
Abstract
Introduction
In general, animal models attempt to reflect human wound healing and associated problems such as dehiscence, ischemia, ulceration, infection, and scarring. 8 These have played a key role in furthering understanding of the underlying mechanisms involved in impaired wound healing, and also have a critical role in the testing of new therapeutic strategies including LLLT. However, with the exception of acute models, studies with animal models will at best only provide approximations of clinical problems owing to differences in tissue architecture, immune system function, physiology, and other healing responses among species.
Rodents are attractive for wound healing studies because of their availability, low cost, and ease of handling. Murine models of wound healing offer several advantages over models in other species. Mice are inexpensive, thus allowing studies to be performed with large sample sizes. Furthermore, there currently exist over 450 inbred strains of mice 9 and over 200 inbred strains of rats. 10 Moreover, there are also more than 10 different mouse models of diabetes, including genetic diabetic models. 11,12 Genetic diabetic rat models are also available, e.g. BB rat, 13 and Cohen diabetic rat. 14 While there may be considerable differences in wound healing response among inbred animal strains, 15 when using such strains, variance falls to levels that can yield significant findings with small group sizes.
Despite such advantages, mouse and rat skin healing does not perfectly mimic human skin wound healing because the skin is morphologically different. 16 Mice and rats are described as loose-skinned animals due to their skin's elasticity or redundancy, and its lack of a strong adherence to the underlying structures. 17 The properties of loose skin allow wound contraction to play a significant role in closing skin wounds; consequently, wound contraction, which is usually more rapid than epithelization, underpins shorter healing times in mouse and rat wounds. Humans have tightly attached skin and this makes comparison difficult with loose-skinned animal models. In terms of animal models, the pig is the closest to the human in skin morphology, 18 –21 but few studies have been performed in the pig because of the high cost of these animals and possible difficulties in handling.
This paper extends previous reviews in this area by critically reviewing those papers published from 2003 to date. It focuses on experimental studies that investigated laser stimulation of healing of full-thickness skin wounds in mice or rats, identifying points of similarity and difference in these various studies, and whether a clear conclusion can be reached from the data presented regarding the influence of laser irradiation on wound healing. Types of wounds included in this review are: incisional or excisional wounds, wounds with impaired healing (ischemic wounds, diabetic wounds), and burn injuries. Key characteristics of these various models are summarized in Table 1.
Laser treatment is characterized by a number of physical parameters such as wavelength, spot size, power, power density, energy, energy density, and duration of irradiation. 22 However, at present, the relevance of these parameters to the putative healing effects of laser irradiation on different injuries and skin conditions remains unclear. The review was informed by the recommendations of Tuner and Hode, who have previously identified important factors to be taken into consideration when examining such studies. 23
The aim of this paper was therefore to review experimental studies of laser irradiation of wound healing in mice and rats to assess the putative stimulatory effects of such irradiation. In addition, the current review also included assessment of: (i) The quality of the study designs and protocols used; (ii) The types of wound healing models used, and the appropriateness of these to clinical applications in humans; (iii) The relevance of irradiation parameters to any observed effects.
Materials and Methods
Original research papers investigating the effects of laser therapy on wound healing in mice and rats and published from January 2003 to August 2008 were retrieved and used for this review. Relevant papers were sought and obtained from library sources and the online databases PubMed and Medline using EndNote X1 (Thomson Corporation). Search terms were “mouse,” “murine,” “rat,” “laser therapy,” “phototherapy,” “wound healing,” and “burn.” Additional secondary sources of information included reference lists from retrieved papers, and pertinent papers identified by hand searches of relevant journals not found from the database (e.g., Laser Therapy).
We included studies that met the following criteria: (i) Laser (or other monochromatic light source) was investigated as the primary intervention (independent variable); (ii) The type of laser and precise wavelength were defined or implied; (iii) At least one outcome or index of wound healing was identified as the dependent variable; (iv) Studies were performed in whole animals (rat or mouse); (v) Studies involved skin wounds.
Studies excluded from this study were: (i) Articles published prior to 2003; (ii) In vitro studies involving cells and tissues, not whole animals; (iii) Studies reported in languages for which no English language translation was available; (iv) Studies performed in patients, or in animals other than the mouse or rat; (v) Studies involving tissues other than skin (e.g., tongue); (vi) Reviews and meta-analyses; (vii) Studies involving multisource/multiwavelength arrays, photodynamic therapy, laser surgery for creating wounds, laser welding of wounds (using high power laser irradiation), laser treatment of skin grafts over wounds; (viii) Studies for which only an abstract was available.
EndNote searches were carried out independently by two of the authors (PP, TYC); articles for inclusion and exclusion were identified independently and confirmed, thereby minimizing bias.
For included articles, the following data were extracted and tabulated by two of the authors (PP, TYC):
research method (control group, randomization or rotation procedure, and blinded outcome assessment);
sample type (animal species, sex, age and/or body weight, number of animals, division into groups, group sizes, and strain, e.g., outbred/inbred, genetic diabetic);
description of wounds (type of wound, method of creation, number of wounds, location, separation of multiple wounds, and area of wounds);
laser treatment parameters;
wound healing outcomes;
authors' conclusion (results of laser irradiation).
Studies were then critically reviewed in terms of study design, methodology (independently by PP and TYC), and appropriateness of irradiation parameters (GDB); comments on these study characteristics were also summarized and tabulated (as bold text within Tables 2 –8, and in the columns headed: Notes on study design & findings).
In Al-Watban et al., 44 the power density and energy density (fluence) are calculated using spot size.
In Corazza et al., 43 the energy density (fluence) is calculated using a circular area of skin of 1.77 cm2 removed with a 15 mm punch.
Results
Results from the literature search are summarized in Figs. 1 and 2 (for studies in the mouse and rat respectively); in total, 47 publications were included in this review (n = 8 in the mouse; 24 –31 n = 39 in the rat 32 –70 ), and are summarized in Tables 2 –8.

Flowchart of Literature Search: Studies in the mouse.
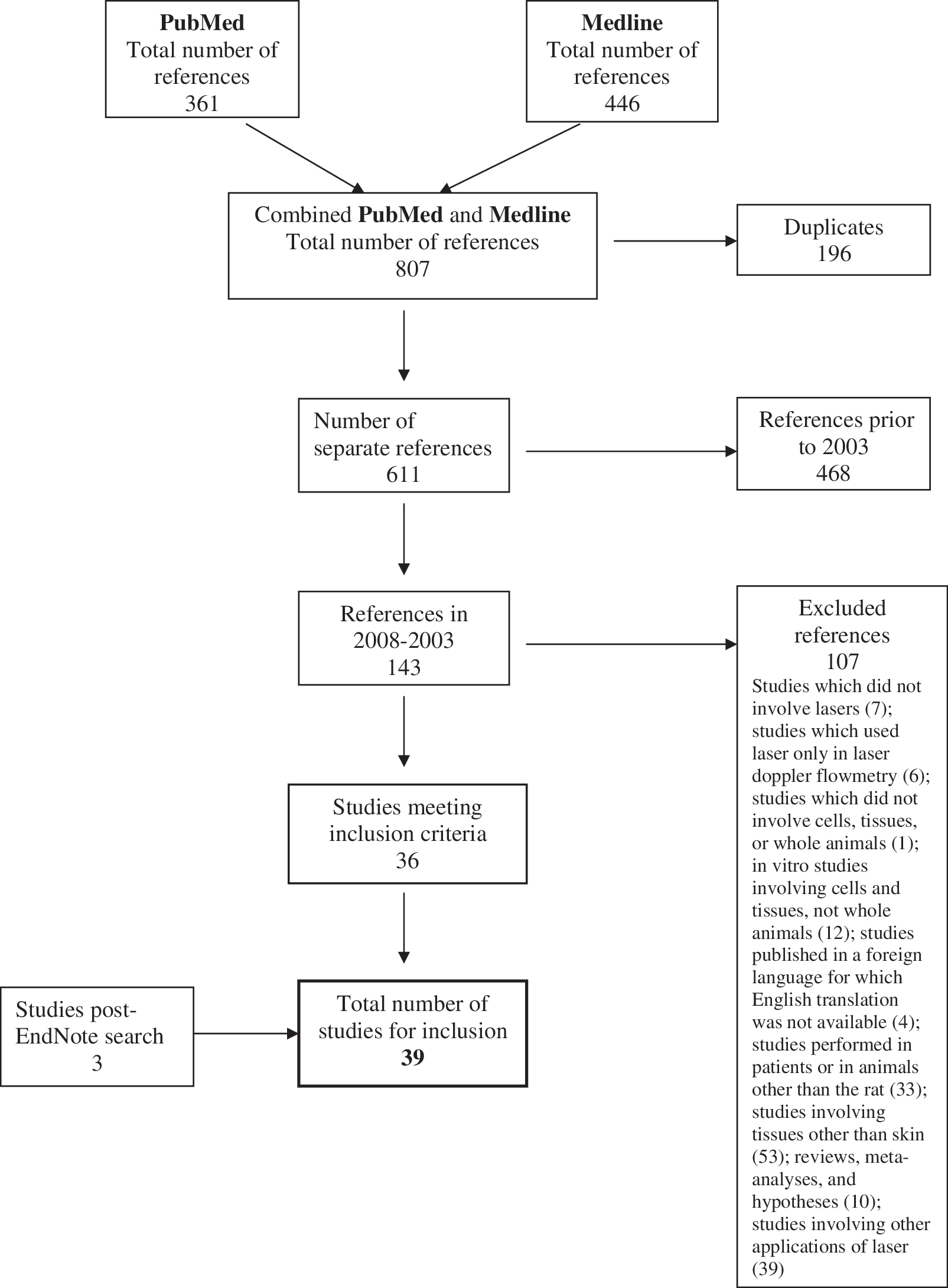
Flowchart of Literature Search: Studies in the rat.
Wound healing models
A variety of wound models were identified in the searched articles, including acute wound models (incisional; excisional – full thickness; burns – thermal, cold), impaired healing models (chemical diabetes: streptozotocin, alloxan; genetic diabetes), and chronic wounds (pressure ulcers). Further details regarding wound healing models are presented in Tables 2 –8.
Strain and sex of animals
In the eight studies using mice, six were performed with inbred strain(s); two of these studies included genetic diabetic mice. By contrast, nearly all of the 39 studies with rats were carried out using outbred strains, seven with Sprague-Dawley and 26 with Wistar rats. For the other six studies, one used an inbred strain (Lewis rats). Furthermore, in two of the studies with Sprague-Dawley rats, diabetes was induced with streptozotocin, while diabetes was induced in Wistar rats by alloxan in two of the studies and by streptozotocin in three of the studies.
Only in three of the mouse studies was the sex of the animals reported, and these included males only. Males were used in 33 of the rat studies; only five studies used females (often together with males). One study in the rat did not indicate the sex of the animals.
Weight and age of animals
Of the eight mouse studies, three reported the weights of the animals used; another two reported the age. Neither of the two studies using genetic diabetic mice indicated the weight or age of the mice.
The majority of the rat studies used animals weighing 200–350 g; however some studies comprised rats weighing 120–140 g or 170–250 g, and others 316–513 g or 450–550 g. The ages of rats were reported in few studies, and ranged from 8 weeks to 10 months; in most of the studies, only the weights of the animals were given. The Harlan Laboratory Animal Company reports that weights of 225–325 g correspond to male Sprague Dawley rats that are 8–11 weeks old (
Wound location, wound size, and number of wounds per animal
Assessment of studies was hampered by the large variation in experimental design with respect to the parameters defining the wounds, which were location, size, and number. Such differences in experimental design make it difficult to compare the findings of these studies in both the mouse and the rat. Further details of wound parameters are provided in Tables 2 –8 in the columns headed: Number, size and location of wounds.
Dressings for wounds
Only one of the mouse studies reported that the wounds were covered with an occlusive dressing (Tegaderm) for a maximum of 4 days. 29 In two of the rat studies involving excisional wounds, the wounds in each animal were covered with a perforated cellophane film. None of the other studies in the mouse or the rat reported covering of the wounds.
Laser parameters
Assessment of laser parameters used in the reviewed studies was confounded for the most part by inadequate reporting of key information, or errors in specification and/or calculation of key parameters (principally errors in calculation of dosage, expressed as either energy or radiant exposure/energy density; see notes in bold, Tables 2 –8). Beyond this, where experiments investigated the relevance of manipulation of one parameter (e.g., wavelength) to effects upon wound healing, comparison was limited by inadequate standardization of other parameters (e.g., irradiance or dosage).
Coherence
Coherence is a particular feature of laser light, and refers to the light being ‘in phase’ over space and time; in contrast, light produced by monochromatic diodes may possess all of the characteristics of laser light, with the exception of coherence. There is ongoing debate as to the relevance of this particular characteristic to the biological and thus clinical effects of laser phototherapy.
The evidence from the studies reviewed would suggest that coherence is not essential to the photobiomodulatory effects of ‘laser’ therapy. Apart from those (positive) studies which used light emitting diodes (LEDs) rather than laser diodes, several studies compared effects of laser and non-coherent sources at similar parameters and failed to show any significant differences in effects. 27,43,50
Continuous wave or pulsed radiation
Of the 22 studies that reported this parameter, i.e., whether the laser radiation was continuous or pulsed, 20 used continuous wave (CW); of the other two, one used pulsed irradiation and one used both continuous wave and pulsed. There was no study that systematically compared the effect of pulsing frequencies among the reviewed studies. As far as it is possible to determine (i.e., from review of incomplete reports of parameters), it is likely that the remaining papers (25/47) employed CW laser or light systems.
Wavelength
Wavelength (typically expressed in nm) was reported or could be established in all reviewed studies. The majority of studies (38/47) employed wavelengths within the visible red spectrum (630–685 nm), which is in keeping with original research reports in this field, based upon the use of gaseous He-Ne sources operating at 632.8 nm, 71 and routine clinical practice. 72 With the exception of one study which reported equivocal results, 70 all studies using red wavelengths reported significant benefits of laser irradiation upon measured parameters of wound healing. However, infrared wavelengths (700–1000 nm) were also investigated in 17 studies, either in isolation (n = 9), or as comparison with visible red wavelengths (n = 8). Despite the preference for use of red wavelengths in wound healing (in experimental and clinical studies, and in clinical practice), results in studies using infrared wavelengths consistently demonstrated laser-stimulated acceleration in wound healing. However, in two of these, 29,42 the use of higher dosages produced reduced stimulation 42 or even inhibitory effects. 29 Those studies which compared the effects of irradiation with red and infrared wavelengths (n = 8) reported a variety of results. One study found irradiation with 820 nm to be superior to treatment with 635, 670 or 720 nm laser light; 27 another reported best results with 633 nm irradiation. 44 Three studies indicated that best results were found with irradiation using 660 nm in the early stages of wound healing, whereas 780 nm treatment produced consistently positive results throughout all stages of wound healing. 62,63,73 Finally, Mendez and colleagues reported simultaneous irradiation with 638 and 830 nm light produced better outcomes than the use of either wavelength in isolation. 54
Power
Radiant power output (usually specified in mW for laser therapy applications) was reported in the majority of reviewed studies (39/47). With the exception of one study, 29 these ranged from 1–220 mW, with reported use of higher outputs typically associated with the use of longer wavelengths in the infrared range. 29,30,44 Kawalec et al., 29 in a study of diabetic-impaired healing in the mouse, employed a high powered laser source (5–10 W; 5000–10,000 mW), which was applied for one second to deliver dosages of 5 J and 10 J. Apart from this study, the average power output in the studies reviewed here was 30 and 35 mW (for mouse and rat studies, respectively). Despite the wide range of radiant power outputs employed in the studies reviewed, there was no clear association between reported outcomes and power levels employed. In those studies where different power outputs were employed, e.g., 43,44 it was not possible (despite authors' conclusions to the contrary) to attribute superior benefits to one particular power level, given the lack of standardization of other parameters, e.g., total dosage. 29,32 Equally, lack of standardization of power output confounds those reports of superior benefits of one wavelength over another. 44 Another issue of concern is that few of the authors of reviewed papers indicated whether power outputs were measured or checked on a regular basis during the period of the study.
Power density (irradiance)
Despite of the fact that power density (irradiance) represents an important parameter (essentially the intensity of the treatment, specified in mWcm2), it was specified as a parameter in less than a third (14/47) of the reviewed studies, and generally in those in which radiant power output was not specified. Irradiance could be derived from specified parameters (i.e., power output and area of irradiation) only in a further six of the reviewed studies; this is of equal concern, and underscores the lack of inclusion of key parameters in many studies. Excepting two papers from one group which employed irradiance levels of 1 Wcm2 (i.e., 1000 mWcm2), 62,63 where irradiance was reported or could be calculated, it ranged widely from 0.59 to 308 mWcm2, with an average irradiance of 56 mWcm2 across all studies (in mouse studies, 92 mWcm2). In those studies which compared differing irradiance levels, better effects were reported at the higher irradiance levels investigated, although values for irradiance varied significantly (670 nm/40 mWcm2; 24 670 nm/40 mWcm2 and 8 mWcm2; 30 635 nm/15 mWcm2; 33 632.8 nm/281 mWcm−2 32).
Time of irradiation
Combined with power or irradiance, the time of irradiation is an important determinant of dosage: dosage specified in energy (Joules; J) is calculated by multiplying power output (W) by time (s); when specified as radiant exposure (Jcm2) it is calculated by multiplying irradiance (mWcm2) by time (s). Thus, for a fixed power output or irradiance, time of irradiation is the primary means of adjusting or determining the dosage provided, and indeed is often used clinically as a shorthand for dosage (i.e., ‘… a 30 second treatment …’). Irradiation time (usually reported in s) was reported in 29 out of 47 reviewed studies, and could be calculated in a further six studies. One study stated that irradiation time was automatically adjusted according to power, but did not report specific time parameters. 64 Where this was specified, irradiation times ranged from 1–7,000 s (i.e., 1 h and 56 min); the average time of irradiation (based upon the longest time used in each experiment) was 766 s (approximately 13 min). The use of longer irradiation times would appear impracticable, and raise concerns regarding animal welfare (e.g., in terms of physical restraints or requirements for anaesthesia over protracted periods). A number of studies employed multiple irradiation times, either as a means of reciprocity (with different power/irradiance settings) to provide fixed dosages, 27,24,30 or, more simply, as a means to vary dosage for fixed power. 43,60,30,42,44,59,60,64,66,67
Spot size/area of irradiation
For 29 of the reviewed studies, spot sizes or areas of irradiation were reported or could be calculated (e.g., from specified diameter). Such areas ranged widely from 0.7 to 900 mm2 (median 100 mm2 or 1 cm2), and included arbitrary or assumed values in some cases, e.g., based on the wound area rather than the area of irradiation. This is concerning, given the importance of accurate specification of area of irradiation for calculation of irradiance and energy density.
Energy
Energy, specified in Joules (J) is one means of specifying dosage in laser treatments; as indicated above, it is calculated by multiplying the radiant output of the system (expressed in W) by the time in seconds. Given that most laser therapy systems employ sources operating in the mW range, this must be taken into account when calculating energy. Energy can be specified per point of application, but aggregated values are also sometimes used by authors: e.g., Pessoa et al. 74 reported dosage per point (0.33 J) and total Joules per treatment (2.97 J).
Only three of the reviewed studies reported dosage in terms of energy delivered (J), one of these apparently incorrectly. 69 Energy could be calculated for 28 of the remaining studies (i.e., 28/44), based on the available data; lack of essential data precluded calculation of this parameter in the remaining studies (n = 16). Dosage in Joules in those studies for which this parameter was provided or could be calculated ranged from 0.1 to 270 J, with a median total energy of 2.4 J per treatment (mean 13.6 J).
Energy density
Energy density (or, more accurately, radiant exposure, measured in Jcm2), is generally regarded as the gold standard for reporting of laser therapy dosage in research papers. However, its calculation can be subject to several sources of error, particularly in relation to spot size or area of irradiation, where relatively small discrepancies in measurement or estimation can give rise to significant errors in energy density.
With two exceptions, 35,39 energy density values were reported in all of the reviewed studies. These varied widely, from 1 to 50 Jcm2. However, based upon details provided for other parameters (i.e., power or irradiance, spot size or area of irradiation, and time of irradiation), there appeared to be widespread errors in reporting this parameter (n = 14 or approximately 30% of studies). Re-calculated values for radiant exposure ranged from 0.1 to 100 Jcm2, with a median value of 4.2 Jcm2 (mean 14.45 Jcm2). A number of studies found evidence of dosage response relationships, 29,32,42 –44, 48,54,58 –60,66,68,70 however, such evidence was fragmentary and – given the lack of standardization of other parameters and the wide range of dosages used – difficult to compare between studies. Demidova-Rice et al. 27 found a biphasic relationship, with positive effects at 2 Jcm2, and inhibitory effects at 50 Jcm2. In contrast, Yasukawa et al. 32 found best effects in terms of rupture strength at 4.2 Jcm2 (with an irradiance 281 mWcm2) compared to 2.09 Jcm2 (139 mWcm2). Kawalec et al. 29 compared two dosage levels (recalculated at 55 and 100 Jcm2) and similarly found that the higher dosage level produced inhibitory effects. This finding may have limited generalizability, however, given the lack of standardization of power levels, and the relatively high power outputs used (5 and 10 W). Indeed, this finding may be important in highlighting the inhibitory effects of higher power levels, rather than dosage per se.
Wound healing outcomes
A number of wound healing indices were measured using various techniques, most commonly histology. Only 18 of the 47 studies reported that measurement of outcomes was performed in a blinded fashion, although in another study microscopic analysis was made by two previously calibrated observers and confirmed by a pathologist. Further details of wound healing outcomes are provided in Tables 2 –8 in the columns headed: Wound outcomes measured.
Discussion
Experimental studies on the effects of laser irradiation on wound healing in animal models provide an ideal means to investigate efficacy and safety, and should represent an important prerequisite to trials in humans (and, eventually, to widespread application in the clinical setting to treat wounds). Furthermore, such models provide a means to test different sets of laser parameters in different animal models and types of wounds to determine an optimal constellation set. The most important finding from the current review is in relation to the effectiveness of laser therapy as a treatment for wounds: the studies reviewed here consistently demonstrate the ability of laser or monochromatic light to photobiomodulate (most commonly photobiostimulate) wound healing processes in experimental wounds in the rat and mouse, at least when applied at appropriate irradiation parameters. While species differences preclude direct extrapolation to clinical applications in humans, the current results strongly support the case for further controlled research in humans and the putative relevance of irradiation parameters such as dosage and irradiance.
This review also highlights a number of important issues relating to the quality of the study designs and protocols used, the types of wound healing models used (particularly in terms of the appropriateness of these to clinical applications in humans), and the relevance of irradiation parameters. These have already been indicated above and are considered further below. Systematic reviews have principally developed as a means of integrating evidence from randomized controlled trials to assess the clinical effectiveness of a given intervention. Although the principles underpinning systematic reviews of randomized controlled trials apply equally to experimental studies, to date there have been relatively few such reviews of basic science. 75 A key aspect of systematic reviews of clinical evidence is assessment of the quality (internal validity) of reviewed studies, using accepted rating scales. While such scales have yet to be developed and formally agreed upon for the assessment of internal validity in experimental studies, assessment of the quality of studies reviewed here has been informed by consideration of the items typically included in scales for randomized controlled clinical studies. 75
Research design and reporting of studies
There are two salient issues which limit comparison between studies, replication of reported benefits, and the formulation of recommended parameters for further studies in animals and in humans. These are the lack of specification of key details in many of the reviewed studies (including age and weight of animals, irradiation parameters etc.), and the wide variety in experimental methods used (including marked variations in ages and weights of animals studies, investigation of different types of wound models, including acute and impaired models of wound healing, and range of irradiation parameters used).
Apart from inadequate reporting of important elements of research design, and errors in calculation of laser irradiation parameters, there were several other prevalent weaknesses in the reviewed studies which may have led to bias in the reported findings. For example, blinding of investigators represents a key means of limiting researcher bias (whether witting or unwitting) in controlled studies. It is of concern that in so few of the studies were researchers blinded to group allocation, nor were measures taken to limit such bias (e.g., histology slides independently analyzed by two observers and confirmed by a pathologist). This is an important issue, and should be considered as an essential element of the research design of any future studies in this area.
Selection of control wounds for comparison with irradiated wounds is also a key issue in these types of studies. In the majority of reviewed studies, the wound healing outcomes of irradiated (treated) wounds were compared with those of non-irradiated (control) wounds, and sometimes this was done in the same individual animal, i.e., using each animal as its own control by creating multiple wounds. This clearly would have been very advantageous in terms of reducing animal numbers and the expense incurred in carrying out such studies. However given the possibility of influences of mediators from the primary wound affecting the healing of subsequent wounds (see below), the likelihood of concomitant irradiation of control wounds via light being reflected at the surface or scattered within the body tissue, and possible systemic effects of phototherapy treatment, it seems likely that this design cannot be justified without prior experimentation. This would require performing studies in animals where single wounds were made and carrying out measurements of the wound outcomes for irradiated and non-irradiated groups of animals.
Strains of animals
By far the larger number of studies have been performed in the rat, mostly using outbred strains such as Sprague-Dawley and Wistar, with very little use of inbred strains (for example Lewis and Brown Norway). This is in contrast to the relatively few studies carried out in the mouse, where more use has been made of inbred strains. Clearly, in terms of trying to develop guidelines which might result in a greater reproducibility between individual studies and reduce the numbers of animals used, the use of a small number of carefully chosen inbred strains would be beneficial. Strain differences have been reported in laser-mediated effects on wound healing in the mouse; 27 further studies are required with inbred strains of rats to determine whether a similar difference exists. This is an issue that needs to be considered further in future studies in this area.
Gender
Most of the studies found in the search only included male animals. However, it would seem important that studies should obtain data from sufficient numbers of both males and females to ascertain whether there are any differences in healing response between the two sexes. Very few of the reviewed articles provided any rationale for the selection of strains or sexes of animals. Possibly convenience and expense may play a role in selection, because male rats generally cost less than female rats of the same size. Also in females there may be a hormonal influence on wound healing, 76 and it was reported that the thinner skin of female rats allows a faster rate of wound healing with a higher rate of wound contraction compared to male rats. 77 Nevertheless, such underrepresentation of females in the studies reviewed here is of concern and should be addressed in future studies; in contrast, many national regulatory bodies now require inclusion of females in human clinical studies.
Age
The healing of wounds in older animals is much slower than that in younger animals; thus in comparing study findings, not only do the strain and sex have to be taken into account, but also the ages of the animals used. It is generally accepted that as animals age, they are less able to cope with environmental stress and more likely to suffer from concurrent multiple health problems, especially those that cause impaired blood supply to the skin and thereby compromise wound healing. 17
Wound healing model
Apart from models of acute wound healing, a range of models of impaired healing were investigated in reviewed studies. Notwithstanding the considerable body of positive findings in models of acute healing, the use of models of impaired wound healing, including models of diabetic-impaired healing, would appear more clinically relevant.
Although findings in diabetic-impaired healing were positive, in none of the rat studies with chemical-induced diabetes was the diabetes controlled by administration of insulin; this is an important issue, as uncontrolled diabetes can severely affect the wellbeing of the animals and compromise the study. 78 The latter is of relevance since findings in the BKS.Cg-m +/+ Leprdb/J strain may have been influenced by insulin levels or different levels of hyperglycemia. 26,29 Blood insulin peaks in these mice by 8–10 weeks of age and then falls precipitously to near normal levels concomitant with rising blood glucose concentrations. 79 –81 For future studies, it would be useful to be able to investigate effects of light therapy using wounds in animals with insulin-controlled diabetes.
Size, number and location of wounds
Considerable variation has been identified in the size, number and location of wounds made in individual animals. The larger size of the rat allows for the creation of up to four wounds on the dorsum, whereas in the mouse it is difficult to create more than two wounds on the dorsum. However, as indicated above, it is of concern that in creating multiple wounds, the healing of wounds made subsequently may be influenced by mediators (e.g., growth factors, cytokines) released from tissues injured when the primary wounds are created. Such mediators might exert their effects locally and/or systemically, and while separating the wounds might reduce the influence of a local effect, it may not completely eliminate it. Interleukin-6 (IL-6) activity is present in wound fluids and serum from wounded rats, and is released from wound cells in culture. 82 It appears that the early wound, and more specifically the polymorphonuclear leukocytes of the immediate inflammatory response, are the source of circulating IL-6 after injury. 82 Studies in human patients undergoing minor surgical procedures have demonstrated the appearance of significant levels of cytokines including IL-6, IL-8, and IL-10 in the blood circulation immediately post-surgery. 83 The regulated interactions of various mediators, including growth factors and cytokines, are important in controlling the series of events that lead to normal tissue repair. 84
Apart from such influences between wounds, the effects of phototherapy are not limited to the site of application, since through biological mediators the effect can be carried to other parts of the body by diffusion or systemically. 85,86
The most satisfactory model for such investigations would be a single wound created on one of the flanks of the experimental animal. In the reviewed studies only 34 out of 47 created a single wound. The mouse is ideally suited to this and would provide a much more cost-effective animal model than the rat.
Wound covering
One of the main limitations for the majority of reviewed studies is that wounds were not reported to be covered, and therefore wound contraction would have been the main contributor to wound closure. Covering of the wounds with an occlusive dressing such as Tegaderm (3M) or Opsite (SmithNephew) keeps the wound moist and facilitates reepithelization of the wound, thus creating conditions similar to those in human wound healing. Beyond this, in laser irradiated wounds, a thin transparent wound dressing such as Tegaderm enables the tip of the laser probe to be held gently in contact with the wound, thereby maximizing irradiance while preventing contamination of the wound. Covering a wound with an occlusive dressing such as Tegaderm or Opsite also prevents the invasion of microorganisms. 87 Thus, covered wounds would appear to be more suitable as a model for investigation of the photobiomodulatory effects of laser and phototherapy in wound healing. The very small number of studies in which wounds were reported to be covered in mice and rats is likely to be related to the difficulty in keeping the wound dressings attached. This is much more easily achieved with diabetic mice, 88 and is probably due to body shape and the larger surface area of skin.
Laser parameters
Laser parameters used in reviewed studies varied enormously, confounding direct comparison between studies and establishment of optimal irradiation parameters for the treatment of wounds, e.g., recommended dosages for wound healing. The optimal dose for wound healing with He-Ne lasers was first suggested to be 1–2 Jcm2 based upon work by Mester et al. 89 but indicated in later work to be 4 J cm2. 90 From current findings, this would appear reasonable, given the median dosage of 4.2 Jcm2 (based on re-calculated values for radiant exposure); however it is important to note that dosages employed ranged from 0.1 to 100 Jcm2, with positive findings reported across the entire dosage spectrum. Furthermore, many studies reported dose-response relationships, with inhibitory effects at higher radiant exposures in some cases, apparently confirming the proposed Arndt-Schultz phenomenon. 1,72
Apart from consideration of dosages, evidence from the current review would suggest the biomodulatory potential of a wide range of irradiation parameters: e.g., positive effects were reported using wavelengths ranging from the visible red to infrared, power and irradiance values from less than a fraction of a milliWatt to the Watt range, and irradiation times from seconds to hours. Notwithstanding the impracticalities associated with the use of such longer irradiation times, this also raises concerns in terms of animal welfare (e.g., in terms of physical or chemical restraints), and it would appear more ethical to reduce the stress to experimental animals by limiting the irradiation time where practicable. Perhaps one of the most interesting findings from this review in terms of irradiation parameters is the apparently equivalent effectiveness of coherent and non-coherent light sources, not least given the ongoing debate about the relevance of coherence to biological and clinical effects of phototherapy.
Beyond this, it is important to highlight the prevalent issue of errors in, or lack of, reporting of laser irradiation parameters in the studies reviewed here. It is essential to the future development of this area that authors should be required to report laser irradiation parameters in detail (including wavelength(s), power and irradiance, dosage in energy, and radiant exposure, as well as sufficient information to allow readers to have confidence in the provenance of cited parameters (e.g., time for calculation of energy; spot size or area of irradiation for calculation of irradiance or radiant exposure). This is an issue for journal editors and reviewers, as well as for authors.
Conclusion and Summary
This literature review identified 47 relevant studies in the mouse (n = 8) and in the rat (n = 39). Findings from these consistently demonstrated the ability of laser or monochromatic light therapy to photobiomodulate (typically stimulate) wound healing processes in experimental wounds in the rat and mouse, and strongly support the case for further controlled research in humans.
A variety of wound models were investigated in the reviewed studies, including acute, chronic and impaired wound healing models. There was considerable variation in research design, methodology, and laser irradiation parameters, which limited comparison of research findings between studies. Inadequate reporting of key details was also prevalent, as well as errors in specification or calculation of key irradiation parameters. These issues need to be considered in designing future research in this area.
Footnotes
Acknowledgments
We would like to thank Brigid Ryan for her helpful comments on the manuscript.
Author Disclosure Statement
No financial support has been received in conjunction with the generation of this report. No competing financial interests exist.