similar results were reported (i.e., that LLLT could reduce serum CK level after muscle injury within the dose range of 1–800 J/cm2). 7,18,19
The effect of LLLT on the metabolism of free radicals after eccentric exercise was also investigated in this study. Our results showed that He-Ne laser irradiation at 43 J/cm2 (71 mW/cm2, 10 min) significantly enhanced muscle SOD activity and reduced muscle MDA level after eccentric exercise. Some studies have reported that LLLT can enhance SOD activity in rat tendon tissue and brain tissues, 20,21 reduce mitochondria-derived free radicals in C2C12 myotubes 22 and inhibit respiratory burst in bovine neutrophils. 23 It has been suggested that the change in the cellular redox state leads to photobiostimulative processes. 5,24 The above data suggests that low-level He-Ne laser irradiation may reduce eccentric exercise-induced muscle injury through diminishing excessive free radicals.
A dose-response pattern for LLLT was observed in this study. The effects of He-Ne laser irradiation on eccentric exercise-induced muscle injury increased with dose from 12 to 43 J/cm2, and the highest dose of 43 J/cm2 (71 mW/cm2, 10 min) was the most efficient. The effective irradiation dose for muscle injury should be location-specific. To penetrate thicker human skin, it would be necessary to increase this laser dose. A few clinical studies have investigated the effects of phototherapy on DOMS. Two studies have found no significant effects from combined laser and light-emitting diode therapy with 660–950 nm wavelengths at 31.7 J/cm2 (44 mW/cm2, 12 min) and 11 J/cm2 (46 mW/cm2, 4 min), respectively. 9,10 An additional study also failed to find significant effects from monochromatic infrared therapy, using 840 nm wavelengths at 3 J/cm2 (10 mW/cm2, 5 min). 11 Douris et al. found that light-emitting diode therapy using 660 nm and 880 nm wavelengths at 8 J/cm2 (100 mW/cm2, 80 sec) could reduce pain but could not improve muscle function in patients with DOMS. 8 For photobiomodulation, the dose is important, but the intensity might be more important. 5,25 It has been shown that the intensity of the source is a major factor that determines quality and quantity of the response for photobiomodulation at a constant total dose. 26 The intensities in the studies of Craig et al. 9,10 and Glasgow et al. 11 may be too low for the phototherapy to effectively treat human DOMS. The phototherapy given by Douri et al. 8 has been effective in reducing pain, and might be more effective in improving muscle function at higher intensity and/or dose in view of our study. Of course, further studies should be done to identify the optimal intensity and dose of LLLT for the treatment of DOMS.
Conclusion and Summary
Low-level He-Ne laser irradiation could exert therapeutic effects on eccentric exercise-induced rat muscle injury through enhancing muscle anti-oxidative capacity and reducing inflammatory reaction in muscular tissue. The effects of He-Ne laser irradiation on the muscle injury depended on laser intensity and dose, and the dose of 43 J/cm2 (71 mW/cm2, 10 min) was the most efficient among the doses used.
Footnotes
Acknowledgments
This work was supported by National Science Foundation of China (60878061), Major Program of Science and Technology Research of Ministry of Education (10420), and the Opening Project of MOE Key laboratory of Laser Life Science, South China Normal University, Guangzhou, China.
Author Disclosure Statement
No competing financial interests exist.