
Abstract
Introduction
Numerous systems are now commercialized for this application, with either a single or a combination of wavelengths (920, 980, 1064, 1320, and 1440 nm). 11 It nevertheless remains to be seen whether the various wavelengths used in these devices are suitable for this particular application and optimized to maximize results.
The purpose of this paper is to: (1) review the typical parameters that are a function of a particular wavelength, and (2) perform a numerical simulation based on a previously developed and calibrated model. The aim of this theoretical analysis is to compare the importance of wavelength selection when operating in similar conditions.
Materials and Methods
Absorption and scattering coefficient
Out of all the parameters that need to be taken into account in order to explain laser adipocytolysis, only the absorption and scattering coefficients are a function of wavelength. Further, these two parameters cannot be dissociated. While the absorption coefficient allows for a deduction of the quantity of energy absorbed in a given structure, it invariably must be counterbalanced by scatter, which indicates how the light will spread. In fact, at short infrared wavelengths, scatter is a more important consideration than absorption. This means that photons emitted by a laser from a given point (e.g., an optical fiber) have a great probability of being scattered first, then absorbed and converted into heat. The effective attenuation coefficient is the most relevant parameter to characterize light propagation in tissue.
12
It is a combination of the absorption and scattering coefficient. It defines a primary volume, representing the zone heated directly by the laser beam, which is nearly spherical in geometry. It is given by:
where μa
(mm−1) is the absorption coefficient in tissue; μ′
s
(mm−1) is reduced scattering coefficient
Penetration depth was then calculated as the inverse of propagation.
Spectra
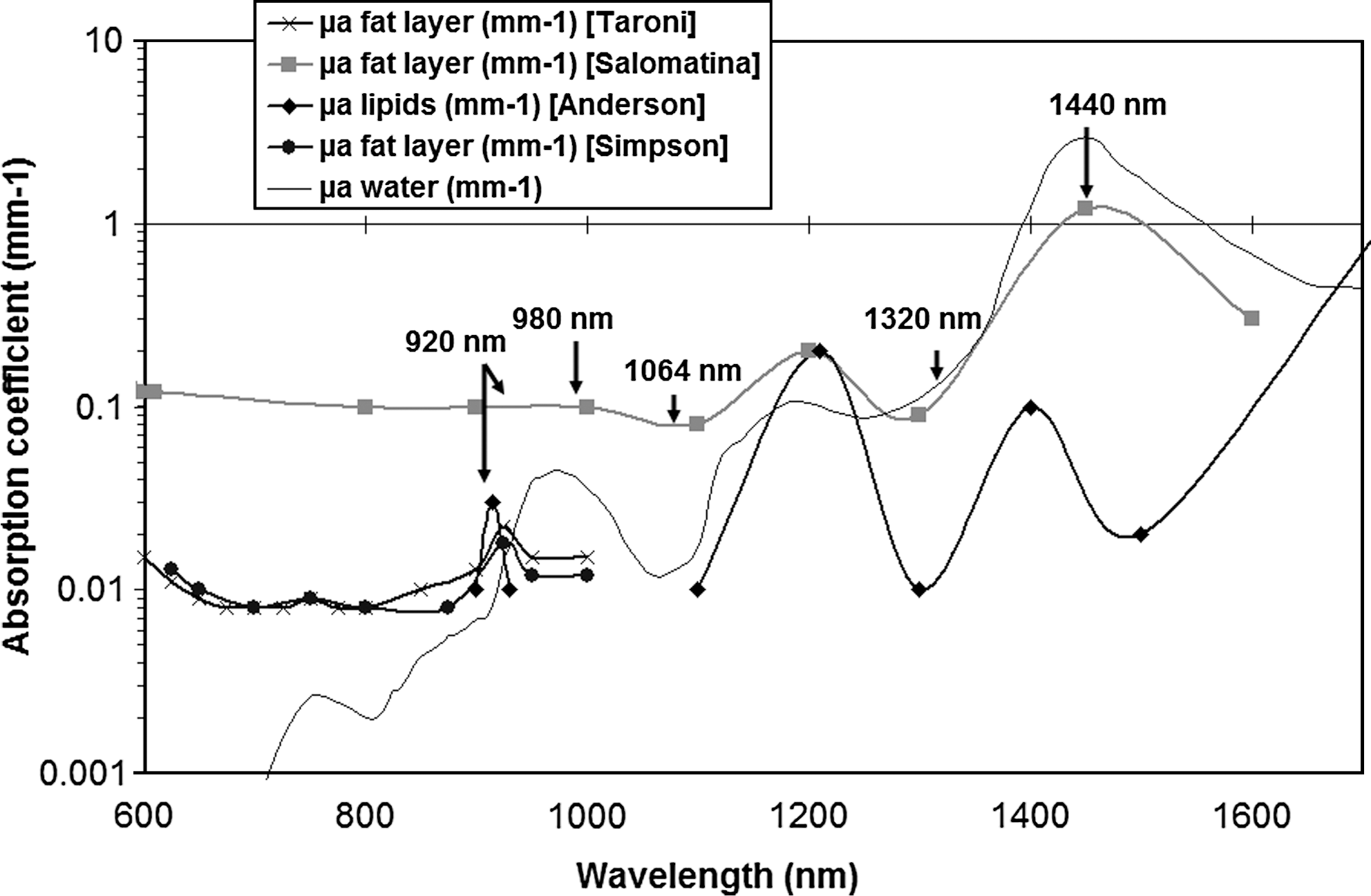
Some groups have reported measuring absorption coefficients from harvested human tissue samples. However, questions arise as to how these samples are harvested and then preserved before analysis. For example, Anderson 13 used heat to extract lipids from subcutaneous fat and then performed a spectral analysis of lipids alone. Specific absorption peaks have been identified that favor absorption by lipid-rich tissue over water-rich tissue. Taroni 14 used a similar protocol in the visible and near infrared range, and they also noted the characteristic peaks of lipids. Simpson 15 performed the same type of spectral analysis and obtained results close to those of Taroni.
Salomatina 16 conducted spectral analysis on untreated cuts of subcutaneous fat and then obtained global coefficients in different tissue types. They found two absorption peaks, around 1200 and 1500 nm. Next to these two peaks, absorption remained largely constant between 600 and 1100 nm.
Mathematical modeling
The model used for this study was developed and calibrated in a previous study published in an online free-access journal. 7 We use the same geometry and the same cannula movement inside the adipose layer for all wavelengths. Only absorption and scattering coefficients were modified in the model. As the laser was set at 15 W and fired for 250 s, the total energy delivered was 3750 J for all wavelengths.
Results
Absorption and scattering coefficient
The spectra are all shown in Fig. 1. In the visible range and up to 1000 nm, there is factor of about 10 between the Salomatina spectrum and the other spectra. In the near infrared range, the Salomatina spectrum is between the water and lipids spectra. The sample preparation prior to analysis may explain the difference.
Absorption coefficient.
With regards to the reduced scattering coefficient (Fig. 2), there are no major differences in all the previously reported spectra. The value decreases from 1.2 to 0.8 mm−1 in our range of interest.

Reduced scattering coefficient.
When the penetration depth is plotted (Fig. 3), the value increases from 1.6 mm at 920 nm to 1.84 mm at 1064 nm, then decreases to 1.4 at 1320 nm, demonstrating that there are no significant differences in absorption depth for wavelengths between 920 nm and 1320 nm. At around 1.5 mm, this average absorption depth appears to be the best compromise to achieve sufficient temperature elevation in an important primary volume. At 1440 nm, the very high absorption value implies that the laser beam will be absorbed in a very small primary volume, potentially inducing high temperatures.
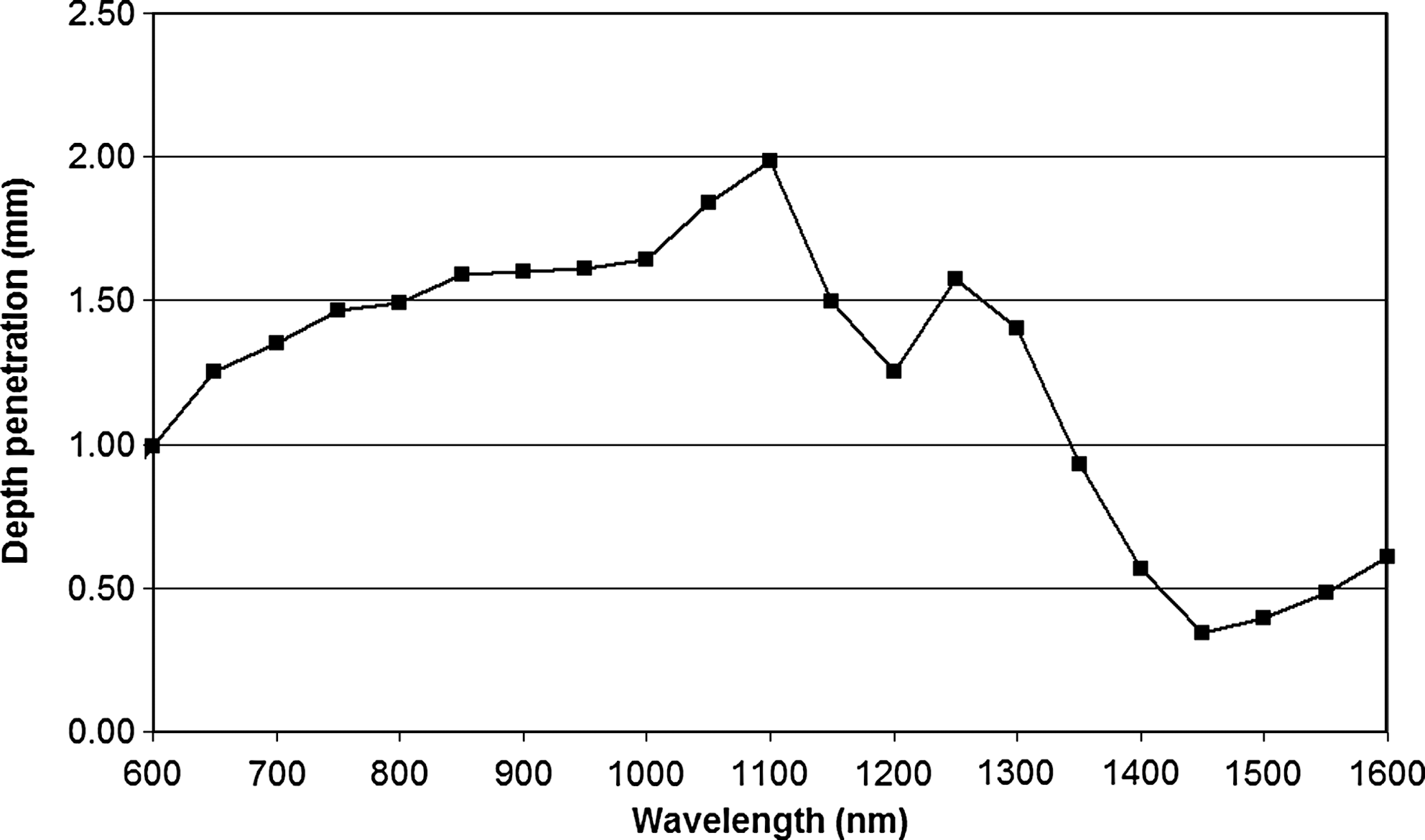
Penetration depth.
Table 1 summarizes the values that were used to simulate the different wavelengths. For the 920-nm wavelength, two values were reported because a controversy exists between considering only the lipid absorption or the whole subcutaneous fat absorption.
Considering only lipids.
Numerical simulation
The total volume irreversibly damaged at the end of the procedure for all five wavelengths is displayed in Fig. 4. There are only minor difference between 920, 980, 1064, and 1320 nm, with a final volume of damage of approximately 4 cm3 for a delivered energy of 3750 J. When considering an absorption coefficient of 0.03 mm−1 for 920 nm, the final volume is less important than for the other wavelengths. Thus, the hypothesis of considering absorption only by lipids at 920 nm seems to be insufficient to explain the thermal elevation. The small lipid peak at this wavelength does not appear to make a significant difference. The high absorption of water at 1440 nm only causes damage to a very small volume of tissue.
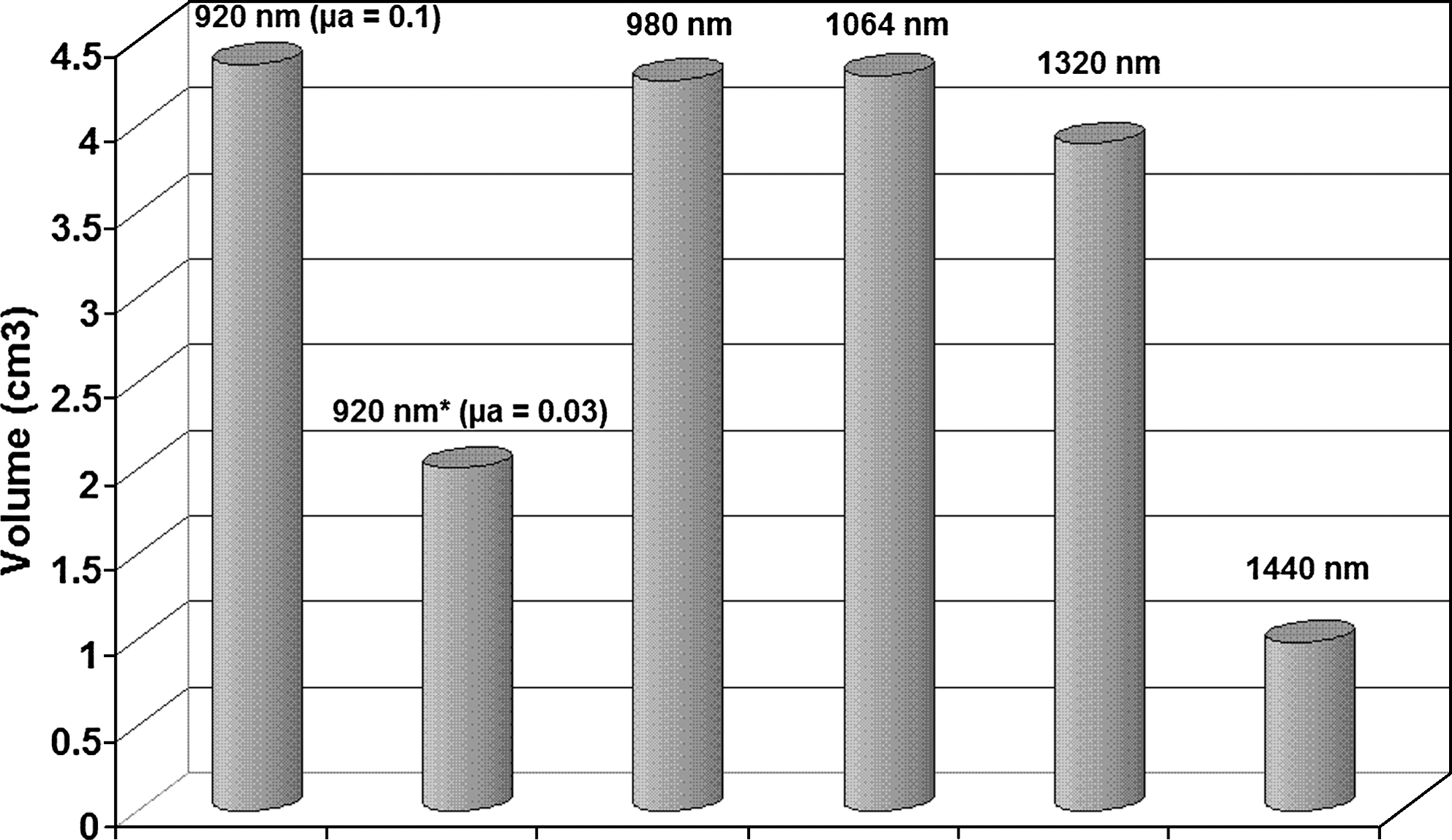
Final volume irreversibly damaged.
Discussion
The minor coefficient differences between the four wavelengths suggest similar efficacy in laser lipolysis. These differences are further moderated by two other factors. First, thermal diffusion – independent from wavelength – creates a secondary, less specific, heated volume. Second, the speed and consistency of the movement of the fiber creates a tertiary volume. As fiber movement can reach speeds of 5 to 20 cm/s, this tertiary volume far outstrips both other volumes in importance.
However, it is important that the penetration depth stays in a range of nominal value. If the penetration is too high, the primary volume will be very important, and mechanisms like thermal diffusion or perfusion will not allow for thermal elevation from the laser energy. Conversely, a penetration that is too small will probably entail carbonization phenomena inside the tissue and on the optical fiber itself. The energy used for phase transition of carbonization will not be converted into heat.
The mode use remains a mathematical model, implying that errors may appear owing to the considerations and simplifications required to realize it. But it is a comparative study and the different wavelengths are in the same conditions. The results in term of volume irreversibly damaged are completely in keeping with these remarks and are coherent with practical measured volumes. With these theoretical results, it becomes possible to estimate the influence of wavelength. But, from a practical standpoint, these theoretical differences will be too weak to be noticeable.
Certain collateral effects of laser lipolysis may well be wavelength dependent. For example the coagulation of small vessels is of great benefit in minimizing complications. Previous studies have demonstrated that, in the infrared portion of the spectrum, blood absorption is maximal in the range from 900 to 1100 nm owing to the conversion of oxy-hemoglobin to meth-hemoglobin. 17 Lasers emitting at these wavelengths may have this advantage. However, thermal elevation within the tissue is probably the main cause of vessel coagulation, implying that wavelength selection plays a minor role in vessel coagulation.
Conversely, skin retraction achieved after laser lipolysis is a consequence of the thermal elevation inside the dermis layer. This phenomenon is not directly dependent on wavelength. Nevertheless, heat diffusion versus temperature elevation and time of exposition must be sufficient to initiate fibroblast stimulation. This explains why we need a laser with an optimal penetration depth that has the ability to increase and then maintain the temperature elevation in the whole volume without significant losses.
Conclusion
This study suggests that wavelengths in the near infrared range (920 to 1320 nm) can be used for laser lipolysis with similar efficacy levels. Thermal elevation can be achieved with various systems, and the differences in terms of results are more likely dependent on operator movement or cumulated energy used. Currently, the only clinical studies available with a large number of patients and long follow-up were conducted using either 1064 nm or 980 nm wavelengths.
Finally, diode technology used to generate the 980 nm wavelength is more reliable to deliver the total amount of energy needed with a high mean power. To optimize the technique, procedure-specific accessories are more important than wavelength. These tools could ensure a control of the operator movement in order to deposit a constant energy. And they could also inform the operator about the dosimetry delivered and its homogeneity.
Footnotes
Acknowledgments
The authors wish to thank Pascal Servell for his careful reading of the manuscript.
Author Disclosure Statement
No competing financial interests exist.