
Abstract
Introduction
Low-level laser therapy (LLLT) as a therapeutic modality was introduced by the work of Andre Mester and his colleagues, who described improvement in wound healing with the application of a low-energy (1 J/cm2) ruby laser. 4,5 Cameron and colleagues reported that the frequency of the laser light, as well as the type of tissue being irradiated, determines the depth to which light penetrates. Laser produced by a gallium aluminum arsenide (GaAlAs) laser penetrates deeper, whereas laser light with shorter wavelength, such as the red light produced by a He–Ne laser, penetrates less deeply. 6 A review of the literature revealed that LLLT with pulsed GaAlAs lasers increased higher fibroblast count than in control in vitro; 7 –9 increased collagen deposition, greater proliferation of myofibroblast 10 and acceleration of wound closure 11 in experimental cutaneous wounds; and increased the healing of human crural wound 12 and human superficial wound. 13
The benefits of continuous diode lasers in wound healing are controversial. Although a few studies have reported positive effects for continuous delivery of diode laser on the cutaneous wound-healing process, 14 –16 many other authors have found no improvement in this process using continuous diode lasers. 17 –22 Because of these contradictory results, there is still no consensus on the effects of LLLT in the wound-healing process. Recent studies have used various diode lasers with different wavelength, laser power, and stimulus dose. Regarding the type of laser and sufficiency of wavelength, no clear recommendations have yet been made.
On the other hand, a low-level pulsed-diode GaAlAs laser with a wavelength of 780 nm has not been examined in the wound-healing process. Recent investigations have not studied wound healing using a 780-nm pulsed-diode GaAlAs laser with a 2336-Hz frequency. Therefore, the aim of the present study was to examine the influence of a pulsed-diode GaAlAs laser with a wavelength of 780 nm and a 2336-Hz frequency on the healing of a full-thickness skin wound in rats.
Materials and Methods
Animals
Thirty adult male Sprague–Dawley rats (220 ± 30 g) housed in individual clean cages were fed a standard diet and tap water ad libitum. All procedures were approved by the Institutional Medical Ethics Committee. The animals were randomly divided into a sham-exposed group (n = 15) and an experimental group (n = 15).
Surgery
On day 0, all rats were anesthetized by 50 mg/kg ketamine hydrochloride injected intramuscularly along with 5 mg/kg diazepam. The dorsal hair of the rats was shaved and cleaned with povidone–iodine. Under sterile conditions, one round, full-thickness skin defect of about 20-mm diameter was produced on the dorsal neck of the animals with a #15 surgical blade. The wounds were left open without dressing. The animals were allowed to walk and move freely in their individual cages.
LLLT
The rats in the experimental group were exposed daily to a low-level laser (Endolaser 465, ENRAF NONIUS, Rotterdam, Netherlands). The specifications of this laser are given in Table 1. There were no methodological differences between experimental and sham-exposed groups except for the use of LLLT.
To administer laser irradiation, the wound area and surrounding normal skin were divided into equal squares (1 cm by 1 cm) and the tip of the laser was placed about 1 mm above the surface of the center of each square, directing it perpendicularly to the target tissue for 57 s. 23 The rats in each group were divided into three equal subgroups (A, n = 5; B, n = 5; and C, n = 5). The rats of groups A, B, and C were sacrificed after 4, 7, and 15 days, respectively.
Histological examination
The first sample for histological examination was excised from the wound bed and normal adjacent skin, fixed in formaldehyde saline, and embedded in a paraffin block. Sagital sections were cut and stained with hematoxyline and eosin. In order to count the fibroblasts, neutrophils, macrophages, endothelium of blood vessels, and blood vessel sections of the wound bed, eight zones from the slide were examined morphometrically through a calibrated ocular (MIC 0078-19) scale with 400 squares (EUROMEX Microscope, Arnhem, Holland) on a Nikon light microscope (Nikon, Tokyo, Japan) at a magnification of 400X. The above-mentioned eyepiece was used to calculate the thickness of newly regenerated epidermis. 24 Using 400 magnifications on the light microscope, the thickness of five different points of regenerated epidermis lying at equal distances from each other was measured, and the mean value was divided by 400. 24 Histological examination was performed in a blind fashion and in accordance with a procedure reported by Young and Dyson, 25 albeit with some modifications.
Biomechanical examinations
After each animal had been killed, the skin with wound was removed. A standardized 5-mm-wide skin strip was cut across the wound using a double-blade cutting instrument. The specimens were then placed in 0.9% saline. Biomechanical examinations were begun within 1 h postnecropsy. One specimen from each wound was obtained. The specimens were mounted in a material testing machine (Zwick 1494, Universal Testing Machine, Ulm, Germany) using two clamps with a rough surface, with the wound in the middle of the free surface. The jaw space, that is, the distance between the edges of the clamps, was 5 mm. Keeping the deformation rate constant at 15 mm/min, the specimens were loaded uniaxially so that failure and complete load–deformation curves could be recorded by transducers coupled to bridges and sampled in a personal computer by an analog-to-digital converter (PC–Software 27005). From the load–deformation curve, the following biomechanical properties were automatically calculated: (1) Maximum stress (g/mm2). At first, maximum load was measured directly from the load–deformation curve, which represents the maximum tensile strength force applied to a rupture specimen. (2) Maximum stress (g/mm2): The maximum load per unit cross-sectional area of the specimen. (3) Young's modulus of elasticity (N/mm2): the maximum slope on the linear portion of the stress–strain curve. 26,27
After analysis by the Mann–Whitney U-test, the data were presented as mean ± SD. A probability (p) of <0.05 was considered significant.
Results
The results obtained on the basis of morphometrical and biomechanical examinations are shown in Figs. 1 through 8.
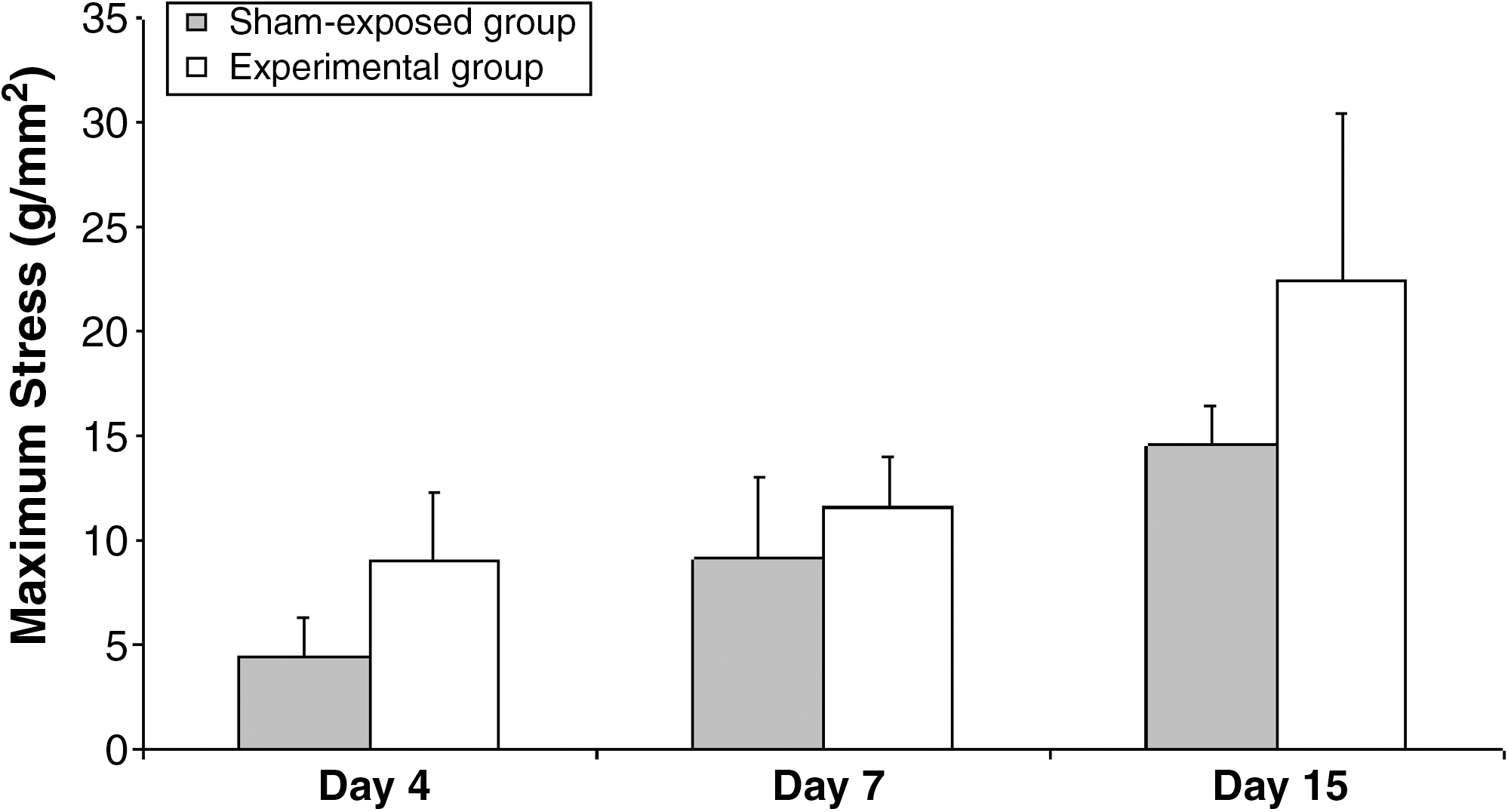
Mean ± SD of maximum stress (g/mm2) of study groups at sequential intervals. Mann–Whitney U-test showed significant differences between sham-exposed and experimental groups on days 4 and 15 (p < 0.01 and p < 0.05, respectively).

Mean ± SD of Young's modulus (g/mm2) of study groups at sequential intervals. Mann–Whitney U-test showed no significant differences between sham-exposed and experimental groups.
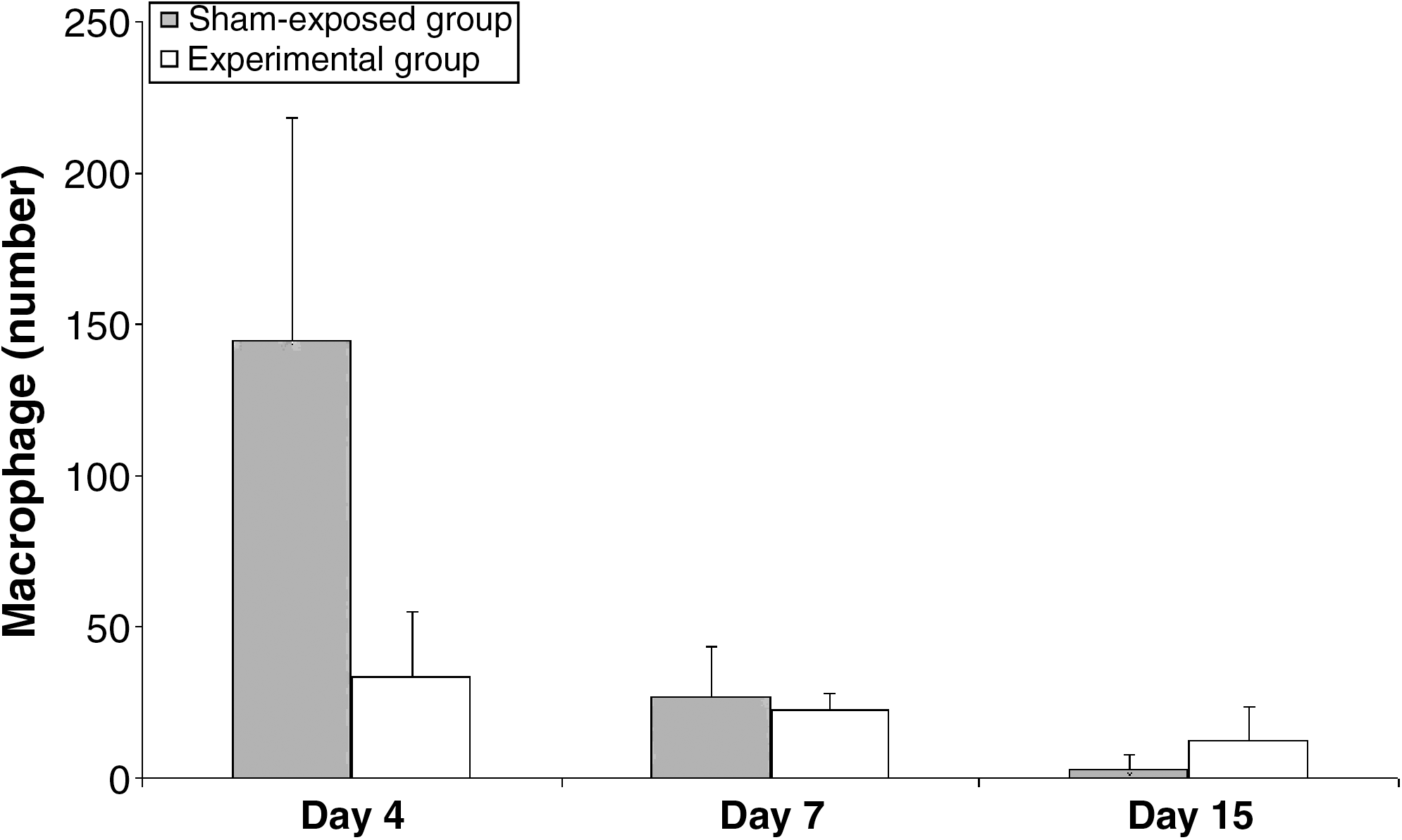
Mean ± SD of macrophages of study groups at sequential intervals. Mann–Whitney U-test showed significant differences between sham-exposed and experimental groups on day 4 (p < 0.01).

Mean ± SD of neutrophils of study groups at sequential intervals. Mann–Whitney U-test showed no significant differences between sham-exposed and experimental groups.

Mean ± SD of fibroblasts of study groups at sequential intervals. Mann–Whitney U-test showed significant differences between sham-exposed and experimental groups on days 7 and 15 (p < 0.05, p < 0.01, respectively).
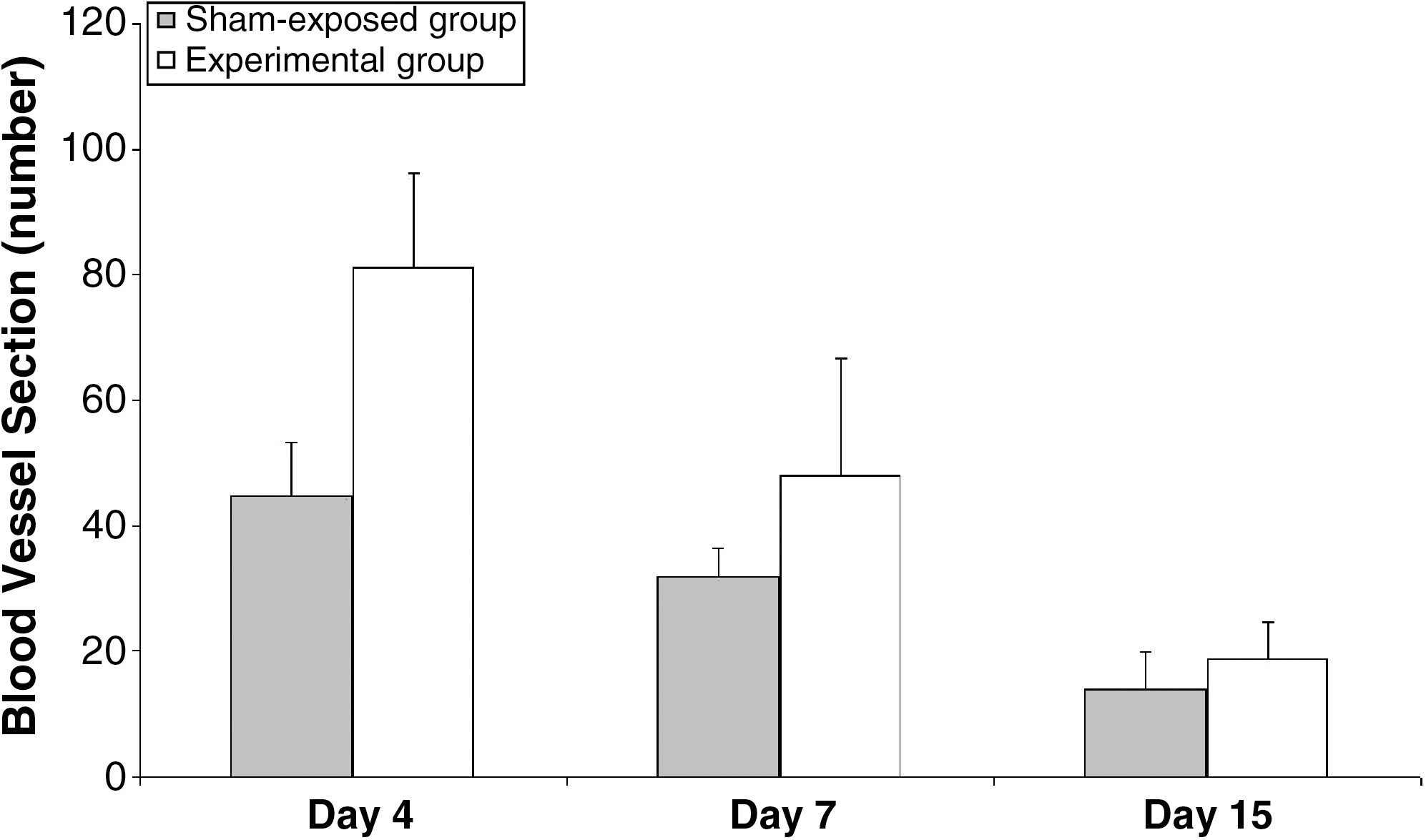
Mean ± SD of blood vessel sections of study groups at sequential intervals. Mann–Whitney U-test showed significant differences between sham-exposed and experimental groups on day 7 (p < 0.05).
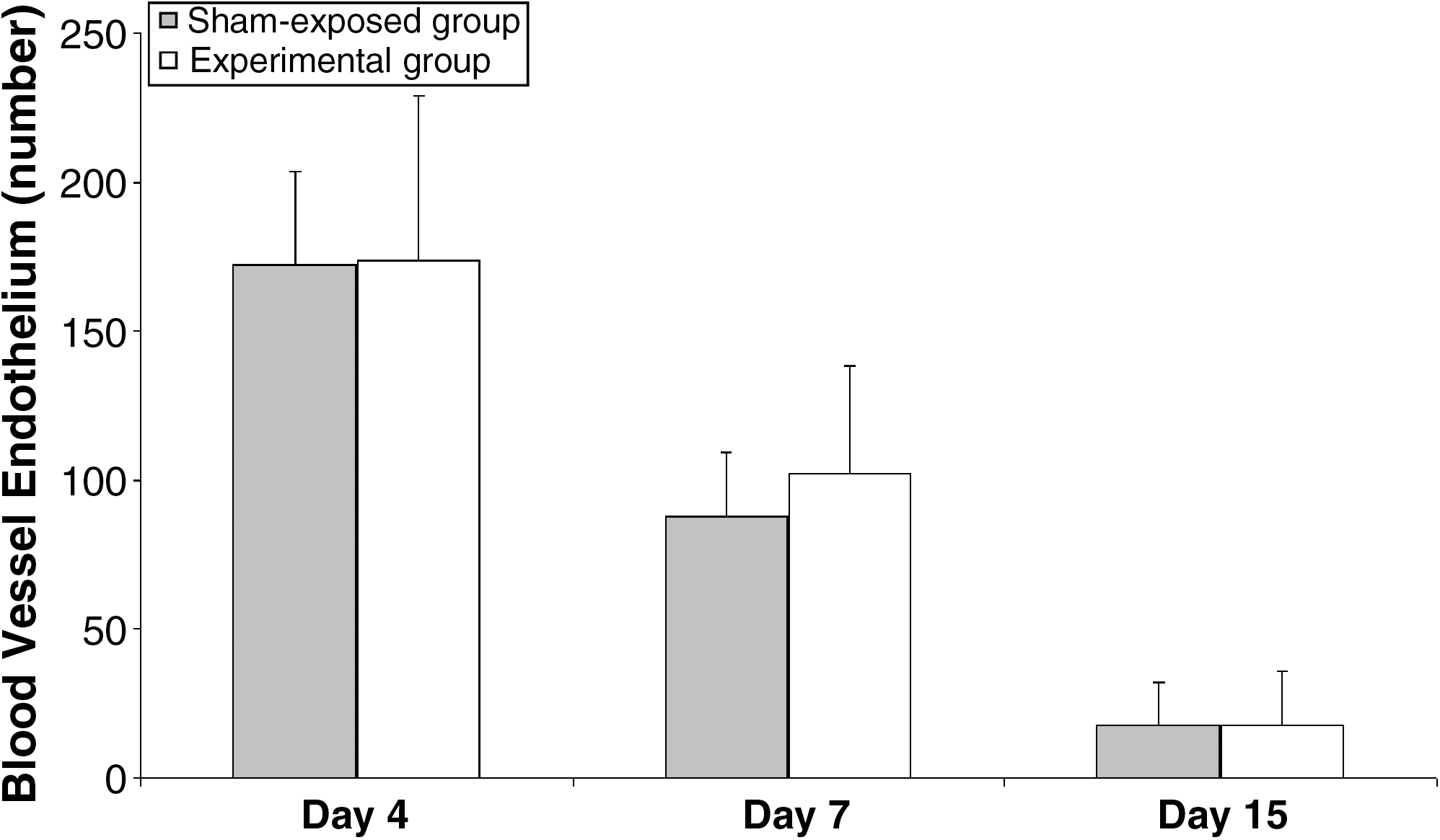
Mean ± SD of blood vessel endothelium of study groups at sequential intervals. Mann–Whitney U-test showed significant differences between sham-exposed and experimental groups on day 15 (p < 0.05).
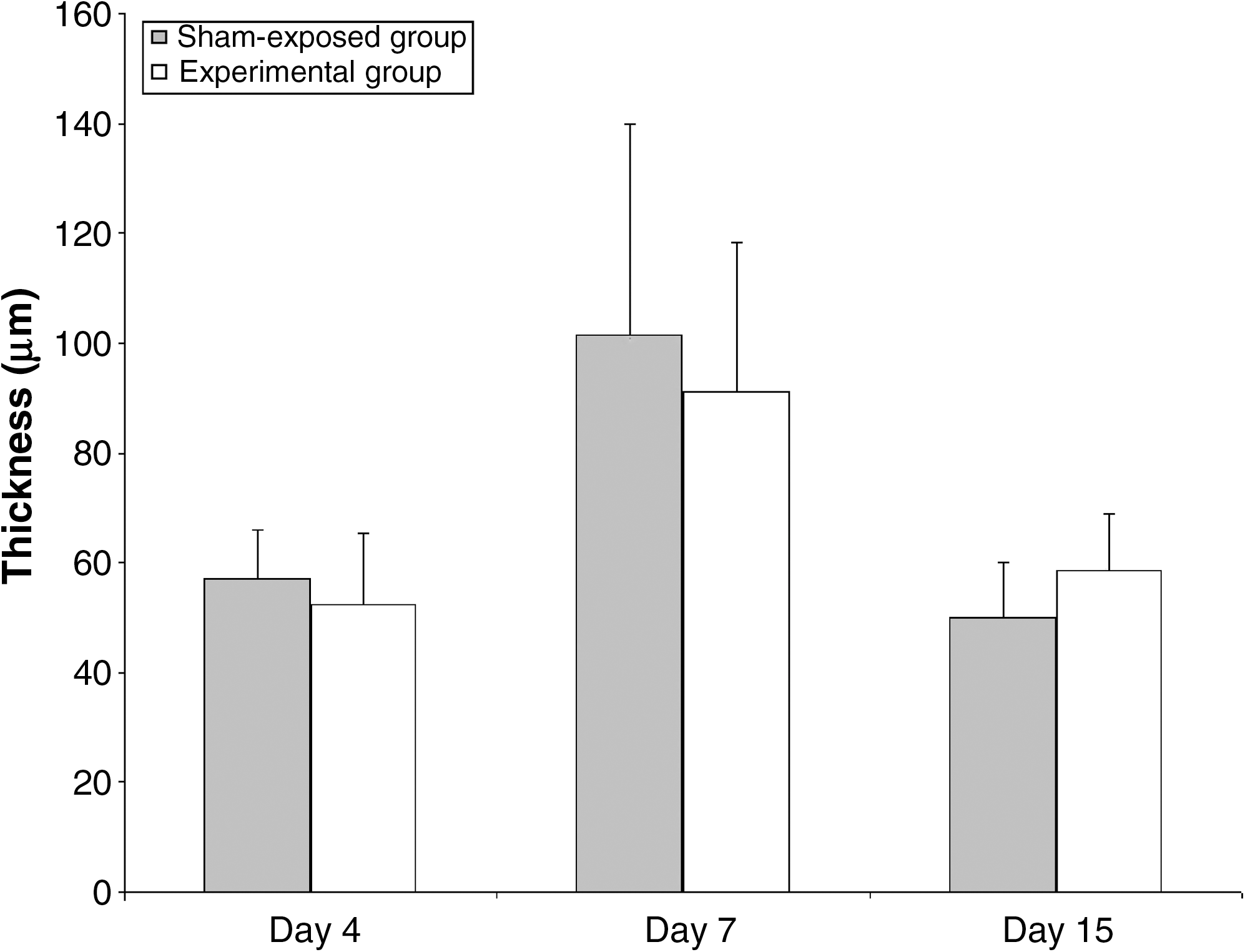
Mean ± SD of thickness of newly regenerated epidermis (μm) of study groups at sequential intervals. Mann–Whitney U-test showed no significant differences between sham-exposed and experimental groups.
Day 4 after surgery
The mean value of maximum stress (g/mm2) in the experimental group (9.01 ± 3.375) was significantly higher than that of the sham-exposed group (4.50 ± 1.756) (p < 0.01). The mean number of macrophages of the experimental group (33.4 ± 21.5) was significantly lower than that of the sham-exposed group (144.7 ± 73.4) (p = 0 < 0.1).
Day 7 after surgery
The mean numbers of fibroblast (1080.6 ± 130) and blood vessel sections (48 ± 18.7) in the experimental group were significantly higher than those of the sham-exposed group (fibroblast, 952.5 ± 88.8; blood vessel sections, 32 ± 4.5; both p < 0.05).
Day 15 after surgery
The mean numbers of fibroblasts (1225.3 ± 180.2), endothelium of blood vessels (60.5 ± 17.9), and maximum stress (22.4 ± 8.01) in the experimental group were significantly higher than those of the sham-exposed group: (fibroblast, 914.4 ± 106; endothelium of blood vessels, 37.7 ± 17.9; maximum stress, 14.55 ± 1.93; all p < 0.01).
Discussion
Because of the different results from studies using continuous diode lasers on skin wounds, 14 –22 the current study investigated the effect of the pulsed-frequency mode of diode laser on skin wound healing.
The biostimulatory effect of pulsed LLLT in the present study is demonstrated by significant increases in fibroblasts, endothelium of blood vessels, blood vessel sections, and maximum stress compared with those of the sham–exposed group. However, the effectiveness of pulsed LLLT with various wavelengths, pulse frequencies, and energy densities on wound healing has not been fully clarified. A review of the available literature indicates that no studies regarding the positive effect of the pulsed mode of LLLT on the delayed and impaired wound-healing process have been carried out. 28 –30 Recently, Lagan and colleagues investigated the influence of a pulsed LLLT on the healing of chronic venous ulcers in patients. 28 A multisource diode array (660–950 nm) was used for irradiation; parameters were kept constant for the duration of the study (532 mW, 5 kHz; 12 J/cm2). These authors reported that their findings provide only limited evidence for the use of pulsed LLLT as an adjunctive therapy with current nursing intervention. 28 Lowe and colleagues and Walker and colleagues also failed to show a positive effect for pulsed LLLT on the impaired wound-healing process. 29,30
Using a GaAlAs 890-nm multidiode (n = 60) array unit (270 Hz, maximum rated output 300 mW), Lowe and colleagues 29 examined wound healing in mice exposed to x-ray irradiation. They found that treatment with 890-nm light therapy did not have a significant effect on wound closure at doses of 0.18 and 0.54 J/cm2. Using a similar animal model of radiation, impaired wound healing in mice, Walker and colleagues 30 found no hastening of wound healing with a 660-nm GaAlAs laser (5 kHz, 15 mW, and 0.5, 1.5, and 4 J/cm2) for three groups. It seems that pulsed LLLT with the parameters used in the above-mentioned studies could not accelerate healing in impaired and delayed wounds of animal models and patients. 28 –30
Very recently, Matic and colleagues have reported LLLT that using an 830-nm wavelength of the semiconductor laser with a frequency of 1500 Hz, impulse duration of 300 ns, and medium strength of 15.4 mW produces a significant accelerated rate of wound closure of a rectangular acute wound of all skin layers. 11 Simunovic and colleagues 31 performed a clinical study on patients with musculoskeletal disorders. All patients had surgical procedure prior to LLLT. A He–Ne laser combined with a diode 904-nm pulsed wave for the scanning procedure was used. The results showed that the wound-healing process was significantly accelerated in the group of patients treated with LLLT. 31 It seems that the patients' wounds can be categorized as acute wounds. The results of the current study support the recent findings of the studies of Matic and colleagues 11 and Simunovic and colleeagues. 31
A biomechanical examination of the present study revealed that maximum stress of laser-treated wounds was significantly higher than that of the sham-exposed group on days 4 and 15. The biomechanical data indicate that the healed wounds receiving laser treatment were stronger (load) than for sham–exposed wounds. The ability of skin to stretch is especially important when it crosses a joint. 27 In the current study there was no significant difference in elasticity (Young's modulus) between the sham-exposed group and experimental group.
The biomechanical results of our study support that LLLT at 780 nm and an energy density of 2 J/cm2 is capable of enhancing collagen synthesis. Similarly, Stadler and colleagues, 32 using a continuous 830-nm low-power laser, and Demir and colleagues, 14 using a continuous 904-nm low-level GaAsAl laser, reported a higher tensile strength in laser-treated rats compared with relevant control groups. Thus it appears that LLLT accelerates some processes of wound healing and may enhance the factorylike roles of fibroblasts, including the production of permanent extra cellular matrix (ECM) (including collagen, glycosaminoglycan, and proteoglycan) and granulation tissue. It may also increase the process of procollagen aggregation into ECM and the strength of collagen fibers. In contrast, Allendorf and colleagues 33 suggested that He–Ne laser irradiation (4 J/cm2) has no beneficial effect on the tensile strength of wounds. The reason for this diversity may be the type of laser used.
In postnatal life the inflammatory response is one inevitable consequence of tissue injury. Experimental studies established the dogma that inflammation is essential to the creation of cutaneous homeostasis following injury, but in recent years information associated with tissue repair has increased. Recently, this dogma has been challenged, and reports have questioned the validity of the essential prerequisite of inflammation for efficient tissue repair. 34 Indeed, in experimental models of repair, inflammation has been shown to delay healing. 35,36 In the present study the mean number of macrophages at the inflammation phase of wound healing in the experimental group was lower than that of the control group 4 days after surgery. The current results confirm the findings of others. Medrado and colleagues 10 reported that in laser-treated animals the extent of edema and the number of inflammatory cells were decreased. Demir and colleagues 14 showed a reduction in inflammatory cells in laser-treated wounds compared to control wounds. Histological examination of the present study showed that the number of fibroblasts in the experimental group was significantly higher than that of the sham-exposed group on day 7. The current information provides data that suggest pulsed LLLT at 780 nm and an energy density of 2 J/cm2 is capable of enhancing fibroblast proliferation in wounds of normal rat. Our results confirm the findings of others. Medrado and colleagues 10 and Demir and colleagues 14 reported a significant increase in fibroblast proliferation of the wound bed of laser-treated wounds 10 days after wounding. Similarly, Reis and colleagues, 37 using a GaAlAs laser (4 J/cm2, 9 mW, λ = 670 nm), showed a similar effect on fibroblast proliferation. The results of the present investigation are also in compliance with previous in vitro studies. 7 –9 However, not all studies support this beneficial effect. 28 –30 In a study on low-energy infrared and skin wound, Anneroth and colleagues 17 failed to demonstrate a difference in histological parameters between laser-treated and control wounds in rats. The reasons for this diversity may be variations in treatment time, area, and frequency; type of laser irradiation (pulse vs. continuous delivery); type of laser used; and the various skin structures in different animal species used in these studies. Neovascularization is a major constituent of every healing wound. Mature vessels in deeper tissue layers produce buds into the granulating wound to provide the wound area with sufficient blood supply. 38 The mean of blood vessel sections on day 7 and blood vessel sections in the experimental group of the present study significantly increased on day 7. The results of our study are in accordance with those of Medrado and colleagues. 10
The results of Demir and colleagues 14 and of the current study showed a significant increase of both fibroblasts in the experimental group and endothelium of blood vessels at the maturation phase of the wound-healing process. In this regard, Webb and Dyson reported that a photobiomodulatory effect of LLLT on hypertrophic scar healing is not required, 39 since excessive fibroplasia 7 is counterproductive in wounds that are susceptive to hypertrophic scarring. The dose of laser used was in the range of the energy densities of previous related studies. 4,5,7,9,10,14 A few studies have reported a positive effect of pulse frequency on surgically induced open skin wounds. So in the current study a 2336-Hz pulse frequency was chosen based on an author's pilot study.
It is concluded that LLLT with 780-nm GaAlAs laser significantly accelerates the healing of surgically induced full-thickness skin wounds in rat. It is suggested that further investigation of the LLLT on delayed wound healing be examined.
Footnotes
Acknowledgments
We wish to extend thanks to the late Mrs. Jamileh Rezaie. We also take this opportunity to thank the Academic Center for Education, Culture, and Research for financial support (grant no 101/1).
Author Disclosure Statement
No conflicting financial interests exist.