
Abstract
Introduction
Laser phototherapy (LPT) has been extensively studied using several models of wound healing, and most previous reports evidenced beneficial effects for this modality of treatment. 6 –8 Studies on the healing of wounds on diabetic animals have shown the beneficial effects of the process. 2,9,10 Early laser reports were very enthusiastic, were many times anecdotal, and offered no understanding of its mechanism. Since the 1960s the volume of research into laser phototherapy has grown substantially and has focused on three areas to assess the value of LPT in wound repair: cellular function, animal studies, and human trials.
LPT is a modality of clinical treatment that results in nonthermal effects on tissues, and its biological effects cannot be attributed to heating. The magnitude of its effects depend on the physiologic status of the cells or the clinical stage of the condition before irradiation. This may explain why positive photobiomodulation may not always be detectable. 8,11
Several aspects are important for the outcome of treatments when using light sources. These parameters include wavelength, power density, energy, time, and frequency of application. 12,13 Most of the proposed protocols used different parameters, and this resulted in conflicting results. The choice of appropriate parameters is essential for the results of the treatment.
The use of laser light has been shown capable of reducing necrosis on flaps. The ability to improve angiogenesis is suggested as a major factor for the positive responses on these models. 14,15 A previous report used λ670 nm with 3, 6, 12, and 24 J/cm2 and found that flap viability was increased with the use of higher energy density. 16
The aim of this study was to assess and compare the effects of LPT (λ660 or λ790 nm, 40 J/cm2) on cutaneous flaps on diabetic rats.
Animals and Methods
Following approval by the Animal Experimentation Ethics Committee of the School of Dentistry of the Federal University of Bahia, 12 adult male Wistar rats weighing 200–230 g, obtained from the Animal House of the Faculty of Veterinary Medicine of the Federal University of Bahia, were held at the Animal Experimentation Laboratory of the School of Dentistry of the Federal University of Bahia. The animals were kept in individual plastic cages bedded with wood chips and maintained at 22°C in a day–night light cycle. The animals were fed with standard pelleted laboratory diet and had water ad libidum. After regular quarantine, the animals were randomly distributed into three groups: (1) diabetic animals without intervention, (2) diabetic animals irradiated with λ680 nm, and (3) diabetic animals irradiated with λ790 nm.
Animals of groups 1, 2, and 3 were held without feeding for 15 h and then injected with streptozotocin diluted in citrate buffer (0.1 mmol, pH 4.5, 60 mg/kg). Forty-eight hours after the injection, blood sugar level was verified (glucose oxidase). Only animals with blood sugar levels of 350 mg/100 mL or higher entered the study. 17 Under intraperitoneal general anesthesia (0.10 mL/100 g of ketamine (Ketalar®) and 0.25 mL/100 mg of xylazine (Virbaxil®), the animals had their dorsum shaved and cleaned. A 2- × 8-cm cutaneous flap was raised on the dorsum of each animal. A plastic sheet was introduced between the flap and the bed to impair blood supply, and the flap was then sutured. 16
LPT consisted of irradiation using red laser light λ660 nm, 30 mW, Φ = 2 mm [Kondortech, São Carlos, São Paulo, Brazil (G2)] or laser light λ790 nm, 40 mW, Φ = 2 mm [Kondortech, São Carlos, São Paulo, Brazil (G3)]. The dose per session was 40 J/cm2. Laser light was applied transcutaneously and fractioned on 16 contact points at the wound margins (16 × 2.5J/cm2). The time of application varied according to the equipment used and was automatically set. LPT was carried out every other day during the experimental period. The choice of the types of treatment was made because of conflicting results found in the literature regarding the effects of treatment parameters on the outcome of LPT. Two different wavelengths were used because of differences in the absorption and penetration of the laser light since both surface and deep tissues were affected.
If an animal presented evidence of pain, a nonsteroid analgesic would have been used, but this was not the case in any group. Following macroscopic examination, each animal was killed by an overdose of general anesthetic at day 8 after surgery. Specimens were taken and kept in 10% formalin for 24 h. They were then routinely cut, waxed, stained with hematoxylin and eosin and sirius red, and underwent histological analysis carried out by an experienced pathologist in a double-blind manner. Three slides were made from each specimen and the whole fragment was analyzed. The criteria used on this analysis were used previously 17 and are shown in Table 1. Each criterion was scored as absent, discrete, moderate, or intense according to the percentage of the phenomenon observed. The percentage of occurrence of each score was analyzed using Minitab15® software (Globaltech, Belo Horizonte, Brazil). For the statistical analysis, the Fisher exact test was used to compare the proportions among groups.The significance level was 5%.
Result
Control
The skin presented typical chronic inflammatory infiltrate, predominantly lymphocytic. A moderate amount of granulation tissue rich in newly formed blood vessels was observed at this stage (Fig. 1), and a moderate amount of fusiform and triangular fibroblasts was also noticed at this time. Intense tissue necrosis was observed in one specimen; it was located close to the plastic sheet. Sirius red stain evidenced a moderate deposition of a disorganized and immature collagen matrix (Fig. 2).
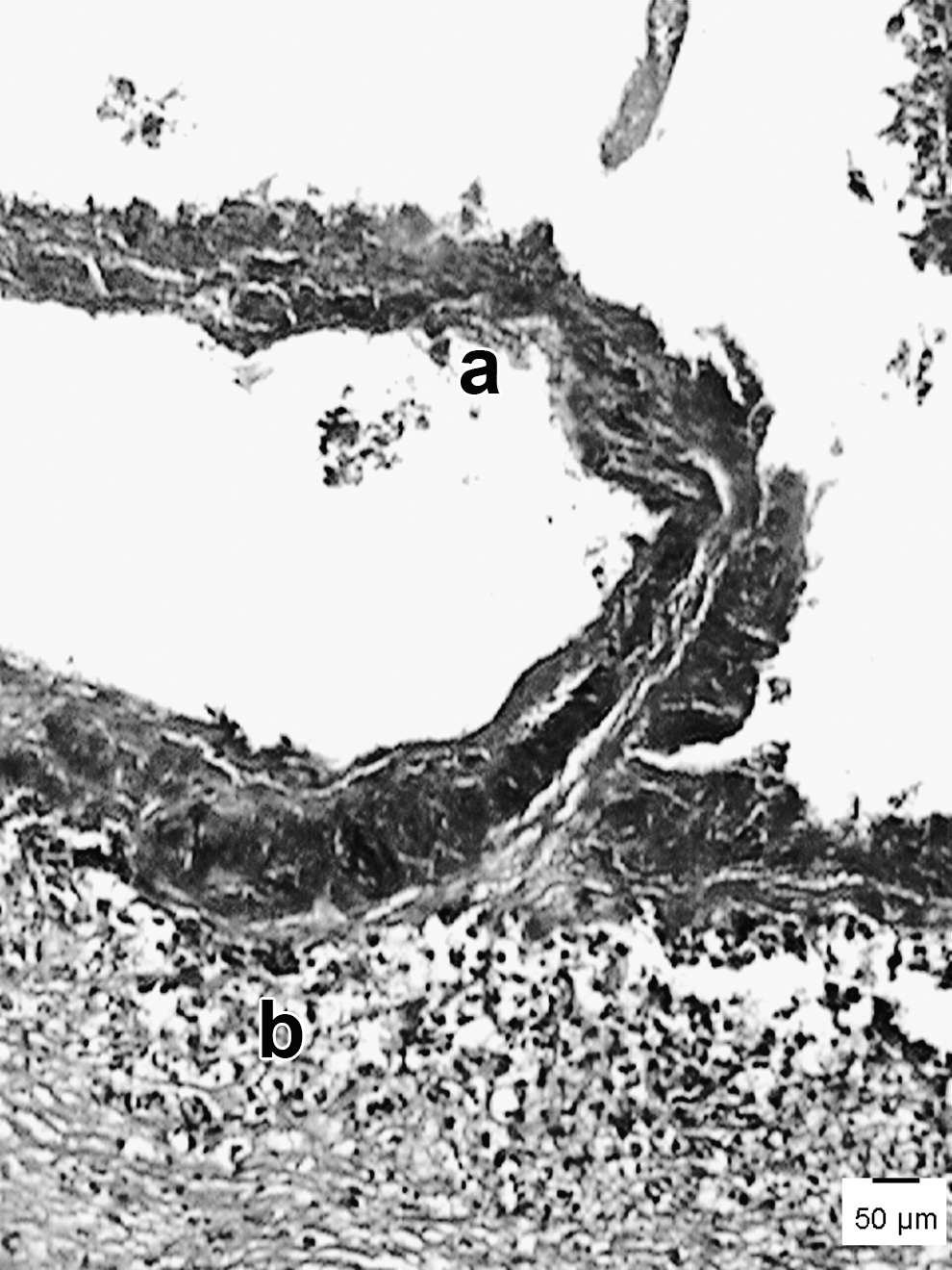
Photomicrograph of control specimen showing a band of necrotic tissue (
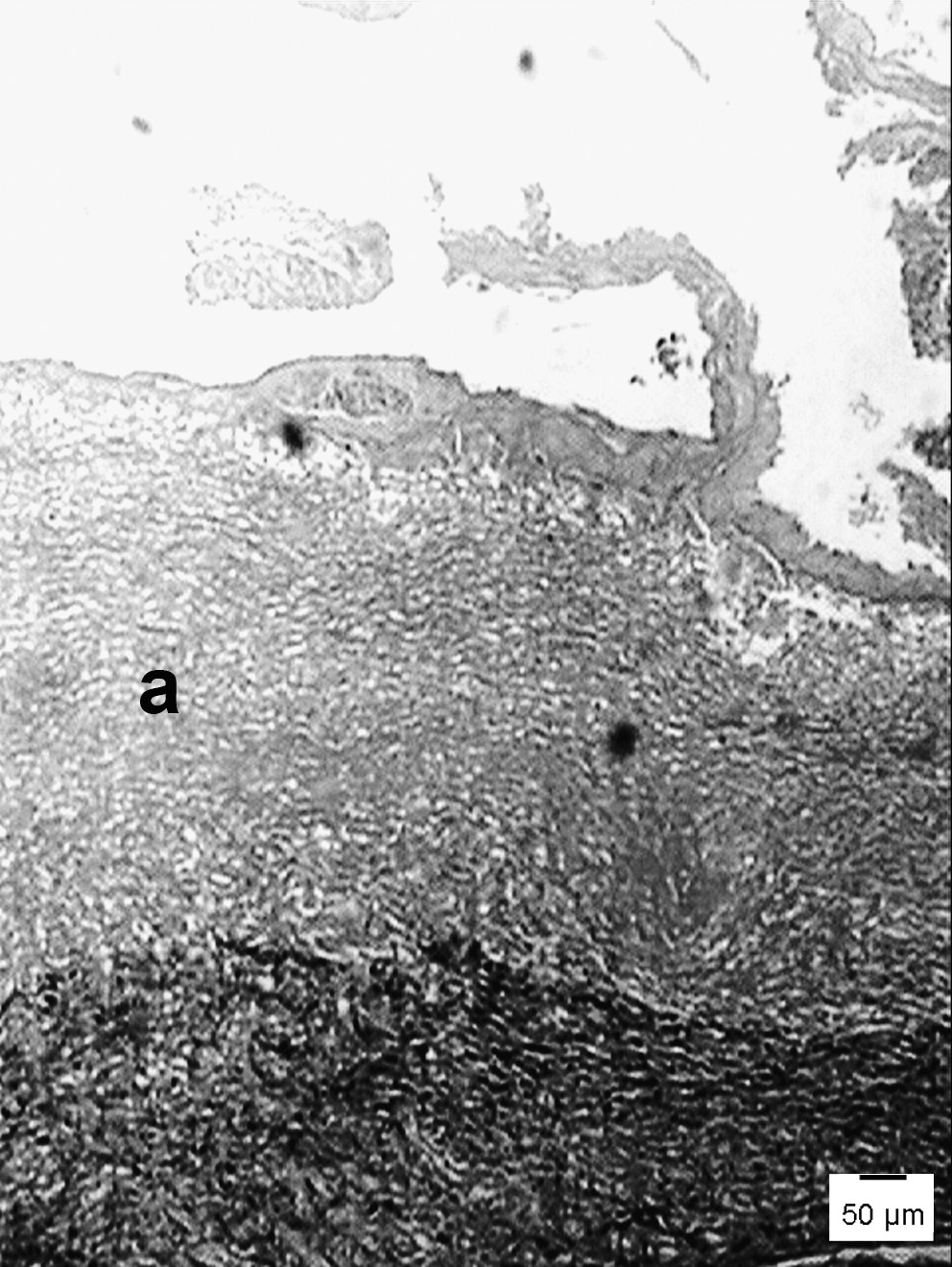
Photomicrograph of control specimen showing the presence of a moderate amount of a not well organized, still immature collagen matrix (
Laser λ680 nm
The specimens showed intense presence of granulation tissue and a typically discrete chronic inflammatory reaction. A few acute inflammatory cells were also present. The dermis showed an intense amount of newly formed blood vessels. Areas of tissue necrosis were seen in all cases close to the plastic sheet. An intense amount of fusiform and triangular fibroblasts was also observed at this time (Fig. 3). Sirius red stain showed a moderate to intense deposition of mature collagen matrix (Fig. 4).
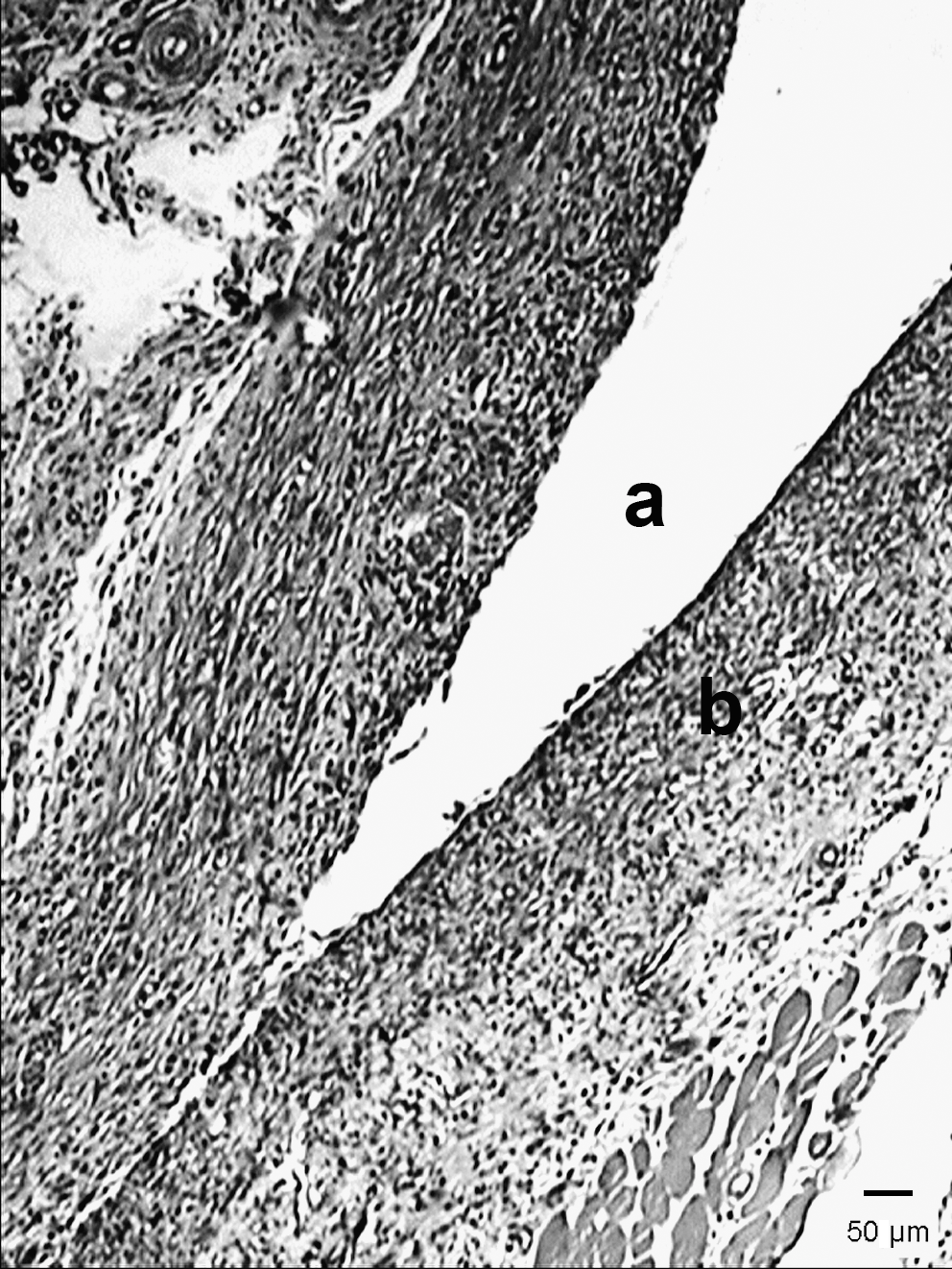
Photomicrograph of a λ660-nm irradiated specimen showing the space previously occupied by the plastic sheet (
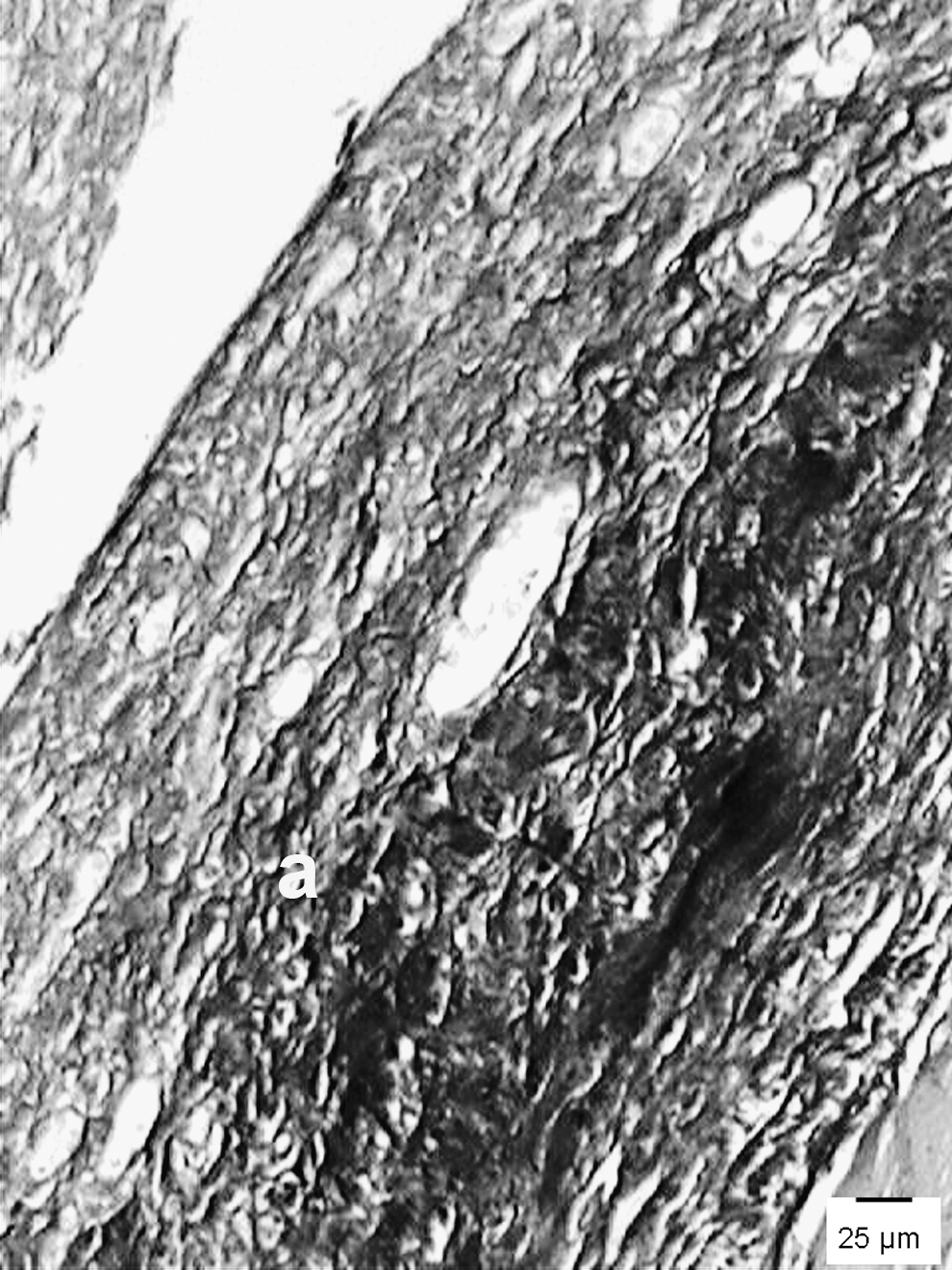
Photomicrograph of a λ660-nm irradiated specimen showing an intense deposition of collagen matrix (
Laser λ790 nm
The specimens showed a moderate amount of granulation tissue and a mostly chronic inflammatory reaction, typically lymphocytic, a moderate amount of newly formed blood vessels (Fig. 5), and intense presence of fibroblasts. One-third of the specimens presented discrete tissue necrosis close to the plastic sheet. Sirius red stain showed a moderate deposition of a little organized collagen matrix (Fig. 6).

Photomicrograph of a λ790-nm irradiated specimen showing an intense chronic inflammatory reaction (

Photomicrograph of a 790-nm irradiated specimen showing a moderate deposition of a not well organized mature collagen matrix (
Statistics showed significant differences in the level of acute inflammation between groups 1 and 3 (p = 0.04). This inflammatory reaction was not observed in G3 and ranged from discrete to moderate in G1. Significant differences were also observed for the presence of areas of tissue necrosis between G1 and G2 (p = 0.03); these areas were present on all specimens of G2 and in two-thirds of the specimens of G1. Groups 2 and 3 presented significant differences for the criteria of chronic inflammation (p = 0.04), fibroblastic proliferation (p = 0.05), and neovascularization (p = 0.04); these were more evident in G3. A summary of the significant differences is given in Table 2.
p < 0.005.
Control.
660 nm.
790 nm.
Discussion
Diabetes mellitus has been both clinically and experimentally associated with delayed wound healing. It has been shown that this unbalance causes impaired functioning of leukocytes, macrophages, and fibroblasts, as well as long-lasting inflammatory reaction and impaired synthesis of collagen and glycoaminoglycans, causing delayed development of granulation tissue. 1
It has been shown that the healing of excisional wounds on diabetic rats may be improved with the use of light therapies, including laser light. 9 The morbidity associated with long-term uncontrolled diabetes is related to several problems, such as microangiopathy, retinopathy, nephropathy, and neuropathy. Long-term assessment of these complications has been extensively studied. 3,17
This study assessed the use of laser light of two wavelengths on the survival rate of musculocutaneous flaps on diabetic Wistar rats. Flap failure owing to deficient vascularization is a major cause of failure of this procedure. 18,19 Poor blood supply is the most important cause of tissue necrosis, whereas good blood supply enhances the survival rate of the flap. 20
Our results suggest that the best responses of the flaps were observed on irradiated subjects, mainly those treated with λ790 nm. The efficiency of IR laser light was previously reported in another study. 21 However, study using 670-nm laser light on nondiabetic animals found positive results for viability of the flap. 16 Poor blood supply is the main cause of failure of flaps, and the association with diabetes decreases survival rate. 15,22
Over the last decade there has been an increased interest in the application of light sources for wound healing and other conditions. 10 In the present study, we found intense angiogenesis in irradiated subjects in accordance with a previous report using a similar model (the skin flap was made on the backs of all animals studied, with a plastic sheet interposed between the flap and the donor site). 16 Angiogenesis is essential for wound healing and for the reestablishment of local blood flow on ischemic areas, such as on flaps where tissue necrosis is a common feature. 23
We found a significant reduction of tissue necrosis on irradiated subjects, mainly when λ790 nm was used, perhaps owing to the high penetration of this wavelength. Some previous reports 14,26 also found reduced necrosis on flaps on animals irradiated with 623 nm laser light using energies of 3 and 2.9 J/cm2.
The dose is the most important parameter in photobiomodulation. At first glance, the dose would seem to be very simple and obvious: simply give so many joules per square centimeter of skin. A two-dimensional power distribution of the light on the tissue surface leads to a three-dimensional energy distribution in the tissue. 13,23
However, controversies regarding doses remain a hot topic among scientists, and previous reports have pointed out that the use of low doses results in positive effects on living organisms. On the other hand, higher doses have not been shown to have a positive effect on stimulating living tissues. Cellular proliferation is more intense 24 h after irradiation and decreases, in an energy-dependent way, up to 72 h. If the same output power is kept and time is increased, the amount of energy within the tissue will increase in the same ratio, so a larger volume of tissue will receive doses within the therapeutic window. 14
The efficacy of LPT depends on the amount of energy delivered to the tissue, exposure time, and delivery method. It is important to start the treatment using lower doses and intensity, particularly in elderly patients whose cellular response is relatively weak. The dose may be adjusted during treatment. Care must be taken to avoid inhibitory threshold and overexposure during treatment. 13,24 –26
Regarding inflammation, we found less acute inflammatory reaction in irradiated animals than in controls. Chronic inflammation ranged from moderate to intense in all groups. If we consider that in normal wound healing chronic inflammation usually starts by day 7, the use of laser light caused a more precocious response. 4,27
Intense fibroblastic proliferation was found on irradiated subjects in contrast to control specimens. These cells are responsible for collagen deposition on wounded sites, and the collagen contributes to the stability of the wound. A previous study on diabetic animals showed a reduction in fibroblastic proliferation and indicated that it was probably caused by some deficiency of growth factors. 10
We conclude that using laser light is effective in increasing angiogenesis in irradiated subjects and is more pronounced when IR laser light is used.
Footnotes
Author Disclosure Statement
No competing financial interests exist.