
Abstract
Introduction
Perhaps because of the multifactorial nature of the pathogenesis of tendinopathy, 5,6 there is a plethora of treatment modalities available to reduce symptoms and to attempt to control or enhance the tendon healing response. These modalities, which include various electrotherapy modalities, eccentric exercise, a variety of injection techniques, and cross-fiber massage, provide mixed or uneven benefit across patient populations. 7 –9
Low level laser therapy (LLLT) or the use of laser sources at powers too low to cause measurable temperature increases, has been used to treat soft tissue injuries and inflammation since the 1960s, and studies from as early as the 1980s reported benefits in a variety of tendon and sports injuries. 10,11 More recently, the term LLLT has been used to describe not only the use of low power laser sources, but also monochromatic superluminous diodes. Both types of system have been used in the treatment of various musculoskeletal conditions, including tendon injuries, each apparently with success. Such applications are supported by experimental evidence of the biological effects of LLLT, including increased ATP production, enhanced cell function, and increased protein synthesis. 12 LLLT has also been shown to have positive effects on the reduction of inflammation, 13 increase of collagen synthesis, 14 and angiogenesis. 15
While LLLT is promoted as a safe and effective form of treatment for a variety of conditions, in today's healthcare climate there is a necessity to practice evidence-based medicine, and a need to provide high level evidence to support the use of any treatment modality. Whether previous research into the effectiveness of LLLT has accomplished this is debatable due to the varying quality of the available research.
With this in mind, a systematic review with a meta-analysis of the data was undertaken to answer the question: “Is Low Level Laser Therapy effective in the treatment of tendinopathy?” Three main objectives were set: a) to determine the clinical effectiveness of LLLT in the treatment of tendinopathy when compared to placebo, no treatment, or other types of intervention; b) to determine the relevance of irradiation parameters to reported positive outcomes; c) to determine the validity of current dosage recommendations for the treatment of tendinopathy.
Materials and Methods
Search strategy
The MEDLINE (1966-1st Aug 2008), PubMed (1950-1st Aug 2008), CINAHL (1982-1st Aug 2008), AMED (1985-1st Aug 2008), EMBASE (1988-1st Aug 2008), All EBM (Evidence Based Medicine) reviews, PEDro (Physiotherapy Evidence Database), and SCOPUS (1960-1st Aug 2008) databases were searched (Table 1).
Selection criteria for this review: types of studies
Fully reported randomized controlled trials (RCTs) and controlled clinical trials (CCTs) from peer reviewed journals were included. No language restrictions were made.
Selection criteria for this review: types of participants
Human participants who had been diagnosed with tendinopathy and exhibited pain and/or functional disability were included. There was no distinction made with regards to age, gender, level of activity or chronicity of the injury.
Selection criteria for this review: types of interventions
One group in the controlled trial must have involved participants treated with active LLLT. Comparisons were made with at least one of the following: placebo, no treatment, or other treatments such as medication, exercise therapy or other electrotherapy modalities. Interventions based upon combinations of LLLT and other modalities were not considered for the review.
Selection criteria for this review: types of outcome measure
Trials which assessed pain or function for at least one of the outcome measures were considered for inclusion.
Retrieval of relevant articles
Two independent reviewers (ST and JM) applied the selection criteria to the titles and abstracts of articles retrieved by the electronic search. All trials classified as relevant by either of the reviewers were retrieved. When there was insufficient information in the title or abstract to determine eligibility, the full text of the article was retrieved. Where there was disagreement between the two reviewers about a trial's eligibility, the retrieved trial was re-examined against the selection criteria, and disagreement resolved by consensus. For studies published in languages other than English, a translation was obtained.
Quality assessment
Three independent reviewers (ST, SM & DH) assessed the included articles for methodological quality against the PEDro scale. 16
Data extraction
Three reviewers (ST, JB & GDB) independently extracted and recorded the necessary details about diagnosis, interventions, and LLLT parameters, in line with recommendations by the World Association for Laser Therapy (WALT) 17 to determine the parameters and method of delivery of laser therapy.
Analysis
The recommendations of Van Tulder et al. 18 regarding levels of evidence were used to interpret the results:
Strong evidence: consistent findings among multiple higher quality RCTs;
Moderate evidence: consistent findings among multiple lower quality RCTs and/or one higher quality RCT;
Limited evidence: one lower quality RCT;
Conflicting evidence: inconsistent findings among multiple RCTs;
No evidence: no RCTs.
Pooling of data
Where available, data were pooled as follows:
Pain: used a visual analogue scale (VAS) for both final scores and change in scores;
Site of injury: i.e., for lateral epicondylitis, Achilles tendinopathies, rotator cuff injuries; Grip strength.
To investigate the relevance of parameters to reported benefits, studies were also grouped into those reporting positive effects and those reporting inconclusive or no effects.
Statistical analysis
Where pooling of data was justified, results were expressed as relative risks (RR) and 95% confidence intervals (CI) for dichotomous outcomes, and weighted mean difference (WMD) and 95% confidence intervals calculated for continuous outcomes. Testing for heterogeneity was done using the chi-square test. Test results for heterogeneity determined whether a random or fixed effects model was used.
Disagreements between reviewers were settled by consensus. Where insufficient data was provided in the published article, every attempt was made to contact the authors to obtain the relevant information.
Results
The Quality of Reporting of Meta-Analysis (QUOROM) statement flow diagram 19 (Fig. 1) displays the results of the search conducted on 1st August 2008. As shown, 663 investigations were identified as being potentially relevant according to the initial search criteria. Of these, 638 reports were excluded at various stages of the process for a variety of reasons, including: they were review articles; they involved surgery or did not involve LLLT; they did not address tendinopathy; they included inappropriate LLLT intervention/application techniques; they were not an RCT/CCT; they were not full reports; or they did not appear in peer-reviewed journals. Twenty-five articles were included in the review (Table 2 and Table 3).
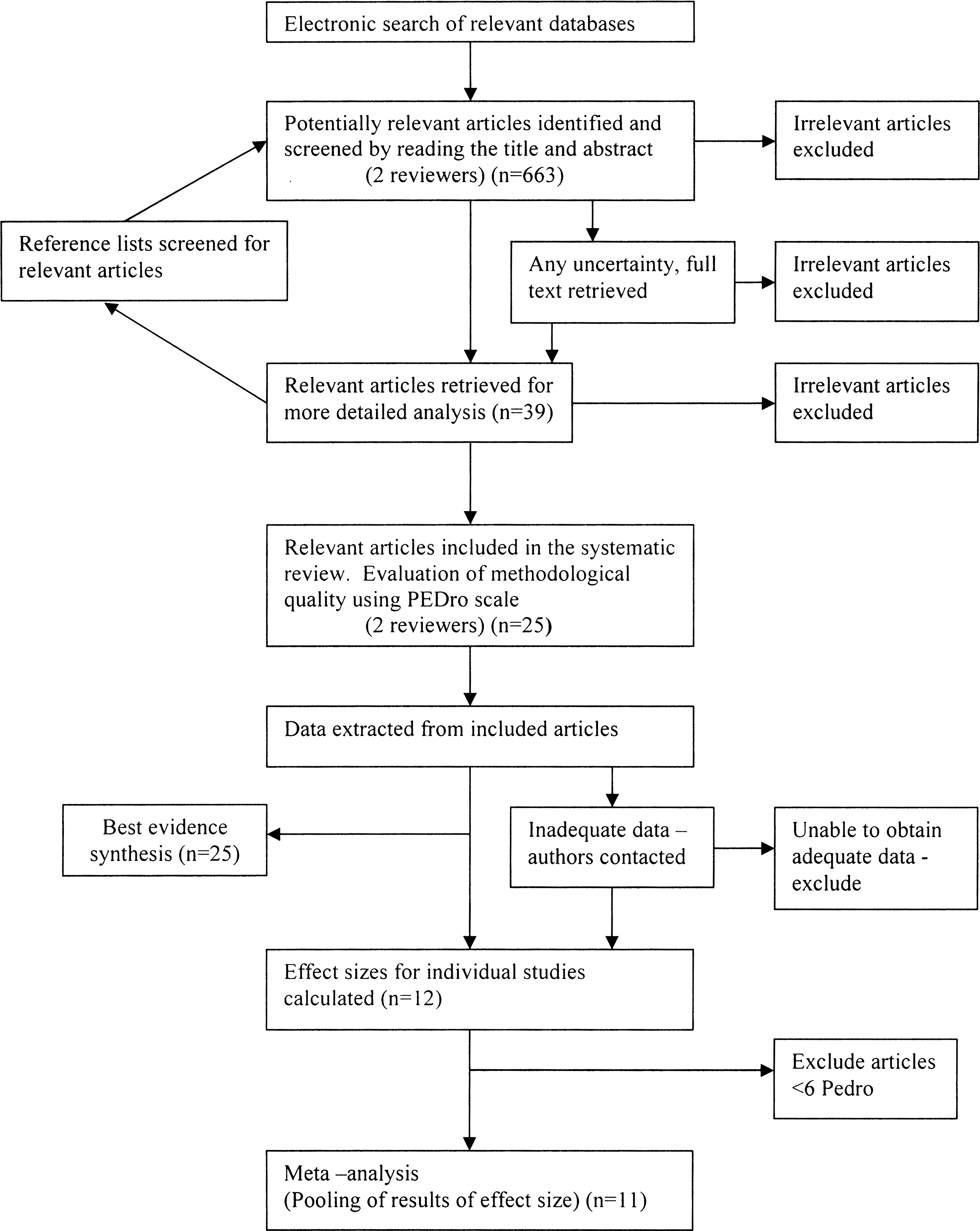
Search Strategy Flow Diagram Search strategy used to screen articles against the inclusion/exclusion criteria to generate the final list of articles for analysis.
1 - Eligibility criteria?
2 - Random allocation?
3 - Concealed allocation?
4 - Baseline comparability?
5 - Blind subjects?
6 - Blind therapists?
7 - Blind assessors?
8 - Adequate follow-up?
9 - Intention-to-treat analysis?
10 - Between-group comparisons?
11 - Point estimates and variability?
✓ = Criterion met; × = Criterion not met; ( ) = Eligibility criteria item does not contribute to total score.
Assessing the level of evidence for the effectiveness of LLLT in the treatment of tendinopathy based upon van Tulder's recommendations (see Table 3), 18 the evidence for the effectiveness of LLLT in the treatment of tendinopathy is inconclusive, as there are conflicting findings among multiple RCTs: twelve studies reported a positive effect (Table 4), and thirteen studies reported no effect or inconclusive results (Table 5).
Parameters not provided or insufficient information given to calculate missing parameter.
These studies are included in the RevMan analysis.
Parameters not provided or insufficient information given to calculate missing parameter.
These studies are included in the RevMan analysis.
Twelve studies provided sufficient detailed data to input into RevMan 4.2 (Cochrane Collaboration, Copenhagen, Denmark 20 ) to calculate effect sizes for the outcome measures of final pain scores and pain change scores measured on a VAS (Fig. 2), or, for lateral epicondylitis, grip strength (Fig. 3). These twelve studies are indicated by** in Tables 4 and 5.
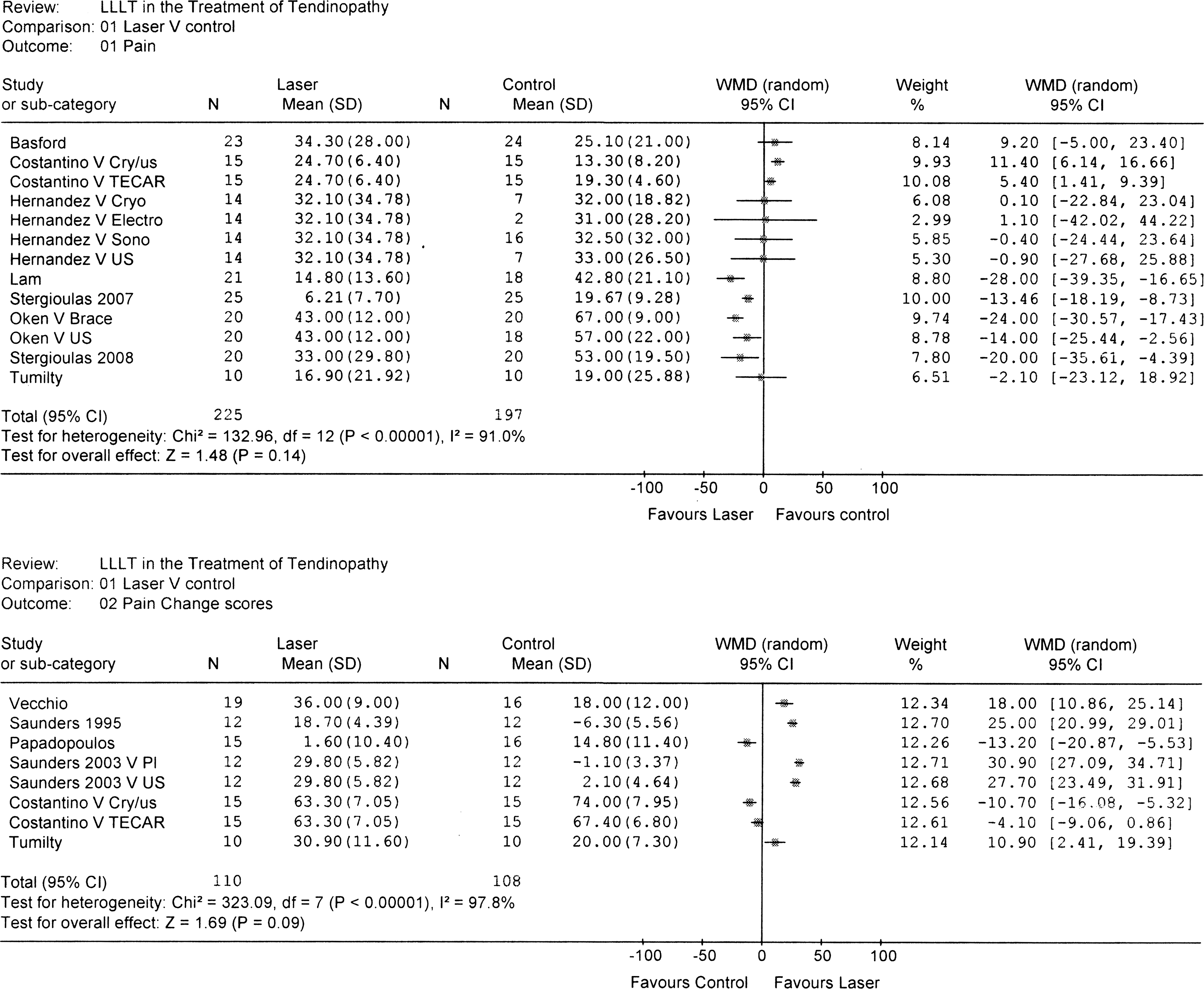
Pain analysis with all groups in all studies. When studies included more than two groups or an active control group, the non-laser treatments are shown after the author's name. US, ultrasound; Sono, sonophoresis; Electro, electrophoresis; Cryo, cryotherapy; Cryo/us cryoultrasound; TECAR, capacitive-resistive electric transfer therapy; Brace, tennis elbow brace; Pl, placebo.

Lateral epicondylitis grip strength. The upper graph includes both comparisons from Oken et al. 29 (2008) and therefore pooling of data is not shown.
Attempts to pool data from multiple studies were not valid as the test for heterogeneity was significant (p < 0.05) for most of the analyses. However, to show the effect of individual comparisons, for studies that compared LLLT against more than one other group, data comparing LLLT against all other modalities were included in the analysis (Fig. 2). For example, in a poorly powered study by Hernandez-Herrero et al. 24 in which LLLT was compared against four other modalities of treatment for elbow tendinosis, it can be seen that there was very little difference between LLLT and the other forms of treatment. Of the studies that showed a positive result of LLLT for pain, the effects ranged from 2.1-28 mm on a 100 mm VAS (Fig. 2).
It was valid to pool data in two instances: the first for participants' grip strength in studies of lateral epicondylitis that scored ≥6 on the PEDro scale (Fig. 3); in the second instance, for pain scores in Achilles tendinopathy (Fig. 4). Effect sizes corresponded to grip strength values of 9.59 kg greater than the control group for participants with lateral epicondylitis, and 13.6 mm less pain on a 100 mm VAS for participants with Achilles tendinopathy.
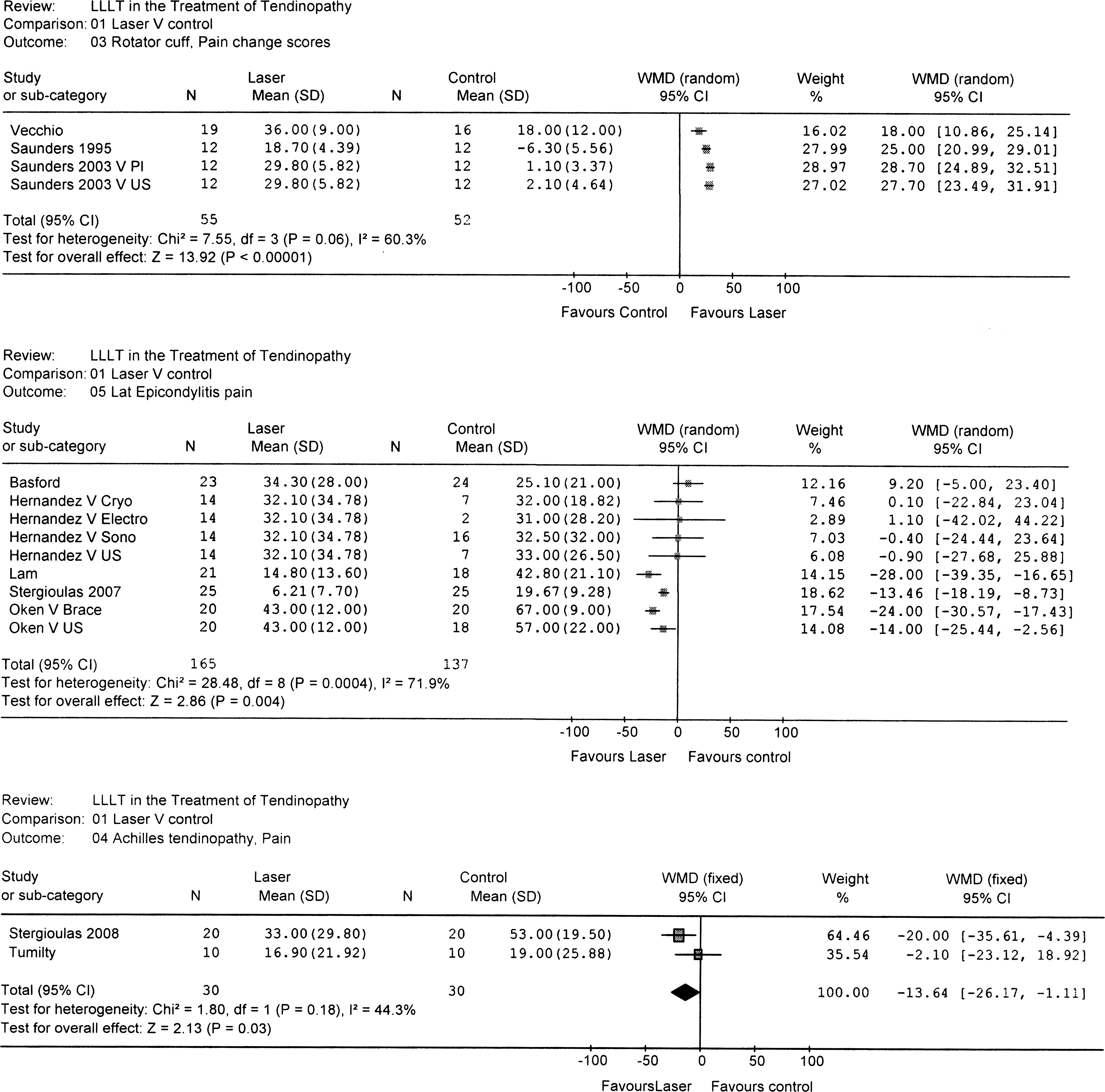
Low Level Laser Therapy Effects on Pain Scores Categorized by Site of Injury. Pooling of data was only valid for Achilles Tendinopathy Pain. When studies included more than two groups or an active control group, the non-laser treatments are shown after the author's name. US, ultrasound; Sono, sonophoresis; Electro, electrophoresis; Cryo, cryotherapy; Cryo/us cryoultrasound; TECAR, capacitive-resistive electric transfer therapy; Brace, tennis elbow brace; Pl, placebo.
Results for pain scores categorized by site of injury are displayed in Figure 4. Three studies reported pain change scores for rotator cuff injuries treated with LLLT. 35 –37 Of these, two compared LLLT to placebo, 35,37 while Saunders et al. 36 included three groups: LLLT, placebo, and ultrasound. Assessment by change in pain between initial and final assessments all showed a positive effect in favor of LLLT.
Of the two studies which investigated Achilles tendinopathy, 39,40 both showed positive effects in terms of pain scores at the final assessment, with a pooled effect size of 13.64 mm in favor of the LLLT groups.
Final pain scores were analyzed for participants with lateral epicondylitis. Figure 4 shows multiple comparisons from single studies, so that determination of a pooled effect size was not possible. Of the five studies, two showed no effect of LLLT on participants' pain, 21,24 and three resulted in a positive effect on pain. 27,29,31
Table 4 displays those studies reporting positive effects of LLLT, as concluded by the authors of the individual studies, along with the parameters used. Five studies (marked**) provided data that were used in the RevMan analysis. Table 5 displays studies reporting inconclusive results or no effect from LLLT. It should be noted that even though three studies 29,37,40 reported no significant differences between groups, in the RevMan analysis the effect sizes of these studies favored the group treated with laser.
Using the parameters reported in Table 4, a range of effective dosages can be calculated for each injury site. These can then be compared to the current recommendations from WALT 17 and from Bjordal et al. 45 (Table 6). These guidelines state that power densities below 100 mW/cm2 should be used for superficial tendons with an energy dose range of 1–8 J. For the deeper tendons of the rotator cuff, power densities are allowed to go as high as 600 mW/cm2, with an energy dose range of 3–9 J.
Epicondylitis
Of thirteen studies investigating the effectiveness of LLLT for epicondylitis, six showed positive results. 22,25,27,28,31,32 Ten out of the thirteen scored six points or more on the PEDro scale and would be considered of high quality. The positive studies used a wavelength of 904 nm and power densities that lay between 2–100 mW/cm2 as recommended by the WALT/Bjordal et al. guidelines. 13 However, one study 32 used a dosage slightly higher then the recommended value (3.5 J/cm2 instead of 3 J/cm2) while another 28 used a wavelength (1064 nm) and energy density (150 J/cm2) that do not appear in any of the guidelines. Those studies demonstrating no effect 21,23,24,26,29,30,33 all used power densities and dosage parameters outside of the guidelines, regardless of wavelength employed.
Rotator cuff
Four high quality studies examined the effects of LLLT on tendinopathy around the shoulder region, 34 –37 with three studies 35 –37 using parameters that lay within the guidelines (30–600 mW/cm2 & 4.2-42 J/cm2). However, these three provided conflicting results (two positive 35,36 and one negative 37 ). The study by England et al. 34 failed to provide enough detail on irradiation parameters.
Achilles tendinopathy
Four studies investigated LLLT for Achilles tendinopathy. 13,38 –40 Two proved beneficial, 13,39 and two were inconclusive. 38,40 The two positive studies used parameters that lay within recommended guidelines, 13,39 but the others did not. 38,40 One of the negative studies was deemed of low methodology (less than 6 on the PEDro scale). 38
De Quervain's tenosynovitis
One high quality study 44 used LLLT to treat tendinopathy at the wrist (Table 6); however, there are no recommended guidelines published for that condition. The parameters used are provided in the table.
Discussion
This systematic review and meta-analysis was designed to assess the evidence for the clinical effectiveness of LLLT for the treatment of tendinopathy, the currently accepted terminology used clinically to encompass tendonitis, tendinosis, and insertional tendinopathy. Its secondary objectives were to determine the relationship between irradiation parameters and outcomes and to compare them with the dosage recommendations provided by WALT 17 and from Bjordal et al. 45 The findings provided conflicting evidence regarding the effectiveness of LLLT for the treatment of tendinopathies. However, there was a clear relationship between positive findings and the use of recommended dosages.
Studies reporting benefits (n = 12) were similar in number to those that found no benefit (n = 13). These conflicting results did not appear to be due to methodological quality, however; the studies' methodological scores were generally good (6 or higher on the PEDro scale), with only two positive studies scoring low, 25,28 compared with three inconclusive studies. 24,38,43 Perhaps the most important finding of this review is that 12 RCTs (ten high quality and two low quality) demonstrate that LLLT is potentially effective in the treatment of tendinopathy when the recommended irradiation parameters are used.
This finding is perhaps not surprising as a dosage-dependent effect should not be unexpected for any effective therapeutic modality. Furthermore, as the body of research grows for a new modality and researchers seek to establish an effective dosage window, conflicting evidence would be expected to accumulate from an ever increasing number of studies; this is seen in the therapeutic ultrasound literature. 46,47 Under these circumstances, it becomes important to look at the available evidence using methods other than van Tulder's best evidence synthesis, which does not take into account the validity of the intervention used. 18
Twelve studies provided sufficient data to undertake a meta-analysis of effects. Unfortunately, given the variation in interventions used (including different manufacturers, devices, variations in delivery, and calculations of dosages) there was clinical heterogeneity between studies. This can result in misleading conclusions, as differences in treatment parameters and application are important, 48 and can lead in turn to statistical heterogeneity. Indeed, only two of the meta-analyses (the effect on Achilles tendon pain and the effect on grip strength for lateral epicondylitis) resulted in studies that were homogenous (see Figs. 2 –4) and thus allowed calculation of pooled effect results. Other meta-analyses resulted in statistical heterogeneity, thus limiting any conclusions from these data. 49 Given such clinical and statistical heterogeneity from the studies included in this review, we made no attempt to report these combined data.
However, useful information can still be derived from the RevMan analysis by calculating effect sizes from individual studies and making multiple comparisons when studies include more than one other intervention or control group. For this reason, results displayed in Figures 2 –4 include effect size calculations for all studies comparing LLLT to all other groups. Sensitivity analyses were attempted using only two groups per study (LLLT versus placebo; or LLLT versus most commonly used modality from the other groups), and also using only studies scoring ≥ 6 on the PEDro scale. In both instances, outcomes changed very little in magnitude or in the direction of effect (pro or contra LLLT) which also remained constant.
When interpreting these results it should be borne in mind that what is important is whether the effect size is greater than the relevant minimal clinically important difference (MCID) for the outcome measure. For pain scales, both a two point reduction on a ten point scale 50,51,52 and a 13 mm reduction on a 100 mm scale 53 have been reported as MCIDs. 54 From Figs. 2 –4, several instances of effect sizes for LLLT treatments which meet or exceed this MCID can be seen, even though pooling of effect sizes was not always possible: e.g. for participants with rotator cuff injury (Fig. 4).
Some studies used a true placebo group and others used an active control group that received a potentially beneficial therapy. This of course dilutes the effect of the treatment under investigation as the potential difference between a treatment and no-treatment would be greater than comparing the effect of a new treatment against a known beneficial treatment. In fact, the two experimental designs are attempts to answer two different questions; does it work; or is it better than the other? It is beyond the scope of this article to enter the debate over the ethics of placebo, 55 but the Declaration of Helsinki advocates for the active control orthodoxy. 56
The present study also aimed to assess the relevance of treatment/irradiation parameters to reported effectiveness. Assessment of results from positive studies provided interesting insights: Table 6 summarizes current results by anatomical site in comparison to guidelines from WALT 17 and Bjordal et al. 45
Epicondylitis
Four high quality studies provided enough information to allow comparison with guidelines; whereas power densities were within recommendations, dosages (J/cm2) used in these studies suggest that for epicondylitis the effective dosage window could be widened. Interestingly, of the inconclusive studies, Oken et al. 29 actually shows a WMD in favor of laser for both pain and grip strength (Figs. 2 –4). However, this study scored only five on the methodology scale and would be classified as low quality. While the wavelength used by Oken et al. 29 was not one identified in the guidelines, nevertheless it would be potentially beneficial for the treatment of epicondylitis.
One point to consider when analyzing the effects of any treatment for lateral epicondylalgia is that the pathology of this condition does not always originate from the tendons. The bony insertion may alternatively be the source of the symptoms; this would represent a totally different pathological problem which may respond differently to treatment. As with many trials exploring the treatment of tendon pathologies, the authors of the included trials have not made definitive differential diagnoses. Indeed, it is very difficult to distinguish between tendinosis, tendonitis, and insertional tendinopathy with lateral epicondylitis. Furthermore, elements of all three may well be present.
Rotator cuff
A range of dosages and methods of application was used for treatment of rotator cuff injuries. This may explain the conflicting results of two different research groups: two studies by Saunders et al. 35,36 used standardized treatment points and applied laser three times per week for three weeks; Vecchio et al. 37 treated up to five tender points per session and gave two sessions per week for eight weeks. Once again, even though Vecchio et al. 37 reported no benefit from the laser treatment, the effect size expressed as WMD (Fig. 4) for pain change scores favored the LLLT group. The mean change in pain for the laser group over the time period studied was twice that of the control group, which would suggest that that analysis of results in the original paper was flawed. On the whole, the effective dose for rotator cuff tendinopathies was found to lie within that recommended by Bjordal et al. 45
Achilles tendinopathy
Three high quality studies 13,39,40 and one of low quality 38 were included in the review. Bjordal et al. 13 measured prostaglandin E2 (PGE2) over the first two hours following treatment using parameters within his own recommended guidelines. 45 Results showed that LLLT was effective in reducing this proxy for inflammation over that time period. Stergioulas et al. 39 also used parameters from within the recommended guidelines. Darre et al. 38 studied treatment of Achilles tendinopathy in Danish Army recruits, however, the number of treatments given was not standardized, detail on participants was insufficient, and no criteria were given for making the decision to end treatment. The power density and the dose delivered were significantly above what would be considered appropriate by Bjordal 45 and may explain the lack of reported differences between treatment and control groups. Studies by Stergioulas et al. 39 and Tumilty et al. 40 were very similar in design, in that both looked at LLLT as an adjunct therapy to heavy load eccentric exercise; both used similar wavelengths (810 nm & 820 nm) but the power and energy densities differed. The pilot study 40 was underpowered as the aim was to gather data to inform a larger RCT in the future; therefore, these results need to be interpreted with this in mind. Once again, the studies reporting beneficial effects support the already published guidelines.
Three other studies reported negative outcomes, 41,42,43 but the design of these studies, namely the grouping of different tendinopathies together and the lack of adequate reporting of parameters or outcome data, precluded comparison of these findings with other work.
There have been few reviews focusing on the evaluation of the evidence for LLLT in the treatment of tendinopathies. Two Cochrane reviews have looked at interventions for rotator cuff tears and shoulder pain, 57,58 and made no or weak recommendations as to the effectiveness of LLLT. The rotator cuff study 57 evaluated physiotherapy interventions but did not adequately define what was included in such an intervention; therefore, no comparison could be made with the current work. The shoulder pain study 7 came to the conclusion that LLLT was more effective than placebo for adhesive capsulitis but not for rotator cuff tendinopathy. This conclusion was based on the finding of only one study for each condition, apparently due to an inability to determine sufficient detail from two of the other included studies. Another Cochrane review on interventions for treating acute and chronic Achilles tendonitis 8 concluded that there was insufficient evidence for effectiveness of LLLT, based on one study.
Two reviews looked at lateral epicondylitis; 58,59 both reported weak or negative conclusions for the effectiveness of LLLT to treat this condition. In the first review, 58 the authors acknowledged many methodological weaknesses, but they still recommended that LLLT should not be used as a sole treatment for lateral epicondylitis. However, they did acknowledge that LLLT is a dose-response modality and that the optimum dose has yet to be found. The second article 59 was a synthesis of other reviews, as well as clinical and randomized controlled trials. Again, and as noted elsewhere, 60 the review methodology had many shortcomings (inadequate coverage of relevant databases; studies rejected because they were “old”; and insufficient analysis of dosage and knowledge of dosage recommendations). The final conclusion that LLLT was ineffective seemed to be based on the evidence from only two studies, and relied strongly on the results of one study with a good methodology score.
In contrast, a recent review by Bjordal et al. 61 evaluated the evidence from 18 RCTs of LLLT to treat lateral epicondylitis and assessed the validity of treatment procedures and doses. Bjordal et al. concluded that the use of optimal wavelengths and doses resulted in beneficial effects of LLLT, either alone or in conjunction with an exercise program.
Such apparent differences in conclusions are explained in part by the Bjordal's approach in scrutinizing application and dosage information included in RCTs. Independent analysis of reported dosages as miscalculations is important, since such miscalculated dosages are not uncommon in the literature. It is noteworthy that negative reviews of laser therapy for musculoskeletal conditions can be challenged, at least in part, on the basis of inaccurately reported or inappropriate dosages. 62
The current review reinforces the validity of this approach, as analysis of results from positive studies can provide evidence of a therapeutic window for effective treatment of tendinopathies.
Limitations of the review
Synthesis of the evidence proved difficult for a number of reasons: although studies scored well in terms of methodological quality, the clinical application of LLLT was either poorly reported or varied between studies. Poor blinding procedures, lack of randomization, and lack of intention to treat analysis may have increased potential biases and weakened the scientific merit of the works reviewed. Lack of use of valid and reliable outcome measures, and inadequate detail in the reporting of these measures, made it difficult to pool data from numerous studies and thus provide any measure of estimated overall effect. We did not perform a hand search of the literature. It might be thought that one would have been beneficial, but the databases targeted and the search strategy used (Table 1) were deemed by the authors to be robust enough to minimize the possibility of missing a significant amount of literature, particularly higher quality trials.
Conclusion
This study found conflicting evidence as to the effectiveness of LLLT in the treatment of tendinopathy. Ten high quality and two low quality RCTs with positive outcomes, compared with ten high quality and three low quality RCTs with negative outcomes, were found. However, there is strong evidence from the 12 positive studies of a correlation between use of recommended dosages and a positive outcome.
The quality of reporting of clinical application techniques and parameters and results needs to be improved in future studies; this would facilitate the pooling of data for a meta-analysis. At present, the heterogeneity of studies often precludes the ability to assess the overall effect of LLLT. Furthermore, for LLLT as for any electrotherapy modality, the application technique and dose must be considered as part of any systematic review.
Finally, the quality of systematic reviews needs to follow some guidelines, such as the QUORUM statement, 19 to ensure a fair and robust evaluation of the evidence.