
Abstract
Introduction
Materials and Methods
A 20-year-old female university student presented to the otolaryngology outpatient clinic with a 3-month history of hoarseness. She was otherwise well and was a nonsmoker, with no history of passive smoking. Indirect laryngoscopy revealed an irregular lesion arising from the entire length of the left vocal cord. Microlaryngoscopy and biopsy was performed (Fig. 1). Histologic examination confirmed severe dysplasia, with squamous mucosa showing full-thickness dysplasia with atypical nuclei present in superficial layers and marked pleomorphism in the basal layer (Fig. 2). After discussion with the patient, it was decided to proceed to laser excision of the lesion with intraoperative frozen-section analysis to ensure clear margins.
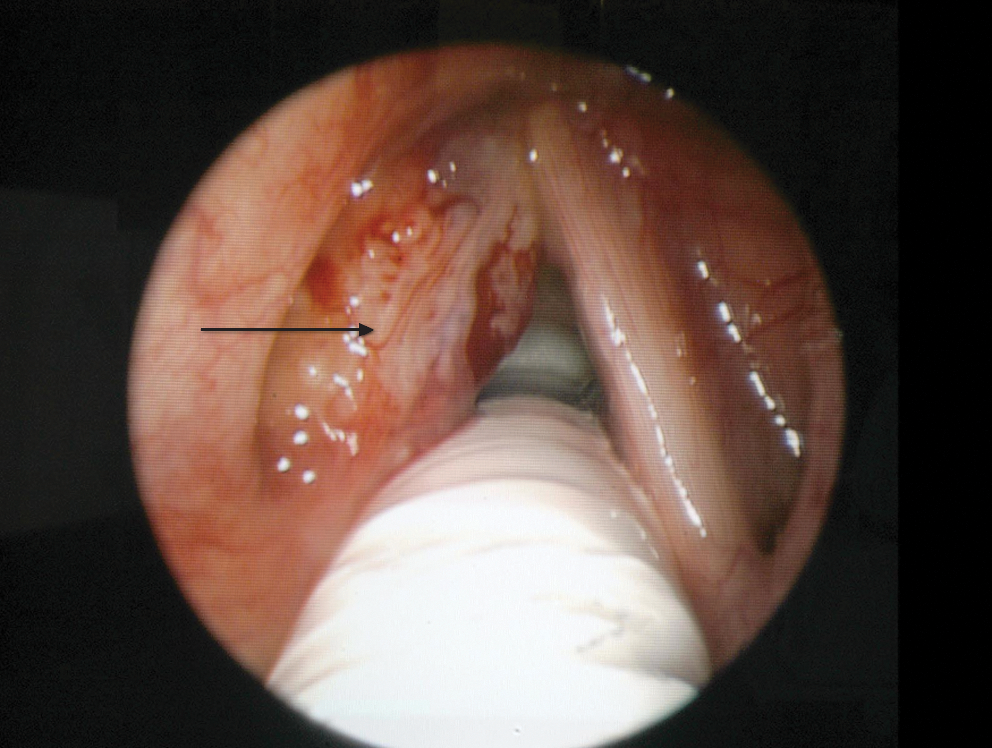
Severe dysplasia of left vocal cord (arrow).
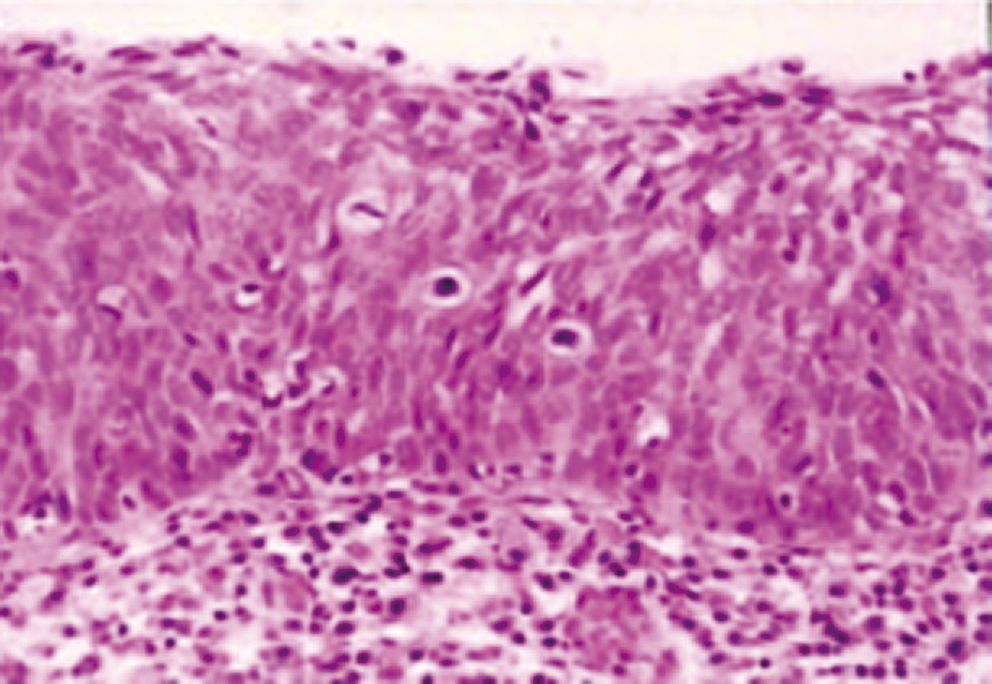
Photomicrograph ( × 20) demonstrating squamous mucosa, showing full-thickness dysplasia with atypical nuclei present in the superficial layer and marked pleomorphism in the basal layer.
Laser excision was performed with a CO2 laser, model 315M Superpulse class 4 (Irradia AB, Stockholm, Sweden). The modified Wolfgang Steiner transoral resection technique, as previously described by the senior author, 5 was performed with the CO2 laser at 6W continuous power setting. This resection technique (Fig. 3) involves a vertical split in the midline of the lesion until the muscle boundary is reached. The anterior portion of the lesion was resected, followed by the posterior portion. Frozen sections of all margins were obtained after excision was thought to be complete. This revealed persistence of dysplasia at the posterior margin, and further resection from the left posterior cord was undertaken, with a second frozen-section analysis confirming a clear margin. Formal formalin histology confirmed the specimen to contain severe dysplasia with clear margins.
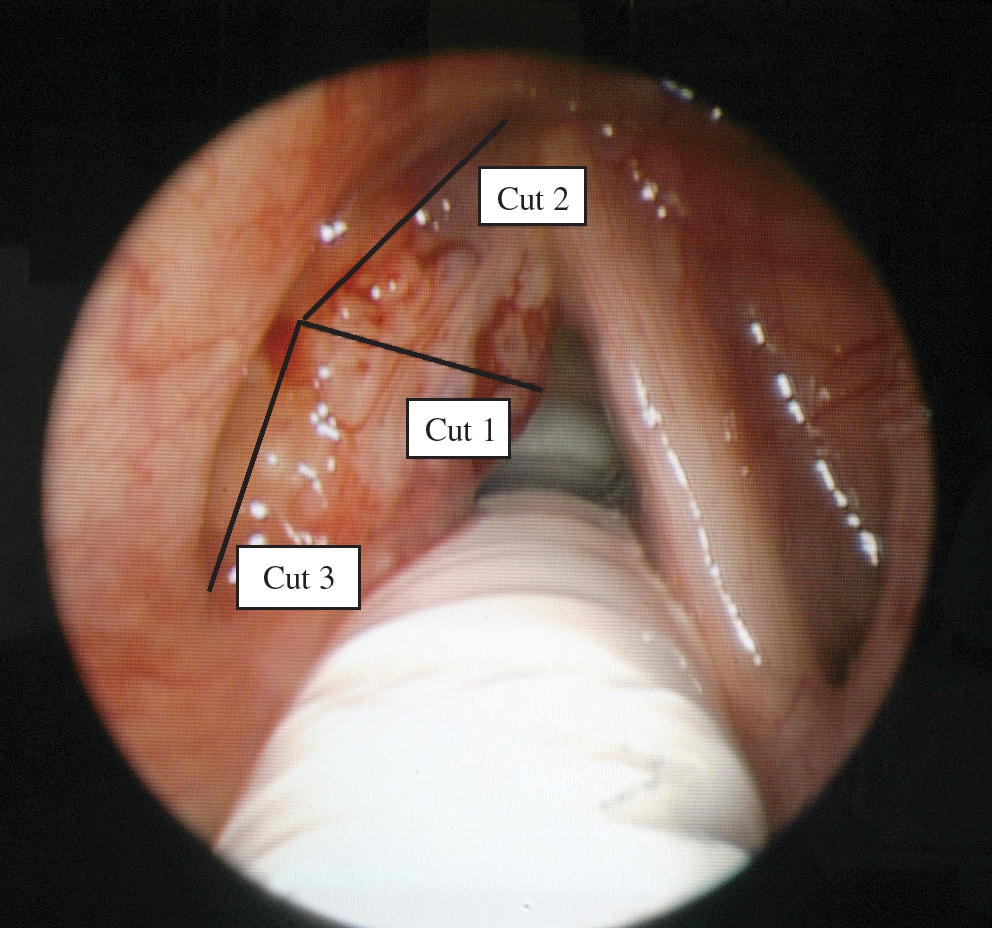
Modified Wolfgang–Steiner excision technique.
Results
Six months after operation, the patient remains disease free with good vocal quality. We plan to keep her under regular review to monitor for recurrence.
Discussion
Along with other squamous malignancies, laryngeal cancer shares an evolutionary progressive development through varying grades of epithelial dysplasia. The prognosis for laryngeal cancer shows a remarkable relation to stage, and therefore, improved understanding of the diagnosis and management of these early precursor lesions is essential to ensure optimal outcome for patients.
Dysplasia is a nonneoplastic atypical intraepithelial proliferation characterized by varying degrees of increased cell growth, cellular atypia, and architectural alteration of the epithelium. 6 It is important to make a distinction between preinvasive lesions (dysplasia and carcinoma in situ) and early invasive cancer because, whereas the former are characterized by atypical cytologic features encompassed within the laryngeal squamous epithelium (without metastatic potential), the latter reach into the lamina propria and, as a consequence possesses a potential for metastasizing.
Since leukoplakia of the larynx was first described by Durant in 1880, 7 several schemes have been proposed for the classification of laryngeal dysplasia. Because such lesions were originally described by their varying macroscopic appearances, several clinically descriptive terms have arisen over the years, including “leukoplakia,” “erythroplakia,” and “keratosis”; these, however, are nonspecific to the underlying histologic changes and as such should no longer be used. Dysplasia is a diagnosis made on histologic analysis alone, and although several categorization systems exist, the World Health Organisation classification 8 (Table 1) is the most commonly used system for the grading of such lesions within the larynx.
Limitations exist, however, with all of the currently used classification systems for laryngeal dysplasia. Inevitably, an element of subjectivity always occurs in the pathologist's interpretation of the specimen: one pathologist's moderate dysplasia may be another's severe dysplasia. Often severe dysplasia and carcinoma in situ are classified together, as the risk of invasive carcinoma from both is thought to be equally significant. 6 Additionally, often no uniformity of dysplasia is found within a single biopsy, with two different grades of dysplasia often coexisting 9 ; therefore, a finding of no or mild dysplasia is no guarantee that an invasive carcinoma does not lurk beneath the epithelial surface. A further limitation is the fact that some laryngeal cancers may develop directly as invasive neoplasms, apparently without passing through the conventional stages of progressive dysplasia. 6
Epidemiologic studies of laryngeal dysplasia have established a definite male predominance and a strong correlation between increased age at presentation and degree of laryngeal dysplasia, 2 with patients with the most severe laryngeal dysplasia in their 60s. Cigarette smoking is well established as the principal risk factor in the development of both laryngeal dysplasia and cancer. 10 Although alcohol has a strong etiologic role in laryngeal malignancy, its role in the development of laryngeal dysplasia is less well established. Over the last two decades, much work has been done investigating the role of other possible etiologic agents, including gastroesophageal reflux disease, the human papilloma virus, and gastric resection; although as yet no firm causal link has been established. 11 Similarly, many articles have attempted to correlate the expression of molecular markers, including p53, Ki-67, and epidermal growth factor, with the clinical course of premalignant lesions of the larynx, 11 although yet again, no definite relation has been proven.
Microlaryngoscopy and biopsy remains the standard method for diagnosis of laryngeal dysplasia. 12 However, this diagnostic method can be somewhat limited by sampling error, lack of sensitivity and specificity, and often the inability to discriminate between normal and dysplastic tissue. Research is currently ongoing into other methods of diagnosis, including autofluorescence spectroscopy and compact endoscopy.
The natural history of laryngeal dysplasia has been well established; it has long been recognized that as the degree of dysplasia increases, so too does the risk of malignant transformation. 1 Not so well established is the frequency and duration of follow-up required. Early forms of dysplasia may be reversible if initial stimuli (tobacco smoke) are removed, and therefore, close observation is all that is recommended by most for mild and moderate dysplasias. The rate of disease progression of severe laryngeal dysplasia to invasive carcinoma is thought by most to be unacceptably high; as such, intervention is normally recommended. 3,13
Worldwide, several management modalities are used to treat laryngeal dysplasia, including radiotherapy, laser excision, and vocal cord stripping. Traditionally radiotherapy has been the preferred method of treatment in many institutions, with protagonists claiming better voice preservation, higher rates of local control, and an enhanced ability to treat the often multifocal pattern of dysplastic disease. However, in view of our patient's age and isolated area of dysplasia, we thought that CO2 laser excision offered the best chance of disease control with voice preservation, in view of its precise application, minimal tissue damage, and rapid healing. Furthermore, laser excision would allow easier detection of any disease recurrence in the years ahead, as opposed to radiotherapy, and also afforded the option of radiotherapy to be kept in reserve as a second-line curative option should disease progression occur.
The Sadri et al. 13 2006 review and statistical analysis of these management modalities concluded that a statistically significant improved local control rate was achieved with radiotherapy (93.52%; CI, 90.80–95.50%) compared with laser excision (80.88%; and CI, 72.67–87.15%) and vocal cord stripping (77.37%; CI, 70.67–82.95%). It should be noted, however, that the types of laser used and laser procedures performed in this review were not uniform. Similarly, most of the laser excision series included do not have the benefit of intraoperative frozen-section analysis to ensure clear excision margins, as we did. CO2 laser excision plus frozen-section analysis remains the treatment of choice for patients with severe laryngeal dysplasia at the authors' institution; the reassurance of histologically clear margins minimizes the extent of radical laser excision necessary, thereby ensuring minimal morbidity and good functional voice results.
For decades, the CO2 laser has remained the gold-standard laser of choice when treating laryngeal dysplasia and maintains respectable disease-control figures. 14,15 With a wavelength of 10,600 nm, the radiant waves are absorbed by water within a depth of 100 μm from the irradiated surface, are not scattered laterally from the target point, and can be used both to precisely cut and coagulate.
In recent years, the technique of unsedated office-based laser surgery (UOLS) by using flexible fiber technology has become increasingly popular for the treatment of laryngeal dysplasia, particularly in the United States. Different laser wavelengths have been used, so far with encouraging results, including pulsed-dye laser (PDL) 16,17 and potassium titanyl phosphate (KTP). 16 –19 Compared with the CO2 laser, the 532-nm pulsed KTP and 585-nm PDL are pulsed-dye lasers whose wavelengths are absorbed directly by oxyhemoglobin, allowing involution of the lesion by targeting its microcirculation, while minimizing thermal trauma to the surrounding soft tissue. In theory, this reduces tissue necrosis, superficial lamina propria scarring, and anterior commissure web formation, therefore helping to maintain pliability of the vocal-fold mucosa and glottic sound production. Limitations of the PDL compared with KTP include its expense, the frequent need for repair (as it is not a solid-state laser), a short nonadjustable pulse width (which can result in vessel-wall rupture and bleeding), the need for larger glass fibers, and the requirement to change calibration if the power setting is changed during a procedure. 19 Although as yet no large randomized controlled trials have occurred with long-term follow-up comparing the efficacy of these different lasers on disease recurrence or voice outcomes, their role continues to be explored.
Although the quality of our patient's voice has now almost returned to normal, voice quality after laser excision remains a contentious issue. Hirano et al. 20 concluded that on stroboscopic examination, little difference in vocal function is found between postlaser and postradiotherapy patients treated for early glottic cancer. Unfortunately, most of the evidence on voice impairment after the radiotherapy or laser excision is gleaned from case series detailing the treatment of patients with invasive carcinoma and are therefore not fully applicable to the treatment of laryngeal dysplasia.
Limitations with both radiotherapy and surgical excision have led to interest in chemoprevention, which is defined as the use of pharmacologic or natural agents to reduce or reverse malignant transformation in high-risk individuals. Although much of the research has centered on oral leukoplakia, several studies have specifically addressed laryngeal dysplasia. In 1999, Papadimitrakopoulou et al. 21 reported the preliminary results of 23 patients with laryngeal dysplasia treated with isotretinoin, α-tocopherol, and interferon for 12 months. The results showed a 50% complete response rate based on histology at 12 months and partial response or stable disease in 28%. These results are encouraging, although clinical trials with larger numbers and longer follow-up are required to determine the efficacy of such treatments.
Conclusion
With the advent of various molecular diagnostic methods, we are now able to evaluate the cellular and molecular events that contribute to the development of precancerous lesions, and further research in this area may provide answers in future as to why a 20-year-old nonsmoker would develop such severely dysplastic changes in her larynx. Endoscopic CO2 laser excision of laryngeal dysplasia with frozen-section analysis is a well-established, safe, and effective treatment option for laryngeal dysplasia. However, the use of PDL and KTP lasers, particularly in the office setting, has been an exciting development over the last decade and has shown promising results in the management of this condition.
Footnotes
Author Disclosure Statement
No competing financial interests exist.