
Abstract
Introduction
Advances in technology have provided great changes in the way the devices are presented when facilitating new therapies that will guarantee significant results in treatment. 2 –4 In this context, low-level laser therapy (LLLT) is an efficient therapeutic resource for use in tissue repair, 5 and thus an important tool for the physiotherapist when dealing with a variety of skin lesions, such as exfoliations, burns, 6 surgical incisions, 7 and ulcers of different etiologies. 8,9
Among LLLT application methods, the contact technique presents advantages by providing more power density in the target tissue, as it maximizes irradiance by reducing reflexion and consequently increasing penetration into tissues. 10 However, the laser pointer can provide a way for contamination, which is minimized by the interposed transparent membrane. 11
Besides preventing contamination, the occlusive dressing has been used to increase healing rate, to keep the wound moist and protected, to induce tissue granulation, and to accelerate epithelization. 12 If it is frequently removed, however, it can cause lesions in the skin. 13 Nevertheless, the material transmissivity, which is part of the occlusive dressing material, may interfere with the power placed in the tissue and, consequently, with the therapeutic re-sponse.
Some studies have shown that transmission through different membranes by the Q-switched Nd:Yag (1064 and 532 nm) and Q-switched alexandrite (720 to 800 nm) lasers has presented various power losses. 11,14 No study was found in the literature regarding LLLT laser transmissions generated by AlGaInP (indium–gallium–aluminum–phosphide), AsGaAl (gallium–aluminum–arsenide), and AsGa (gallium–arsenide) diodes when applied to occlusive dressings, largely used for the treatment of cutaneous lesions.
Frequently, it is not possible to remove the occlusive dressing in all LLLT application sectionsand we must irradiate the lesion with the dressing interposed between the applicator and the target tissue. In this context, it is necessary to know the transmissivity property of different materials to be able to consider the loss of reflected and absorbed power. Our hypothesis is that different occlusive dressings present different laser radiation transmissions, which may depend on the wavelength.
By considering this, the purpose of this study is to investigate the low-level laser therapy transmission with different wavelengths, applied specifically on the occlusive dressings and commonly used in clinical practices.
Material and Methods
For the analysis of laser radiation transmission, a digital power analyzer, model LaserCheck® (Coherent, Staunton, VA), was used with medium levels of 0.5 μW to 1.0 W, allowing the measurement of low-level laser devices with wavelengths between 400–1064 nm. The equipment was previously tested by the Instituto de Pesquisas Tecnológicas, IPT, São Paulo, Brazil (report 63120-3/3).
Dressings were purchased in specialized markets within the validation period and stored according to manufacturer specifications. Tested materials were CombiDERM™ (Bristol Myers Squibb, Greensboro, NC), BioFill® (Biofill Technology Products SA, Curitiba, Paraná, Brazil), DuoDERM® Extra Thin (Bristol Myers Squibb, Princeton, NJ), Actisorb® Plus (Johnson & Johnson Medical Ltd., Gargrave, Skipton, UK), Hydrofilm® (Paul Hartmann AG, Heidenhein, Germany), Hydrocoll® (Paul Hartmann), Confeel® Plus 3533 (Coloplast A/S, Humleback, Denmark), Confeel® 3218 (Coloplast), transparent Band-aid® (Johnson & Johnson do Brazil, São José dos Campos, São Paulo, Brazil), Emplasto Sábia® (Johnson & Johnson do Brazil), Micropore Nexcare® (3M do Brasil, Sumaré, São Paulo, Brazil), and CIEX® waterproof tape (CIEX, Pôrto Alegre, Rio Grande do Sul, Brazil). Their physical characteristics are described in Table 1. In addition to these materials, polyvinyl chloride (PVC) Majipack® film (Inproco Industry and Trade Ltda., Campinas, São Paulo, Brazil) was measured, as it is used to isolate the laser emitter in skin ulcers to avoid direct contact between the emitter and the granulated tissue and/or secretion, thus minimizing contamination.
The electromagnetic radiation was produced by a low-level laser device (Laserpulse®, Ibramed, Amparo, São Paulo, Brazil), with wavelengths of 670, 830, and 904 nm, medium power of 30, 30, and 6.5 mW, and diode irradiation area of 0.05, 0.1, and 0.1 cm2, respectively, based on IEC 60825-1 standards. 15 The equipment was plugged into a uninterruptible power supply to avoid unexpected power disruption. Laser emission was continuous for the lengths of 670 and 830 nm and pulsed (pulses of 170 ns, frequency of 2600 Hz, and peak power of 15 W) for 904 nm. The equipment was on for 10 min before starting collection.
Laser emissions were constant (10 J/cm2) during the collection period for each dressing and the emitted medium power was measured. The laser emitter was connected to the sensor of the digital power analyzer according to the manufacturer's instructions, with the occlusive dressings placed between the analyzer sensor and the laser emitter (Fig. 1), simulating LLLT clinical practice, and specific application was applied to the occlusive dressing.

Position of the laser emitter at 90° on the Lasercheck analyzer sensor with the Micropore hypoallergic tape between them.
For each material, 15 samples were selected and irradiated once in an attempt to avoid any interference with laser radiation in the material tested.
The collection environment was controlled with a temperature of 23 ± 2°C and 60% air humidity.
Statistics were provided by analysis of variance (ANOVA), followed by Student's t-test (same wavelength) or Tukey test (different wavelengths). Pearson test was used for correlation analysis. A significance level of 5% for all measures was established. BioEstat® 4.0 software (Tefé, Amazonas, Brazil) was used.
Results
Medium values of the measured power after occlusive dressing irradiation are given in Table 2. The power transmitted ranged from 96% to 0% of the incident power, depending on the material and wavelength. BioFill, Hydrofilm, Confeel Plus 3533, DuoDerm Extra Thin, Hydrocoll, and Micropore Nexcare and the polyvinyl chloride film (PVC) transmitted power higher than 40% independently from the wavelength and area indicated for the use associated with LLLT. A small standard deviation regarding the values collected was observed, indicating that the experimental model was adequate.
p < 0.05 in relation to the respective control.
Figure 2 shows the results in percentages of the transmitted power in relation to the respective control. It can be observed that the 904-nm laser presented a lower attenuation, when compared to the 830- and 670-nm lasers. Results demonstrated that the PVC Majipack film was the material that presented the highest power transmission: 98.6%, 97.0%, and 98.4% for wavelengths of 670, 830, and 904 nm, respectively. Results for other materials, using the same wavelength sequence, were BioFill (78.6%, 83.7%, 93.8%), Hydrofilm (82.6%, 82.0%, 91.0%), Confeel Plus 3533 (72.1%, 73.7%, 78.4%), DuoDerm Extra Thin (55.7%, 64.7%, 69.2%), Hydrocoll (48.2%, 57.8%, 63.1%), Micropore Nexcare (40.3%, 40.5%, 60.0%), Confeel 3218 (17.0%, 24.9%, 29.2%), CIEX tape (10.8%, 9.6%, 26.1%), Emplasto Sábia (4.9%, 4.6%, 20.0%), CombiDerm (3.6%, 5.0%, 6.9%), transparent Band-aid (2.6%, 2.7%, 6.1%), and Actisorb (0.0%, 0.0%, 0.0%).
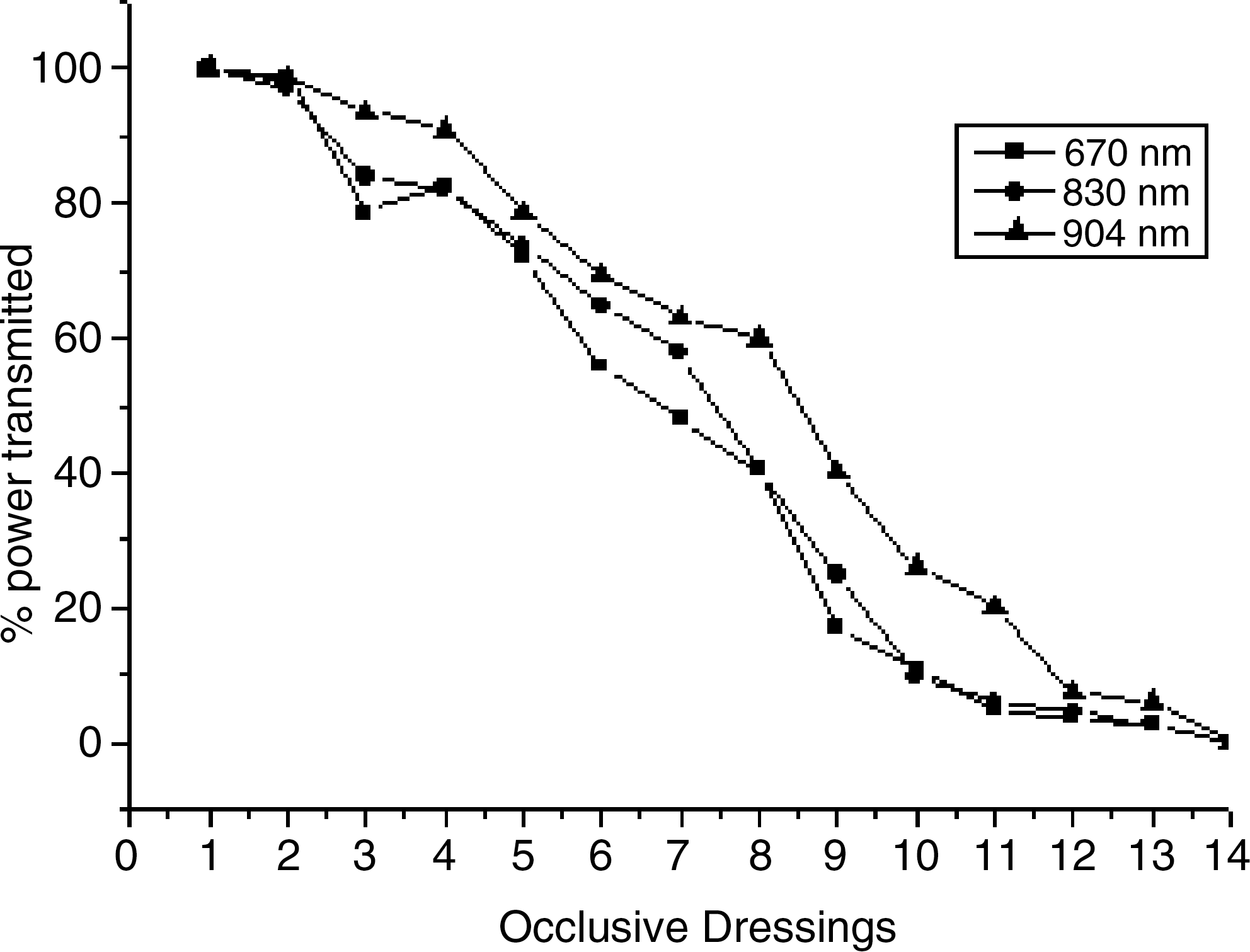
Percentage of power transmitted by occlusive dressings (1, control; 2, PVC Majipack film; 3, BioFill; 4, Hydrofilm; 5, Confell Plus 3533; 6, DuoDerm Extra Thin; 7, Hydrocool; 8 Micropore Nexcare; 9, Confell 3218; 10, CIEX tape; 11, Emplasto Sábia; 12; Combi; 13, Band-aid; 14, Actsorb) after irradiation with wavelengths of 670, 830, and 904 nm, n = 15.
The correlation analysis results showed significance between the measured power, the visual characteristic (p < 0.0001), and thickness (p < 0.04), resulting in a strong negative for the visual characteristic and moderate negative for thickness. On the contrary, both adhesive presence and density did not interfere with the measured power loss (Table 3).
Discussion
Direct application of laser radiation on the body surface entails many considerations, starting from the stratum corneum. For Parrish and Deutsch, 16 the first interaction of light with the skin occurs on the stratum corneum surface where approximately 5–7% of the incident radiation is reflected. For Tunér and Hode, 17 light penetration in the biological tissue is defined first by the wavelength, second by the device power, and also by the dispersion and absorption phenomena, which will define the energy level applied.
Skin lesions caused by surgical procedures may become infected, 18 and when the occlusive dressing is removed to facilitate the handling of the lesion, contamination may occur. 19 Thus, Lilge and colleagues 20 suggested LLLT application on the occlusive dressing to reduce the trauma caused by its removal, to reduce infection, and to facilitate skin regeneration.
When considering clinical cases, where there is indication of LLLT irradiation on the occlusive dressings, the transmission losses caused by different materials must be taken into account, because evidence shows that the biological response depends on irradiance and, therefore, needs well-defined parameters to generate therapeutic responses.
With the results presented and considering that transmissivity ranged from 98.6% to 0.0%, Confeel dressing, CIEX tape, Emplasto Sabiá, CombiDerm, transparent Band-aid, and Actsorb should not be used for irradiation with LLLT; they have a power transmission lower than 30%. The great variation in transmission among the products tested may be due to the dressing materials, including cellulose film (Biofill) and absorbent materials with activated carbon and silver (Actisorb Plus), in addition to the differences in thickness and in the presence or not of a adhesive film for fixation.
In a similar study, 11 transmissivity of a Q-switched alexandrite laser (720–800 nm) was tested in eight different types of protection membrane, and the losses found ranged from 7.5% to 48.1%. The authors observed that the material thickness did not seem to have any influence on the electromagnetic wave transmissivity, contrary to its transparency. In the current study, both the visual characteristic and the dressing thickness are correlated with the measured power when irradiated by different wavelengths. However, the visual characteristic values (−0.92 to −0.96) were higher when compared to thickness (−0.52 to −0.60), showing that this parameter was not so relevant when power transmissivity loss was considered. Opaque dressings, or the ones containing materials for absorption, attenuated more than did the thicker dressings.
In addition to losses related to reflexion, absorption, and refraction, in different strati, the absorption of laser radiation by the tissues will depend on the type of laser used, as each wavelength has a positive phototropism for a specific response. 21 To analyze this variable, Enwemeka 22 tested the penetration and attenuation capability of LLLT with wavelengths of 632.8 and 904 nm in the skin, tendons muscle, and cartilage tissues of rabbits and observed that attenuation has great influence with different wavelengths. Wavelengths of 632.8 nm presented greater attenuation in the muscular tissues when compared with 904 nm.
Our results found with occlusive dressings point to the same pattern between wavelength and attenuation that occurred in biological tissues. By analyzing the mean power percentages transmitted, it was observed that generally the highest transmissivity occurred with a wavelength of 904 nm, considering that there was no significant difference independently from the material used.
It can be questioned if the lowest power transmitted to the tissues owing to losses generated by the materials would alter the biological responses. However, there is broad variation with regard to the indications involving the ideal energy for different conditions, suggesting that the power density commonly used ranges from 1 to 10 J/cm2, even though fluences between 0.005–25 J/cm2 have been suggested. 23
Studies show that there is a dose–response relationship, as observed by Manzanares and colleagues, 24 for LLLT in the epiphyseal plate of growth cartilage in rat tibia, who concluded that the stimulating action was more effective in the fluences of 5.4 and 7.2 J/cm2, and not in 3.6 J/cm2. Al-Watban and colleagues 25 applied lasers of 532, 633, 810, and 918 nm, with energy densities of 5, 10, 20, and 30 J/cm2, to lesions of diabetic and nondiabetic rats and found that healing in diabetic rats was slower; it was most effective with the use of a 633-nm laser with energy density of 10 J/cm2.
Increasing use of occlusive materials in surgical procedures and in chronic dermal lesions demands more studies to enable the analysis of biological responses following irradiation on different materials to accelerate the healing response.
Studies that are necessary to analyze the biological response after irradiation on occlusive dressings are not available in the literature. However, we suggest that the fluence rate should be corrected for values used in studies with direct application into the biological tissue, considering the loss percentage of each material analyzed in the present study.
Conclusion
Occlusive dressings present variations in the energy transmitted by LLLT, depending on their material and on the radiation wavelength. It is recommended that the fluence rate to be applied on the dressing be corrected in consideration of the loss of transmission that occurs in different materials.
Footnotes
Author Disclosure Statement
No competing financial interests exist.