
Abstract
Introduction
Bone saw, chisel, and bur are used for osteotomies and bone ablations. With developing technologies, different operative approaches for these surgical procedures are used, such as laser treatment. Lasers have been widely used in surgery for hard and soft tissues. Several lasers, such as the Nd:YAG (neodymium–yttrium–aluminum–garnet), Ho:YAG (holmium–yttrium–aluminum–garnet), CO2 (carbon dioxide), and Er:YAG (erbium–yttrium–aluminum–garnet) have been used in these applications. The reported advantages of laser surgery include sterilization of the surgical site while cutting tissue, simultaneous hemostasis of small vessels, resulting in decreased bleeding and a dry surgical field, no-touch technique, reduced postoperative pain, less edema, and limited scarring. 8 Studies in orthopedic 9 –11 and oral and maxillofacial surgery 12 have suggested that the Er:YAG laser is the most promising laser system for effective and precise removal of bone. The other advantages of the Er:YAG laser in bone tissue surgery are (1) the absence of a vibration mechanism and pressure; it could be an alternative for replacing the high- and low-speed bur; (2) the possibility of removing bone tissue in places that are difficult to access by conventional methods; and (3) bone tissue ablation with precise, fast, and selective cutting. 13
Published literature has compered Er:YAG laser in osteotomy, 14 harvesting of intraoral autogenous block grafts, 15 implant surgery, 16 and removal of impacted teeth. 17 However, the reported results for lasers in bone surgery in diabetics are still inadequate. The present study compares bone healing in experimental diabetics after ostectomies obtained by Er:YAG laser and bur drilling.
Material and Methods
Twenty-eight Wistar rats weighing 250 to 300 g (Ataturk University Faculty of Veterinary Animal Care Unit) were used for this study. The rats were housed 2 animals per cage in a room with a 12-h light/dark cycle. All animal care and surgeries were carried out in accordance with an approved protocol reviewed by the Ataturk University Faculty of Veterinary Animal Care and Use Ethic Committee. Animals were given regular standard rat chow and water ad libitum throughout the experiment. Diabetes was chemically induced with streptozotocin (STZ) (Sigma, St. Louis, MO, USA), 50 mg/kg, dissolved in citrate buffer (pH 4.5) and administrated as a single intraperitoneal injection. The control rats were injected with an equivalent volume of the vehicle (citrate buffer) only. Two days after STZ injection, blood samples were collected from a saphenous vein using a 0.6-mm needle. Samples were measured by a glucometer and test strips [Optium Xceed glucometer (Abbott, Abbott Park, IL)]. All STZ-injected animals with a blood glucose of 250 mg/dL or more were included in the protocol. 18,19 The surgical procedure was postponed for 2 months until chronic complications of diabetes were evident. The reason for this delay period is that high glucose levels may lead to a disorder of bone metabolism, such as osteopenia, only when a chronic diabetic stage is reached. 20,21 By 4–5 weeks, severe weight loss and cataract were observed in all the diabetic rats. Fourteen nondiabetic (normal) and 14 diabetic rats were included in the analysis. Before surgery, the blood glucose level and body weight of each rat was checked again (starting blood glucose and body weight) (Table 1).
Values given as mean ± SEM.
Each rat was anesthetized with ketamine (10 mg/kg) and xylazine (3 mg/kg) intraperitoneally. The left hind limbs of the diabetic and normal animals were shaved and cleaned with 2% alcoholic iodine solution. Access to the femur was obtained by means of a longitudinal incision 2.0 cm long on the skin and subcutaneous tissue, and the incision was made approaching the femur laterally. A small bone window was opened without cutting muscle tissue by blunt dissection between the flexors and extensors. After exposure, the left femur distal epiphysis was perforated with a standard trephine bur, involving the cortical and medullary bone (2-mm diameter, 3 mm in depth), coupled to a micromotor (1500 rpm) under constant refrigeration with sterile 0.9% saline solution. (This surgical bur is made of high-grade stainless steel and measures 2.0 mm in diameter, with a contra-angle shank.)
Another defect with similar dimensions was created by an Er:YAG laser on the left femur of diabetic rats. The Doctor Smile erbium&diode laser (Lambda Laser Products, Vicenza, Italy) was used to induce the defect (laser source power 15 W, laser class IV, medical class IIB, network frequency 50 Hz, input power supply 230 ± 10% VAC). The Er:YAG laser with 2940-nm wavelength was used, in noncontact mode under water coolant with an energy density of 1.5 W. Time for making the cavity (involving the cortical and medullary bone, 2.5-mm diameter, 3 mm in depth) with burs was 3–4 sec. However, it took 10–12 sec with the Er:YAG laser. The incisions were then sutured with polyglycolic acid. Rats were assigned to three experimental groups: (1) normal bur group (control), (2) diabetic bur group, and (3) diabetic Er:YAG group.
In all rats, fracture of the femur during preparation of the defect, infection, or death was not seen as a result of high glucose levels. Blood glucose levels and body weights of the rats were measured again (final blood glucose and body weight) (Table 1). To compare bone healing, 7 normal (bur cavity) and 7 diabetic (bur and Er:YAG cavities) rats were killed at 10 days and again at 20 days.
Histopathologic study
The femurs were fixed with 10% neutral buffered formalin and were decalcified in 10% EDTA (ethylenediaminetetraacetic acid). The specimens were embedded in paraffin and sectioned to 5 μm thickness. Histological sections were stained with hematoxylin and eosin (H&E)and examined at a magnification of × 100. The histologic analysis was performed using the histological scoring system developed by Heiple and colleagues. 22 Scoring was carried out by two experts on histology, who were blind to the groups.
Statistical analysis
Data were analyzed using the computer program Microsoft SPSS 11.0 for Windows. The differences for union, spongiosa (internal medullary region), cortex, bone marrow, and total scores among the groups were analyzed with the Kruskal–Wallis test. The Mann–Whitney U test for pairwise comparisons was performed when the Kruskal–Wallis test indicated significant differences.
Results
Cutting efficiency with the laser was excellent, but the time required for the surgical procedure was increased. The time spent for making a cavity of 2.5-mm diameter and 3-mm depth involving the cortical and medullary bone with burs was 3–4 sec. It took 10–12 sec with the Er:YAG laser. In the present study, time measurements were recorded after obtaining the same-sized bone cavities.
Carbonizing effects or collateral damage to the tissue surrounding the bone cavity was not observed in practice with the laser handpiece's water spray. No charred tissue around the cutting edges was observed. Additional bony particles were not generated during the preparation of the cavity with the laser. Bleeding tendency during the surgical procedure was also minimal with respect to the bur. Cutting of the bone without contact and vibration was another major advantage of the laser. In all rats, there was no fracture of the femur during preparation of the defects, infection, or death as a result of high glucose levels.
Histological results at 10 days of healing
In the histological study, there was fibrous union in the normal bur group. Besides this, in the histological preparation series there were, in part, more evident areas where the development of early and active new bone formation occurred in the spongiosa. Reorganized spongiosa formation was observed in 3 of 7 specimens. Also, bone marrow occupied more than half of the cavity in 2 of 7 specimens. In this group, there was fibrinous material in most of the cavities (fibrin including a lot of tissue fragments) (Fig. 1).
Photomicrograph of a tissue sample from an animal in the normal bur group at day 10. New bone formation (yellow arrow) and fibrinous material (green arrow) can be seen [H&E (eosin), original magnification × 100].
In the diabetic bur group, there was fibrous union in most of the cavities. Osteochondral union was observed in 3 of 7 specimens. In 4 of 7 specimens, there was early new bone formation in the spongiosa. In others, there was no sign of cellular activity in the spongiosa. In this group, there was fibrinous material in all the cavities (Fig. 2).
Photomicrograph of a tissue sample from an animal in diabetic bur group at day 10. Fibrinous material (black arrow) can be seen (H&E, original magnification × 100).
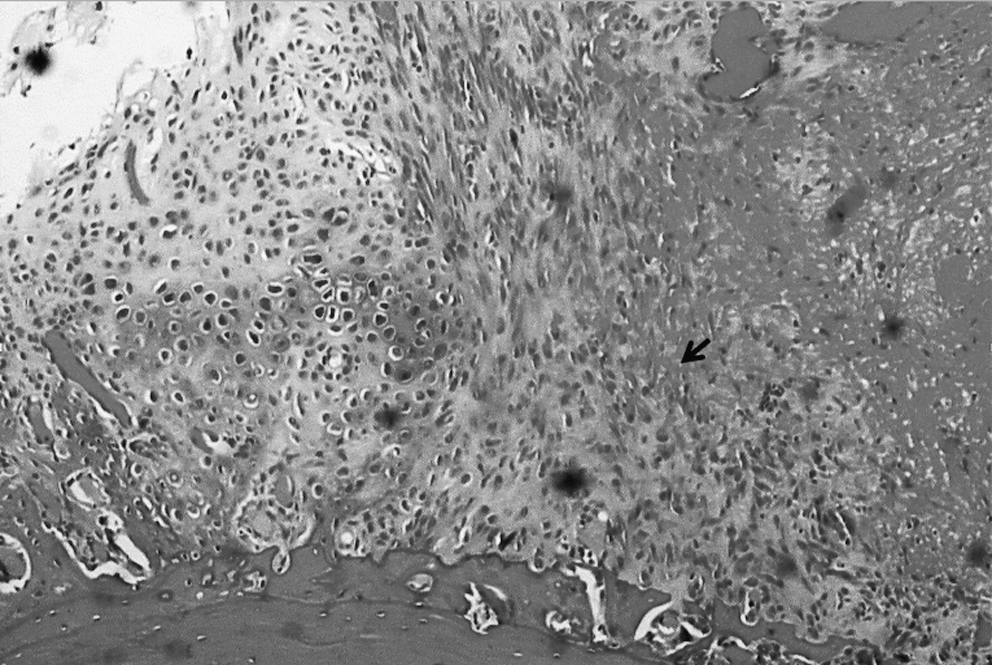
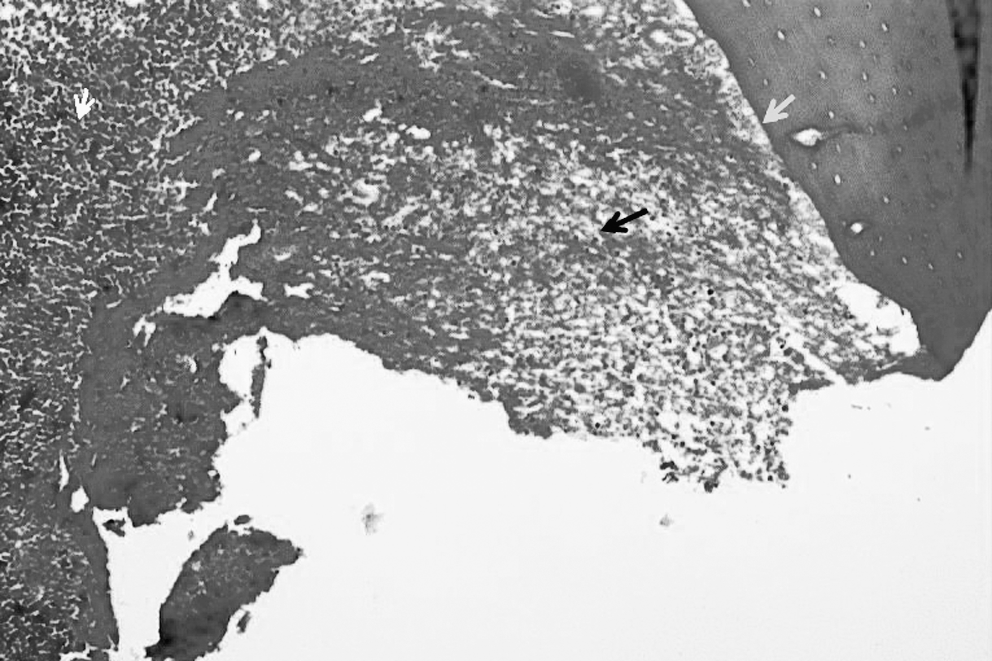
In the diabetic Er:YAG group, there was fibrous union in all the specimens. There were areas where the development of early and active new bone formation in the spongiosa was more evident. There was fibrinous material in all the cavities of this group (Fig. 3).

Photomicrograph of a tissue sample from an animal in the diabetic Er:YAG group at day 10. Fibrinous material (black arrow) can be seen (H&E, original magnification × 100).
No cortex development was observed in any group at day 10.
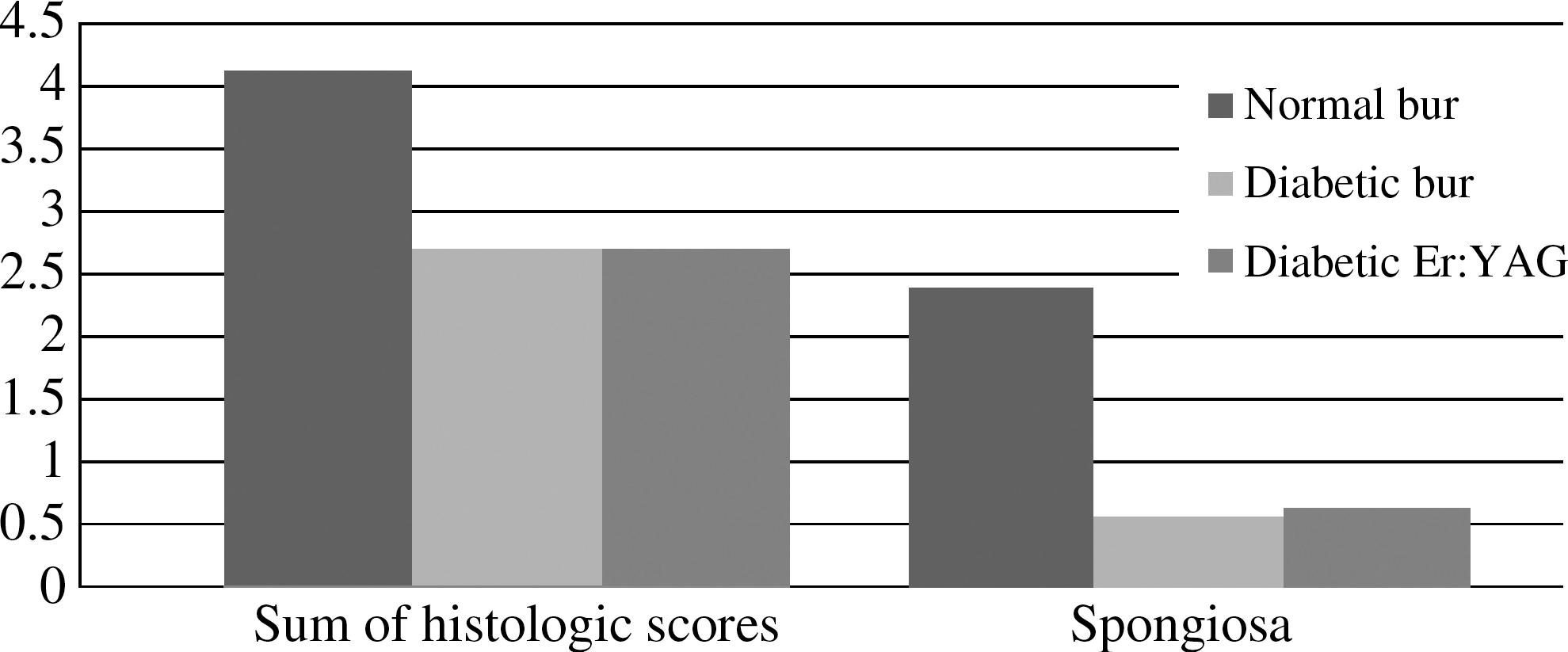
It was determined that there was a significant difference among the groups in sum of histologic scores on day 10 (Kruskal–Wallis test) (p = 0.027) (Table 2) (Fig. 4). No difference was found between the diabetic bur and diabetic Er:YAG groups (p > 0.05). Sum of histologic scores was higher in the normal bur group (mean ± SD = 4.14 ± 1.34) than in the diabetic bur (mean ± SD = 2.71 ± 0.75) and diabetic Er:YAG groups (mean ± SD = 2.71 ± 0.48).
Sum of histologic scores and
Mann–Whitney U tests post hoc were used to determine the specific differences among the groups. In the present study, union, spongiosa, and bone marrow were evaluated, respectively, and there were no significant differences between the groups for union and bone marrow (p > 0.05). Spongiosa bone formation was higher in the normal bur group (mean ± SD = 1.85 ± 0.89) than in the diabetic bur (mean ± SD = 0.57 ± 0.53) and diabetic Er:YAG groups (mean ± SD = 0.71 ± 0.48) (p = 0.011) (Table 2) (Fig. 4). (No cortex development was observed in any of the groups at day 10; for this reason it is not included in the statistical analysis.)
Histological results at 20 days of healing
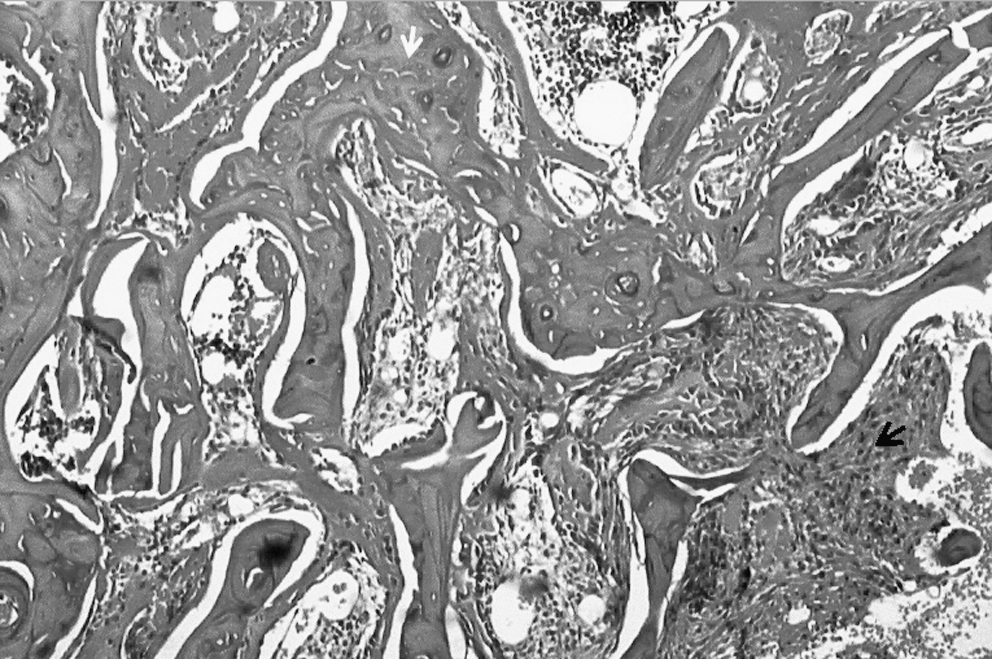
In the normal bur group, there was fibrous union in all cavities. Areas of early and active new bone formation in the spongiosa, in part, was more evident. Reorganized spongiosa formation was observed in 2 of 7 specimens. There was fibrinous material in most of the cavities, and in 5 of 7 specimens, bone marrow occupied more than half of the defect (Fig. 5).

Photomicrograph of a tissue sample from an animal in the normal bur group at day 20. Cavity border (black arrow) and new bone formation (yellow arrow) can be seen (H&E, original magnification × 100).
Fibrous union was observed in all cavities in the diabetic bur group. There were, in part, more evident areas of active new bone formation in the spongiosa. Fibrinous material was observed in all cavities. (Fig. 6).
Photomicrograph of a tissue sample from an animal in the diabetic bur group at day 20. Fibrinous material (green arrow) and new bone formation (black arrow) can be seen (H&E, original magnification × 100).
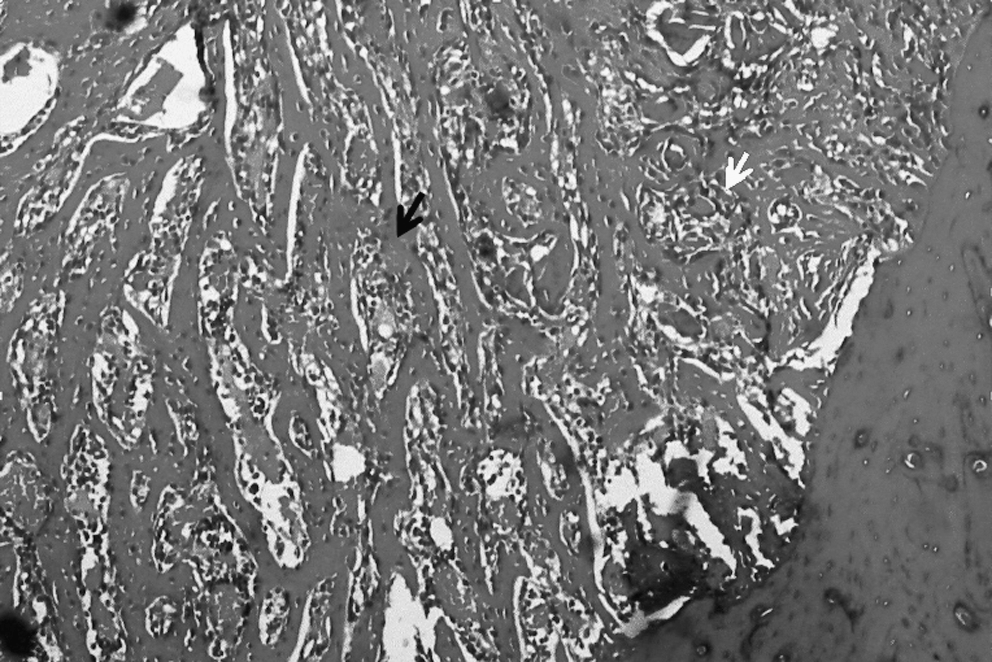
In the diabetic Er:YAG group, there were fibrous union and fibrinous material in most of the cavities. In others, osteochondral union was observed. There were areas of early and active new bone formation in the spongiosa. In 4 of 7 specimens, bone marrow occupied more than half of the defect (Fig. 7).
Photomicrograph of a tissue sample from an animal in the diabetic Er:YAG group at day 20. Cavity border (yellow arrow), fibrinous material (black arrow), and new bone formation (green arrow) can be seen (H&E, original magnification × 100).
No cortex development was observed in any group at day 20.
There were no significant differences among the groups for union, spongiosa, bone marrow, and sum of histologic scores (p > 0.05) at 20 days of healing (Table 3). (No cortex development was observed in any group at day 20; for this reason this parameter is not included in the statistical analysis).
Discussion
In previous studies, the Er:YAG laser has been reported to ablate bone effectively with minimal thermal damage and no adverse effects on bone healing. 13,23 Pourzarandian and colleagues 24 found more pronounced revascularization, faster bone healing, and more favorable surface for cell attachment in calvarial bones in rats treated with Er:YAG versus mechanical bur or CO2 laser. Ishikawa and colleagues 23 reported that the Er:YAG laser possesses characteristics suitable for oral treatment because of its dual ability to ablate soft and hard tissues with minimal damage. 23 In the study of Salina and colleagues, 25 the different bone reactions in rabbit tibiae after the insertion of mini-implants, using two different techniques of site preparation, were evaluated. It was recommended that, in comparison with traditional drilling procedures, the Er:YAG laser can be considered efficient in bone surgery without inducing irreversible damage. Based on the results of our study, we can state that the Er:YAG laser ablates bone effectively and precisely, but more slowly than steel burs. Also, there was no vibration of the laser compared to that of steel burs, which reduces the comfort of the patient and surgeon. Carbonizing effects or collateral damage to the tissue surrounding the bone cavity was not observed in our study. The results of a study by Papadaki and colleagues 26 were similar to ours. They reported that, if bone cutting using lasers is pursued, the osteotomy is easily performed and the technique is better suited to minimally invasive surgical access. It has also been demonstrated that the Er:YAG laser successfully promotes ablation of bone tissue by removing the cortical and medullar bone and was effective for the ostectomy procedure. 13 According to Lewandrowski and colleagues, 27 the Er:YAG laser appears to be an effective and precise bone ablator and is useful when control of depth is required, as in the reconstruction of midface fractures in the infraorbital and sinus region.
Also, in the study of Lewandrowski and colleagues, 27 no difference was found in the amount of newly formed woven bone at the osteotomy site or at the screw holes made by either the Er:YAG laser or the drill. De Mello and colleagues 13 compared the bone repair process after osteotomies performed either with the Er:YAG laser or low-speed bur drilling in rat tibia. They reported that histological analysis for the control group (bur drilling) showed immature trabecular bone with smaller marrow cavities than those observed in the experimental group (Er:YAG laser), and the histological analysis of the specimens in the group submitted to Er:YAG laser ostectomy presented new immature trabecular bone. De Mello and colleagues also 13 demonstrated, through histological analysis at 7 and 14 days, that the experimental group (Er:YAG laser) presented a more advanced bone repair than that observed in the control group (bur drilling). Aoki and colleagues 28 examined the healing process of the bone defect created by Er:YAG laser irradition in the long term (at 0, 1, 2, and 4 weeks and 2, 3, 6, 12, and 18 months after surgery), compared with that created by the conventional rotating bur, and reported that the Er:YAG laser was capable of ablating bone tissue with the same effectiveness as the bur treatment. The results of our study were similar to those of Aoki and colleagues. 28 Our study demonstrated no difference between the diabetic bur and diabetic Er:YAG groups in bone healing at 10 days with regard to the sum of histologic scores. It can be concluded that bone ablation with the Er:YAG laser has no negative effect on diabetic bone healing in comparison to the bur. Sum of histologic scores was higher in the normal bur group (mean ± SD = 4.14 ± 1.34) than in the diabetic bur (mean ± SD = 2.71 ± 0.75) and diabetic Er:YAG groups (mean ± SD = 2.71 ± 0.48). Post hoc, union, spongiosa, and bone marrow were evaluated, respectively, and spongiosa bone formation was higher in the normal bur group than in the diabetic bur and diabetic Er:YAG groups (p = 0.011). This might be explained by the possible results of complications of diabetes mellitus. Mishima and colleagues 29 demonstrated that streptozotocin-induced diabetes mellitus in the rat results in reduced rates of bone formation, as well as a reduced number of osteoclasts on the alveolar wall, suggesting that the early stage of diabetes mellitus produces low bone turnover. Their results agree well with histological descriptions of the bone union in fracture healing in diabetic rats. 30 In the present study, spongiosa bone formation was lowest at 10 days of healing in diabetic rats. Also, Alkan and colleaues 21 compared the bone repair process in the tibia of diabetic and normal rats. They reported that the diabetic group exhibited inferior healing when compared with the control groups in terms of the amount of new bone formation within the defects at 10 days of healing.
De Mello and colleagues 13 reported that at 21 days after surgery the histological features of the bur and Er:YAG laser groups were very similar; also the Er:YAG laser successfully promoted ablation of the bone tissue by removing the cortical bone and part of the medullar bone. The Er:YAG laser was shown to be effective for the ostectomy procedure. The results of our study were similar to the results of De Mello and colleagues. 13 In the present study, there was no statistical difference in bone healing among the Er:YAG and bur groups in diabetic rat, and there were no significant differences among all groups regarding union, spongiosa, bone marrow, and sum of histologic scores (p > 0.05) at 20 days of healing.
Conclusion
Histologically, no difference was found between the Er:YAG and bur cavities in diabetic rats in bone healing. Er:YAG laser irradiation did not affect the bone-healing process adversely. We can state that the Er:YAG laser ablates bone effectively and precisely, but more slowly than steel burs. Also, there is no vibration of the laser as occurs when using steel burs. Vibration reduces the comfort of the patient and surgeon. With these histological and experimental results, we consider that the 2940-nm Er:YAG laser (1.5 W) can be used confidently for the ablation of bones in diabetic cases.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Acknowledgement
This study was supported by the Ataturk University Scientific Research Projects Fund. The authors thank Dr. Cemal Gundogdu and Dr. Havva Erdem (Department of Pathology, Medical Faculty, Ataturk University, Erzurum, Turkey) for their evaluation of the histology slides.