
Abstract
Introduction
Studies that employed lasers with different fluences found significant increases in the viability of skin flaps 5 –9 and transverse rectus abdominis musculocutaneous flap, 10 but the influence of the output power in relation to the other parameters was not revealed, including comparison between the powers.
Most studies in skin flaps have used red visible laser with an output power of 30 mW 9,11,12 and found improved viability of skin flaps, as demonstrated in a study 12 that used 60 mW with infrared laser.
Laser irradiation can reduce necrosis in random skin flaps, 8,11 and the positive effects of laser irradiation in the viability of skin flaps seem to be due to stimulation of the formation of new blood vessels, improving blood flow through the flap. 13 –16 Nevertheless, the exact mechanisms of action and protocols of treatment for laser therapy have not been adequately defined. 16,17
Aiming to broaden the understanding of the parameters involved in laser therapy, the presented study analyzed the effect of a LLLT using two different output powers (30 and 60 mW) in the viability of a random skin flap in rats.
Methods
The Federal University of Sao Paulo's Ethical Committee approved the present study. Thirty-six male adult Wistar-EPM rats, weighing between 260 and 300 g, were randomly distributed into three groups: sham (SG), 30-mW output power (30G), and 60-mW output power (60G). The animals were maintained in individual cages with controlled temperature (22–23°C) and 12-h light-dark cycle.
After anesthesia with ketamine (100 mg/kg) and xylazine (50 mg/kg), intramuscularly, the animals had their dorsal areas depilated and were ventrally positioned over a flat surface. A cranially based, random dorsal flap (4 × 10 cm) 18 was elevated and a plastic barrier positioned between the flap and its donor bed (Fig. 1). Suture with 4–0 nylon simple stitches completed the procedure.

Random skin flap elevated with a plastic barrier (10 × 4 cm).
Two minutes after flap elevation, laser irradiation was applied, being repeated on postoperative days 1, 2, 3, and 4. A low-level laser with 660-nm (aluminium gallium indium phosphide) wavelength (Thera laser, DMC Equipamentos Ltda., São Carlos, Brazil), continuous wave, beam transversal sectional area 0.028 cm2, fluency 3 J/cm2, was used, with 30 mW of output power (30G) (total energy 1.44 J) and 60 mW of output power (60G) (total energy 1.44 J). Laser irradiation was delivered with a punctual contact technique, with 24 points inside and around the flap (Fig. 2). The equipment was calibrated in the Physics Department of University of São Paulo. Before each application, the calibrator was adjusted. Radiant power determination was realized by attaching the extremity of the laser diode, at a 90° angle, to the digital potency analyzer sensor, calibrated and used according to the manufacturer's instructions.

Scheme of laser irradiation on 24 points, using the punctual contact technique.
Irradiation was carried out through a perforated plastic template of the flap, which delineated each point of laser treatment. 8 Sham animals were exposed to a simulation of laser irradiation (SG).
On postoperative day 7, the rats were anesthetized and the analysis procedure followed. Euthanasia by anesthetic overdose followed.
Analysis
Macroscopic analysis of necrosis percentages
Percentages of necrosis were calculated on postoperative day 7 using the paper template method. 19 After anesthesia, each flap's limit between viable skin and necrosis was delineated with a pen. A template of the whole flap and the necrotic area was delineated in transparent paper by blinded observers and digitalized with a scanner. With Adobe PhotoShop software, the number of pixels in the total flap area and the necrosis area were determined. 20 The percentage of necrosis was calculated by dividing the number of pixels from the necrosis area by the number of pixels from the total flap area and multiplying by 100.
Microscopic analysis of vascular densities
After macroscopic delineations, four fragments of each flap were collected to allow determination of the vascular density using vessel morphometric analysis. 21
Selection of four fragments of each flap for histological analysis started at the cranial base (Fig. 3). Four laminas for each fragment, from each animal, were colored with hematoxylin and eosin (HE) and analyzed using the bidimensional method of morphometric counting of blood vessels to SG, 30G, and 60G, with p ≤ 0.05.
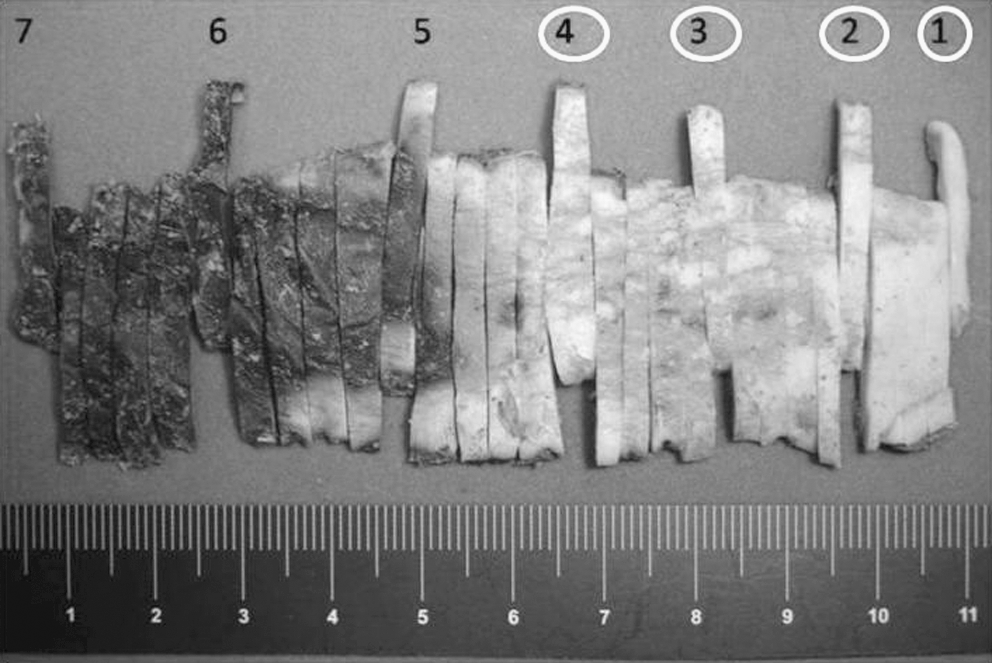
Selection of four fragments of each flap for histological analysis starting at the cranial base. The numbers with circles are examples of the fragments chosen.
Micrographic photographs were obtained using a digital camera (Sony Cyber Shot with 7.2 megapixels, Sony, Japan) adapted to an optical microscope (Carl Zeiss, Germany), in 400 × augment. A grid with 100 points was superimposed over the photographs, and the vessels that coincided with these points were counted. Vascular density was expressed in percentages. Two blinded researchers made these measurements. For statistical analysis, the mean values of blood vessels obtained from the laminas of each animal were considered.
Statistical analysis
Means and standard deviations were used to present the results. To Wilcoxon test was used to analyze agreement between the two observers. Kruskal-Wallis variance analysis was used to identify changes between groups with regard to the variables necrosis and percentages of blood vessels. A significance level of 5% was elected (p ≤ 0.05).
Results
Regarding comparison of the agreement between observers to necrosis and blood vessels, it was observed that there was no significant difference (p < 0.9 and p < 0.4, respectively).
Figure 4 presents means and distribution of data obtained for percentages of flap necrosis in the different groups.
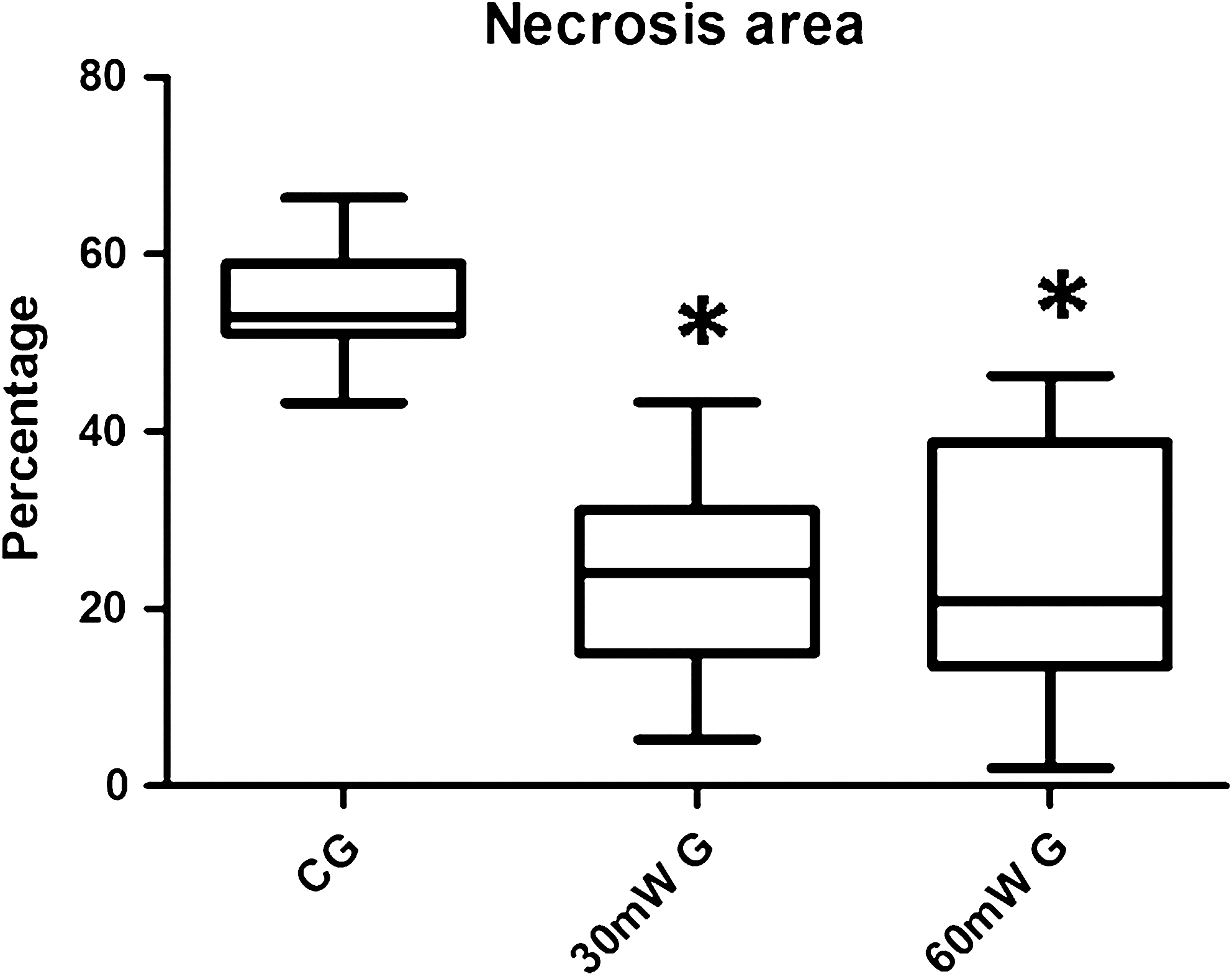
Average percentages of necrosis of the sham group (SG), the group treated with 30 mW of power (30G), and the group treated with 60 mW of power (60G). *Statistically significant compared with the SG.
Sham group animals showed a significantly higher mean percentage of flap necrosis (53%) than the laser-treated animals. This was true for rats that received laser irradiation with 30-mW output power (24%; p < 0.05) and those treated with 60-mW (25%; p < 0.05). No difference was found between laser-treated animals (p = 0.96).
Also, low-intensity laser (660 nm) in treated animals resulted in a significantly greater percentage of vascular density than control rats (SG, 37%; 30G, 57%; p < 0.05) (SG, 37%; 60G, 59%; p < 0.05). Again, no difference was found between laser-treated animals (p = 0.96) (Fig. 5, 6).
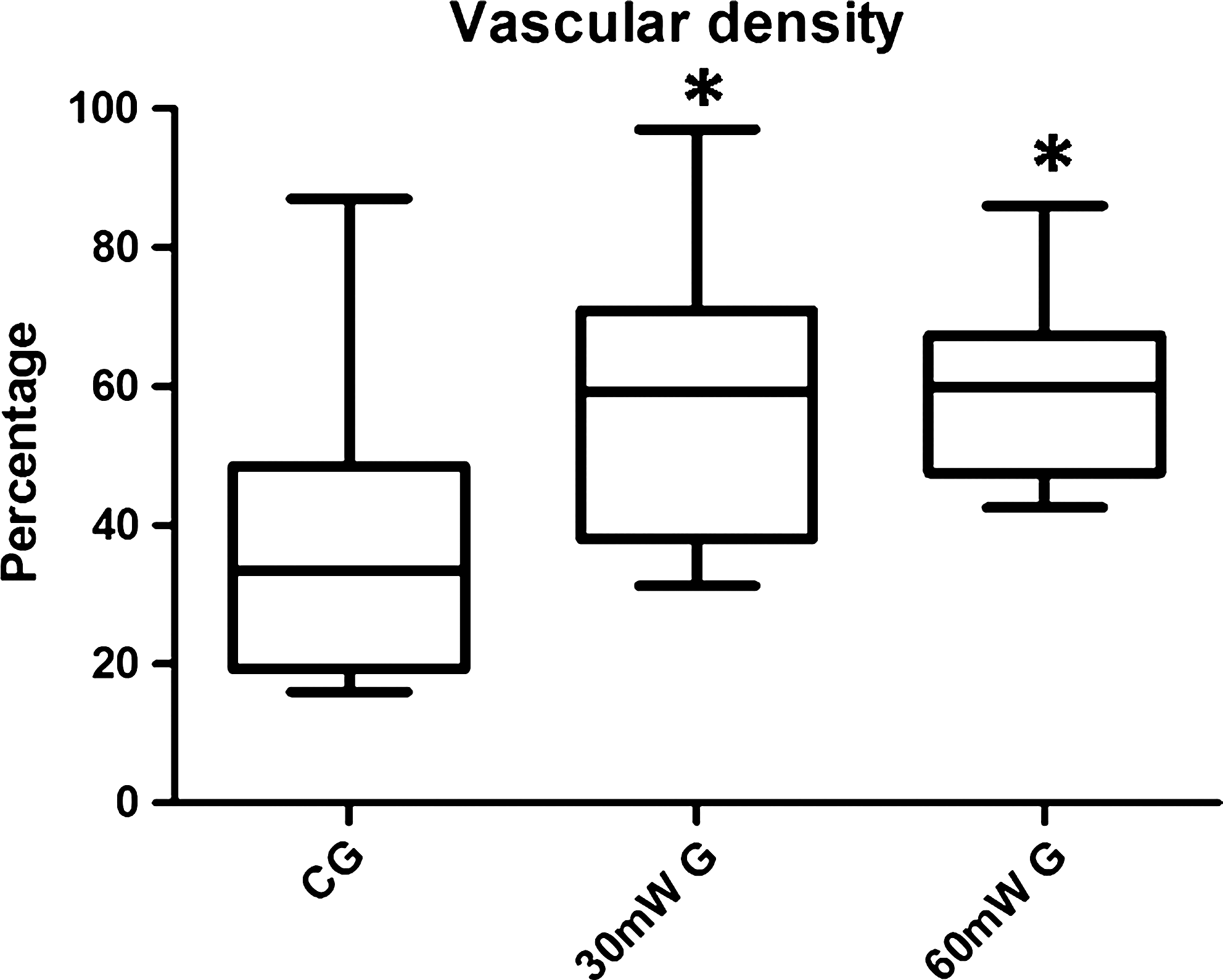
Average percentages of vascular density of the SG, 30G, and 60G. *Statistically significant compared with the SG.
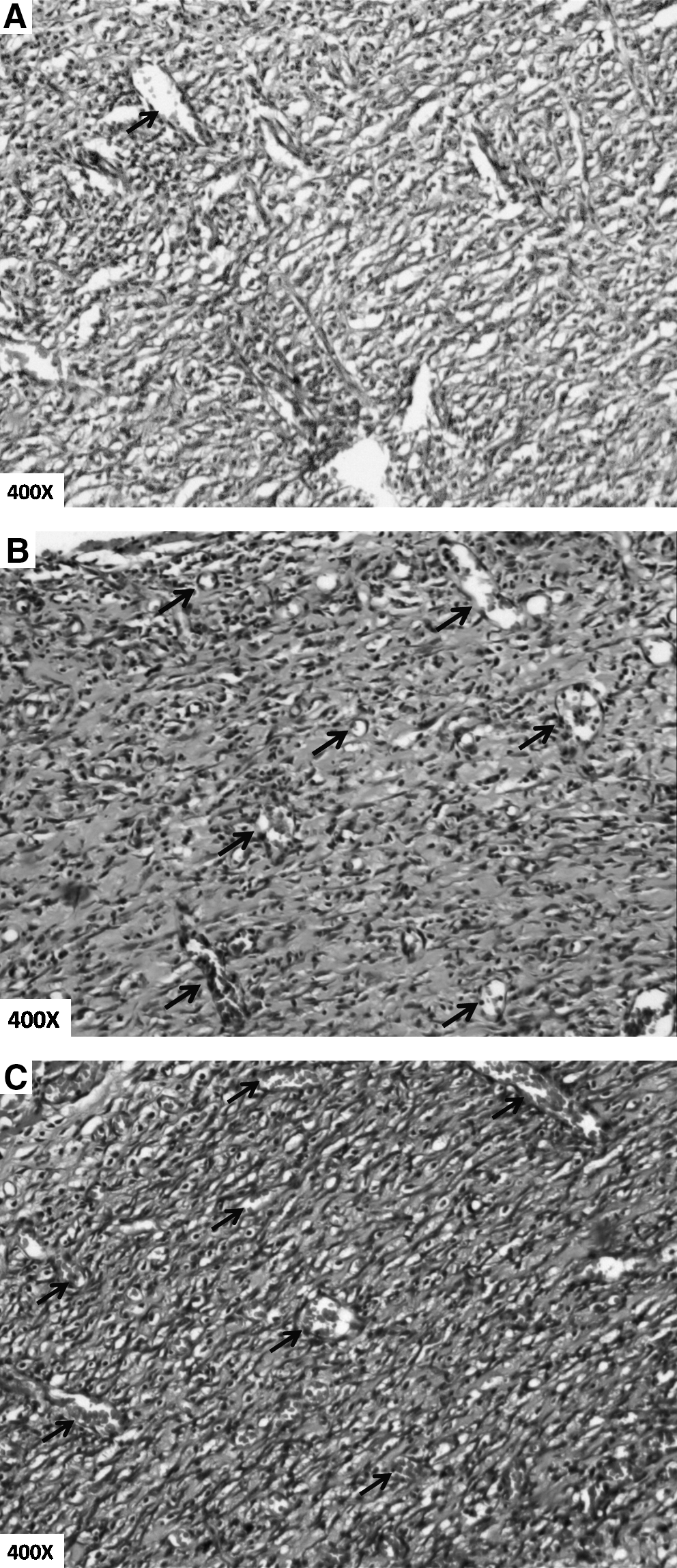
Presence of blood vessels in each group. (
Discussion
The present study investigated the vascular effects of 660-nm laser irradiation with different power output (30 mW and 60 mW), and the findings revealed that the laser produced an increase in viability of skin flap in two groups, with no differences between them.
Recent studies found significant results involving the decrease in the necrosis area through the increase of blood flow and neo-angiogenesis, 9,22 suggesting that laser irradiation increased skin flap survival due to the increase of the mitochondrial activity stimulating cell proliferation, increasing fibroblast synthesis, and increasing the fibrin absorption of the affected tissue. 15,23 LLLT action is based on light absorption by the tissues, which will generate modifications in cell metabolism.
Considering the reduction in percentage of flap necrosis, the present study is in accordance with two studies that used visible red laser with 30-mW output power. Assis et al. 12 with 16 J/cm2 fluency increased the flap viability with 73% of viable area in its treated group and Bossini et al. 9 with 3 J/cm2 fluency also obtained an increase in viability of skin flap with 41.8% in its treated group.
In addition, the results showed an increase in flap vascular density after low-intensity laser irradiation (660 nm). The 30-mW group obtained an average of 57% vascular density and the 60-mW group and an average of 59%, significantly different from the SG (37%). These results corroborate with Bossini et al., 9 who also measured an increase in blood vessels and obtained significant results in skin flaps with a total number of 92.6 vessels using the visible red laser with potency of 30 mW and energy density of 3J/cm2.
Kubota and Oshiro 7 measured flowmetry using laser Doppler and the efficacy of laser irradiation (830 nm) with output power of 60 mW. They also observed an increase in vascular perfusion and greater survival areas in flaps that were submitted to irradiation in relation to the SG, which received none.
For skin flap survival and consequently for the success of the repair procedure, adequate blood flow is essential in this area. 17,24 The development of new blood vessels is an important part of the healing process and in the reestablishment of the local circulation in the injury, repairing an ischemic lesion. 25
The methodology used in this study is in accordance with previous reports found in the literature. 8,9,11 The plastic barrier used between the flap and the donor bed prevents flap revascularization by means of bed vessels, ensuring homogeneous ischemia. 18 The punctual contact technique used for irradiation (inside and around the flap) was efficient in skin flap viability. 8 The paper template method plus a computerized analysis is rapid and avoids any small miscalculations in determining the flap's limits. In addition, the bidimensional morphometric method used to calculate the vascular density was efficient in representing the increase in the number of vessels in the flaps. As it was used by Barthe et al. 21 in the morphometric analysis in the vascularisation of the skin of delayed flaps in rabbits, Völker 26 has also used morphometric analysis in the fibril density in skin of patients with spontaneous cervical artery. Cheretis et al. 27 used morphometrical analysis to detect the recurrence tendency of basal cell carcinoma.
The present study presented some limitations. Even though we had analyzed vascular density in the viable flap area, a limitation of the transition area with the necrosis area would be necessary to provide more data in relation to the number of vessels of different areas. Differentiation of the different types of vessels (arteries and capillaries) in the vascular density count was not carried out.
Although the effects of LLLT have been demonstrated in many studies, the laser regulatory mechanisms in tissues are not well understood. 17 The output powers investigated in the present study have not presented differences when compared with each other, providing us with some perspectives as to the use of higher potencies of red laser, as well as the infrared. We observed that the output powers in visible laser are not essential to increase vascular perfusion. Output power plus the 60 mW have not been studied, and this study showed that small differences of output power did not show significant results between them. Maybe, output plus 60 mW like 80 and 100 mW can change these results. Additional research is necessary to clarify doubts related to the parameters of LLLT such as fluency, wave length, output power, and application technique, which are relevant research and divergence sources between studies.
Conclusion
LLLT (660 nm) with 30-mW and 60-mW output power was efficient in the increase of skin flap viability, but there was no difference between them.