
Abstract
Introduction
Nonablative photorejuvenation technologies repair structural damage related to photoaging without disruption of cutaneous integrity. 5 The main goals of physicians in non-ablative skin remodeling are the reduction of rhytids, vascular abnormalities and solar lentigines through sequential treatments that are relatively painless and associated with relatively few complications and less downtime for the patient. 3,6 Patient expectations align with these goals and this results in an ever increasing demand from patients for such procedures. 7
In nonablative photoaging technologies, selective thermal injury leads to fibroblast activation with secondary collagen remodeling via heatshock protein, vascular endothelial factor and fibroblast growth factor modulation. 5,6,8 This leads to the synthesis of new collagen and extracellular matrix material, culminating in dermal remodeling or toning. 5
A recently introduced concept, three-dimensional (3D) skin rejuvenation, enables practitioners to integrate three different targeted treatments into a single treatment, creating a treatment series with better results and fewer treatments for the patient. The proposed aim of this 3D concept is to treat epidermal and superficial dermal damage such as sun spots and diffuse vascular lesions with a short wavelength broad band pulse light (BBPL) (Photogenesis Procedure); to treat superficial to mid-dermal damage such as large pores, fine lines, and vascular lesions with a microsecond-pulsed high repetition rate 1064 nm neodymium-yttrium-aluminum-garnet (Nd:YAG) laser system (Laser Genesis Procedure), and to treat deep dermal damage such as skin ptosis and laxity with a 1100–1800 nm infrared light source (IRLS) (Titan® Procedure).
Weiss et al. have shown that 550–590 nm BBPL photorejuvenation is associated with long-lasting improvement in superficial skin texture, telangiectasias and pigmentation. 4 BBPL photorejuvenation has been reported to result in early neo-collagenesis signs in the papillary dermis in histopathologic studies performed by Sadick and Weiss. 5
Nd:YAG laser energy has been reported to stimulate dermal collagen regrowth and realignment in the papillary dermis. 9 In this way, pore size and erythema are reduced, cobble stoning is flattened, and fine lines are decreased, resulting in improvement of skin texture. 9,10 Nd:YAG laser treatment, with a wavelength of 1064 nm, has been shown to decrease overall collagen fiber diameter in the papillary dermis, which is consistent with production of new collagen, at one and three months following completion of three treatment sessions. 9
With the help of infrared light, dermal water is heated up to a level that leads to collagen contraction. 8 Matrix-supporting collagen fibers tighten immediately and this contraction is also reinforced over time by the integration of new fibroblasts. 8,11 The clinical result is skin that looks and feels firmer. 12 Zelickson et al.'s findings 8 suggest that collagen fibril denaturation, which is consistent with collagen fibril thermocontraction, occurs immediately after treatment with the 1100–1800 nm IRLS, and that these changes are fluence dependent. Peak collagen fibril alteration occurs at 1 to 2 mm depth and this occurs at a depth range appropriate for deep dermal treatments. 7,8,12 Sachiko et al. 11 observed that greater fluence resulted in more conspicuous fibroblast enlargement, inflammatory infiltration and collagen fiber thickening in the skin of rats following 1100–1800 nm IRLS treatment. They have proposed that collagen fibers are synthesized and generated by the general wound healing mechanism after thermal dermal injury over a long period of time. 11
Non-ablative radiofrequency targets tissues at the 3 to 4 mm depth and can produce skin tightening with significant pain resulting from its application; this limits its use. 7,12,13 Taylor and Prokopenko 10 have compared radiofrequency and 1064 nm Nd:YAG laser skin resurfacing and concluded that a single treatment with either modality produced similar improvement of facial skin. Compared with radiofrequency, 1100–1800 nm IRLS has been reported to have similar, if not better, and painless clinical results. 7,12
The additional use of 1064 nm Nd:YAG laser to BBPL photorejuvenation for wrinkles has been advocated for patients for whom wrinkle reduction was an added objective, but without proven efficacy. 5 The 3D concept is purported to safely treat multiple changes associated with aging skin by using three different laser systems during a single treatment session. The procedure was developed to increase patient satisfaction with the ease of application and also to employ the synergistic effects of all of these laser procedures. Although there is worldwide use of these three instruments in 3D procedures for non-ablative photorejuvenation, until now, there has not been any scientific report on their effectiveness. This study investigates whether or not these benefits really occur through assessment of patient and physician satisfaction post-procedure.
Materials and Methods
Equipment used
In this study, two laser platforms with a total of three applications were used to target different skin layers at different depths. A broadband 560–1200 nm BBPL handpiece (LP560, Cutera Inc., Brisbane, CA) and a 1100–1800 nm IRLS handpiece (Titan®, Cutera Inc.) which are integrated into a light based platform (XEO SATM, Cutera Inc.) and a 1064 nm high peak power, high repetition rate, long-pulsed Nd:YAG laser system (CoolGlide® Vantage, Cutera Inc.) were used. The BBPL handpiece uses wavelength ranges between 560–1200 nm that target melanin and hemoglobin at the epidermal layer. The BBPL outputs energy ranging from 5 J/cm2 to 40 J/cm2, and equips a 10 × 30 mm diameter spot size and a water-circulated contact epidermal cooling tip. Its pulse width is automatically set, along with its output energy, and its stability is monitored by a real time calibration system. The 1100–1800 nm IRLS handpiece provides effective volumetric heating at the desired dermal depth (1 to 3 mm) for targeting water to stimulate new collagen. Its output ranges from 5 to 65 J/cm2, with a 10 × 15 mm sapphire tip with epidermal cooling device. The cooling device keeps the epidermal temperature at a safe level (below 40°C) by precise pre-, parallel and post-cooling. The 1064 nm long pulsed Nd:YAG laser uses high-power microsecond pulses at high repetition rates to safely heat the papillary and reticular dermis, stimulating collagen and reducing diffuse redness. This Nd:YAG laser has a wavelength of 1064 nm with a maximum peak power of 14000 Watts and a pulse duration ranging from 0.1 ms to 300 ms. The maximum fluence that can be delivered by this system is 300 J/cm2. Spot sizes are adjustable from 3 to 10 mm at the level of the hand piece. Epidermal cooling is achieved with a self-contained, internal cooling system that is administered to tissue by the hand piece. The laser hand piece was held 1 to 2 cm above the lesions, delivering energy in a non-contact mode to enable motion during delivery and prevent contact cooling.
Patient profiles
Forty-six patients with Fitzpatrick skin phototypes ranging from II to IV that were treated between 2005 and 2007, in a private laser clinic owned by one of the authors (E.C.), were evaluated retrospectively in this study. The patients had an age range between 36 and 68 years (mean, 52.43). There were 9 (19.57%) males and 37 (80.43%) females.
Patients with a history of deep vein thrombosis, pregnancy or lactation, poor wound healing diseases, hypercoagulability, connective tissue diseases, predisposition to hypertrophic scars and keloids, oral isotretinoin treatment in the previous two months, or immunosuppression were not treated. Also, patients with unrealistic expectations regarding the procedure or poor correction of the deformity on pulling the skin in the direction of vectors were not treated either.
Treatment protocol
Treatment sessions were conducted after taking informed consent and in accordance with the principles of the Declaration of Helsinki, the International Conference on Harmonization Guidelines for Good Clinical Practice, and local regulatory requirements.
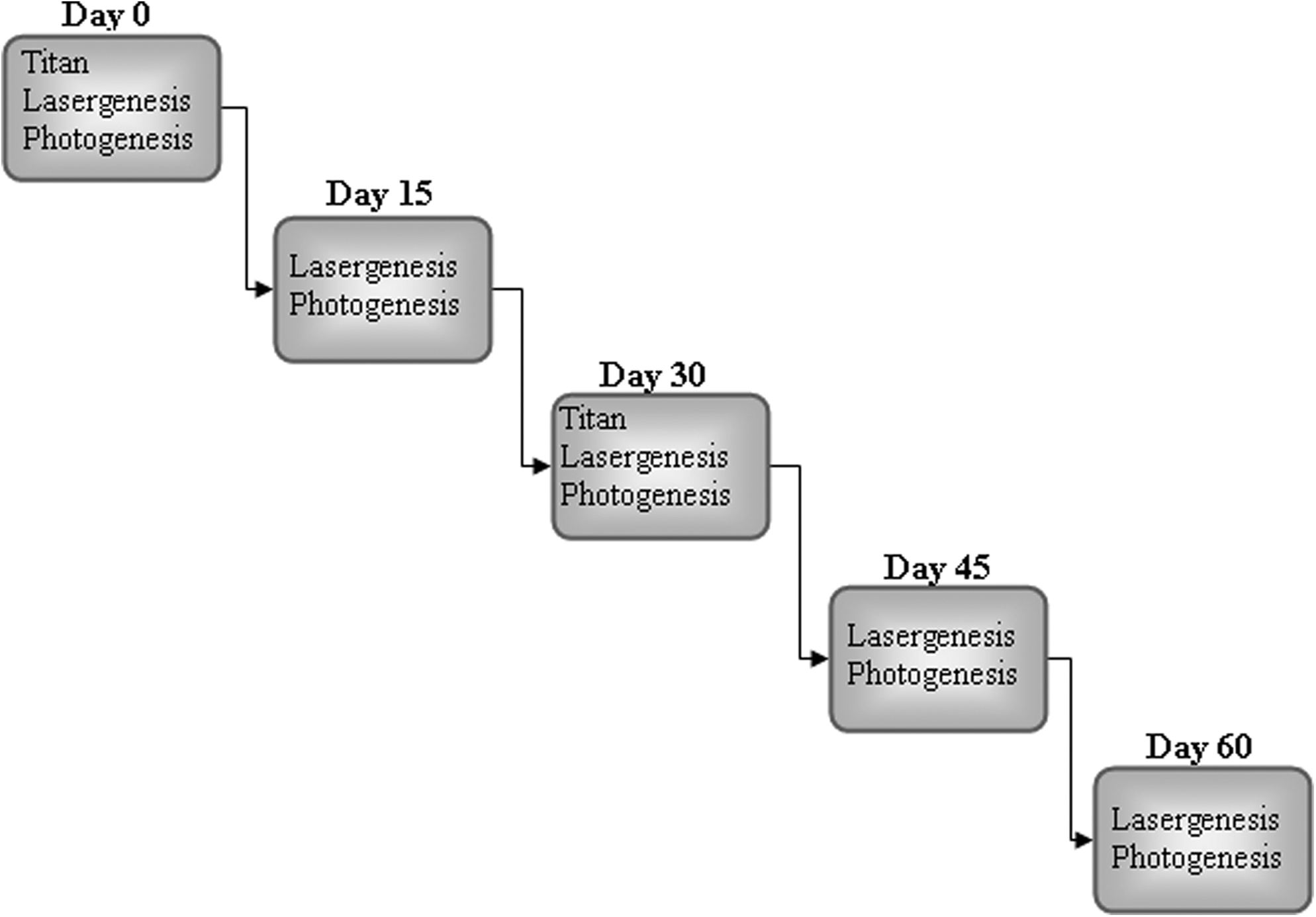
All of the three procedures, photogenesis, laser genesis, and titan procedures, were applied to all of the patients. The 3D procedure was carried out in five sessions (Figure 1). In the first and third sessions, all three procedures (Titan®, laser genesis, and photogenesis) were applied in the same order to all of the patients. In the second, fourth, and fifth sessions, laser genesis and photogenesis procedures were applied in the same order to all of the patients. The visits were spaced two weeks apart in accordance with the manufacturer's advice considering commencement of skin healing and remodeling of the dermis. The treatment protocol, methods and parameters were set according to those of previously published reports 12,14 –18 , the manufacturer's guidelines, and the authors' experiences. The application of the 3D procedure was performed from deep to superficial layers. First, the Titan™ procedure (approximately one hour), second, laser genesis (approximately 30 minutes), and lastly, photogenesis (approximately 10 minutes), were carried out according to the treatment protocol for each patient. All of the patients received almost identical treatment protocols, with only minor differences in the pulse duration periods and fluences.
Treatment Protocol.
In the Titan® procedure, a 1100–1800 nm IRLS hand piece was used with fluences set to 34–37 J/cm2, according to the patient's pain threshold based on the treatment protocol of Taub et al.'s multicentre study (Table 1) 12,14,15 . As the fluence decreased, 10% more pulses were applied. Light exposure durations were set automatically and ranged from 6.5 to 7.2 milliseconds (ms). After thorough facial and neck washing, hydrophilic gel was applied on the skin surface prior to the IRLS exposure to smooth the skin surface and improve the contact with the handpiece tip. The skin required no other pre-operative care. The basic treatment plan involved identifying areas which had redundant or overabundant skin (such as at the jowls or submental fat pad) and their corresponding vectors of lift. Vectors were determined by pulling on the skin with the second and third fingers in the direction of correction desired and finding the best location of the pull while the patient was sitting up 18 . For a lifting effect, multiple passes were done to these vectors. For overabundant skin, multiple passes were performed just to the area to be shrunk. 12 Two focused passes were applied to all of the patients within a one-month interval. 12,14,15
In the laser genesis procedure, clinical investigations performed by Schmults et al. 9 and Lipper et al. 17 were taken into consideration to determine the 1064 nm Nd:YAG laser treatment parameters; a fluence range between 13 and 14 J/cm2 (Table 1) and a pulse width of 0.3 msec with 5 mm spot size. This procedure was applied within a two week time interval. 17 The total number of pulses was 1500–2500 for forehead, 1500–2500 for cheek, 1500–2500 for the perioral area, 1500–2500 for neck, and 8000–12000 for full face and neck on average. The skin was heated with a 5 mm hand piece held 1 cm from the skin and moved with back-and-forth motion in each area, with a concentration over the problematic areas with wide pores or fine lines and in perioral and dorsal nasal areas. Vascular lesions in the face were also treated with one to two sessions of Nd:YAG laser treatment over a six-week interval (spot size 3 mm, 150–170 J/cm2, pulse duration 10–20 ms) 16 .
In the photogenesis procedure, a test pulse with a fluence of 12 J/cm2 was carried out with a BBPL handpiece in the first session to identify the approppriate fluence for each subject. Fifteen minutes after this test pulse, the skin reaction was observed. We looked for darkening of pigmented lesions and minimal changes in background color. In this study, mild erythema and darkening of pigmented lesions were accepted as the end point of the treatment. We reduced the fluence when skin erythema and burn injury were significant. There was mild erythema following test doses in all of the patients but this erythema disappeared within a few hours in all patients. The treatment started with a fluence of 12 J/cm2 and there was not any need to use a lower fluence. Fluence was increased by 2 J/cm2 at each session (Table 1). The dose escalation was not changed in Fitzpatrick skin phototype III and IV patients. Exposure durations were set automatically. The application was carried out throughout the face irrespective of the presence of sun spots.
Pre- and intra-operative considerations
Patients washed their faces and wiped off their make up before the procedure. The subjects' eyes were protected with external ocular shields and laser pulses were applied on the skin extending to the orbital rim to protect the eyes. There was not any requirement for anesthesia for the patients before the operations. Gel was not used during the procedures, except for the 1100–1800 nm IRLS applications.
Postoperative considerations
All of the patients were informed that some degree of erythema (lasting for a few hours), swelling, burning, vesiculation, darkening of sun spots, crusting, and, rarely, erosions were expected after the procedure. The patients were instructed not to excoriate these lesions and advised to apply topical fucidic acid cream on a twice daily basis for three days. Following completion of each treatment, all of the patients were advised to use sunscreen and to stop the use of all cosmetics except for moisturizer creams. Patients were examined before and immediately after the treatment sessions and at least three months following the last treatment session. Photographs were taken before and immediately after the first treatment session and more than three months after the last treatment session.
Evaluation
The primary end point of the study was physician assessment of the treatment outcome. Results were judged by an experienced laser dermatologist (E.C.) both by direct patient examination and by comparing “before” and “after” photographs. Results were ranked in five categories ranging from 0 to 4 (0: no improvement, 1: poor improvement, 2: mild improvement, 3: moderate improvement, 4: significant / excellent improvement). The secondary end point of the study was patient assessment of treatment outcome. At the final control, all patients were asked to rate their satisfaction with the procedure in five categories ranging from 0 to 4 (0: not satisfied, 1: barely satisfied, 2: somewhat satisfied, 3: satisfied, 4: very satisfied).
Statistical analysis
In order to compare the satisfaction of doctors and patients with respect to gender, skin type, season, and age group, we conducted Mann-Whitney U and Kruskal Wallis tests depending on the number of samples. We took the type I error level α as 0.05.
Since our data were ordinal, we used the Spearman's rho statistic to assess the correlation between satisfaction levels of doctors and patients after the final laser application. A correlation value of 0.60 or higher was considered to indicate a strong correlation between the variables of interest.
Case reports
Case 1
The 3D procedure was applied to a 58-year-old female patient with skin of phototype II. Five months after the final treatment session (Figures 2 and 3), doctor and patient satisfaction scores were both 4.
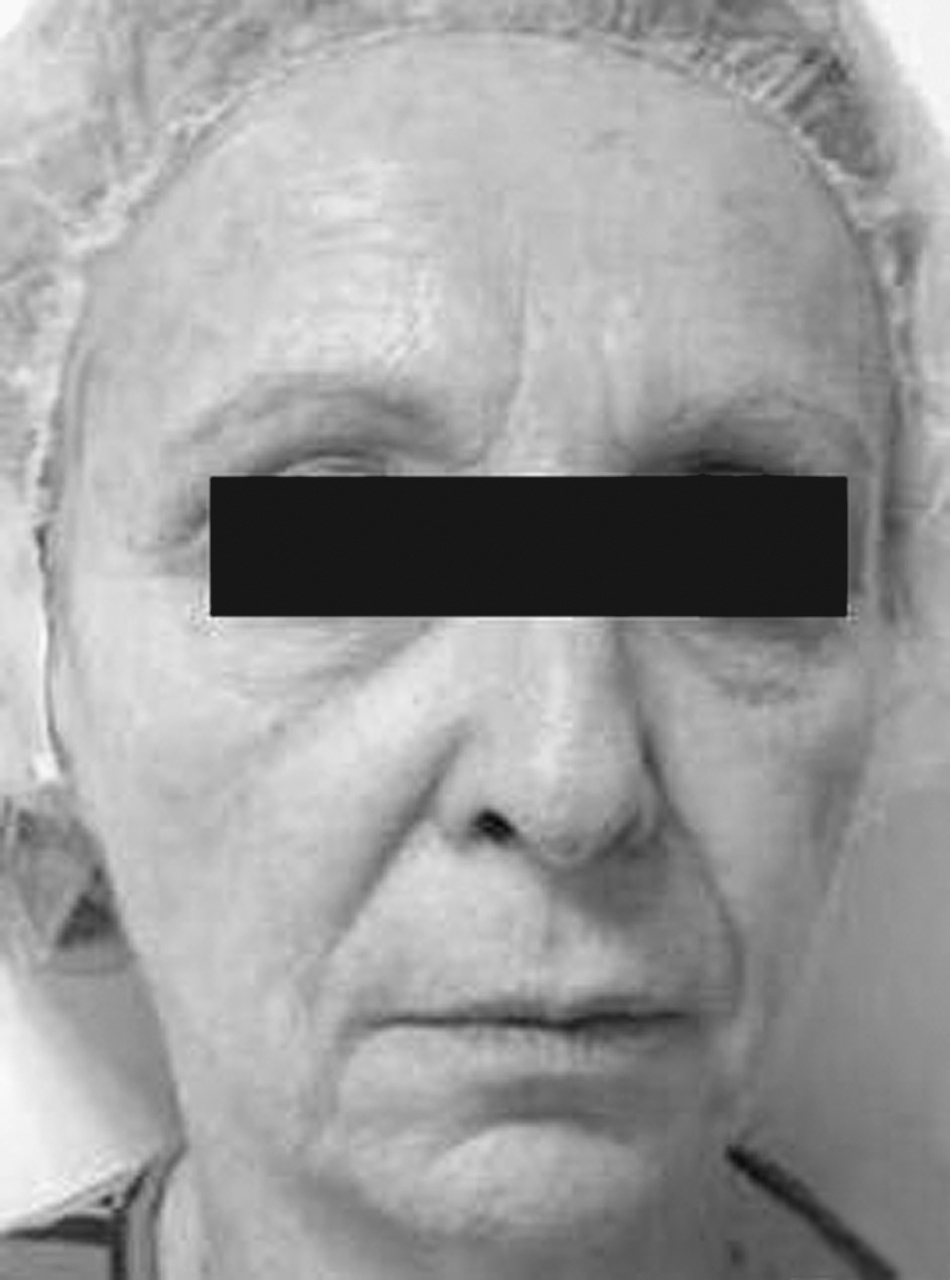
Case 1: Clinical appearance of the patient prior to treatment with the 3D procedure.

Case 1: Five months after the final 3D treatment session: improvement of skin texture and pigmentation (asterisks), elevation of eye brows (arrows) and improvement of nasolabial sulci (arrowheads) are seen.
Case 2
The 3D procedure was applied to a 60-year-old female patient with skin of phototype III. Three months after the final treatment session (Figures 4 and 5), doctor and patient satisfaction scores were both 4.

Case 2: Clinical appearance of the patient's periorbital and nasal lines prior to treatment with the 3D procedure.
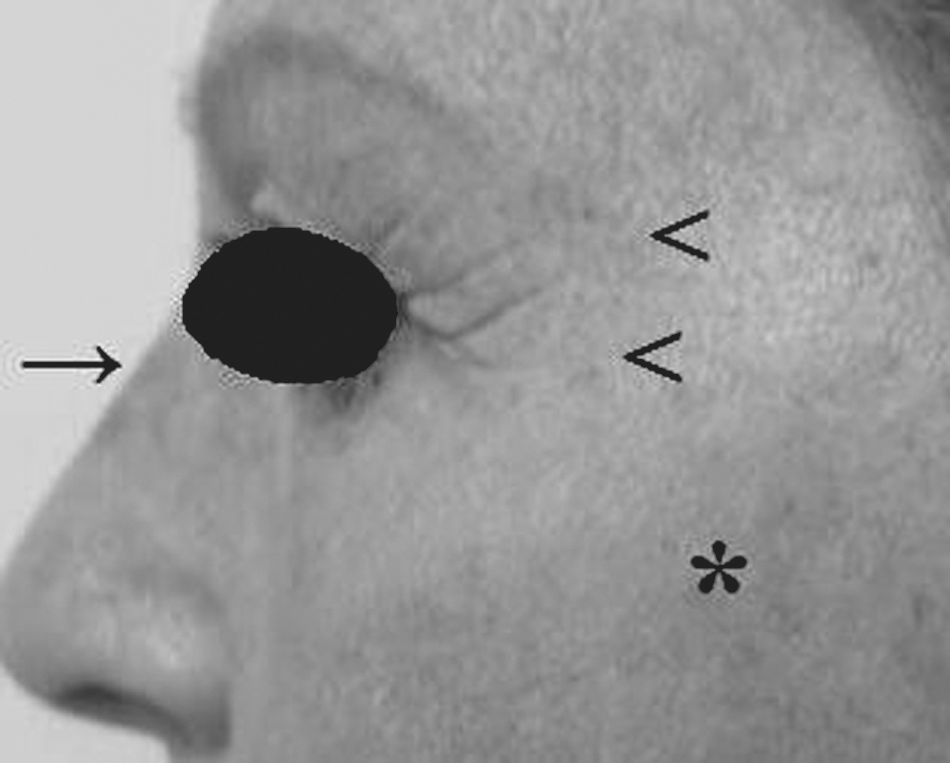
Case 2: Three months after the final 3D treatment session: reduction of pigmentation (asterisks) and improvement of periorbital (arrowheads) and nasal (arrow) fine lines are seen.
Case 3
The 3D procedure was applied to a 60-year-old female patient with skin of phototype II. Nine months after the final treatment session, significant improvement of facial and neck creases and neck laxity was observed (Figures 6 and 7). Additionally, improvement of perioral and chin lines was significant (Figures 8 and 9). Doctor and patient satisfaction scores were both 4.

Case 3: Clinical appearance of the patient's facial and neck rhytids and neck laxity prior to treatment with the 3D procedure.
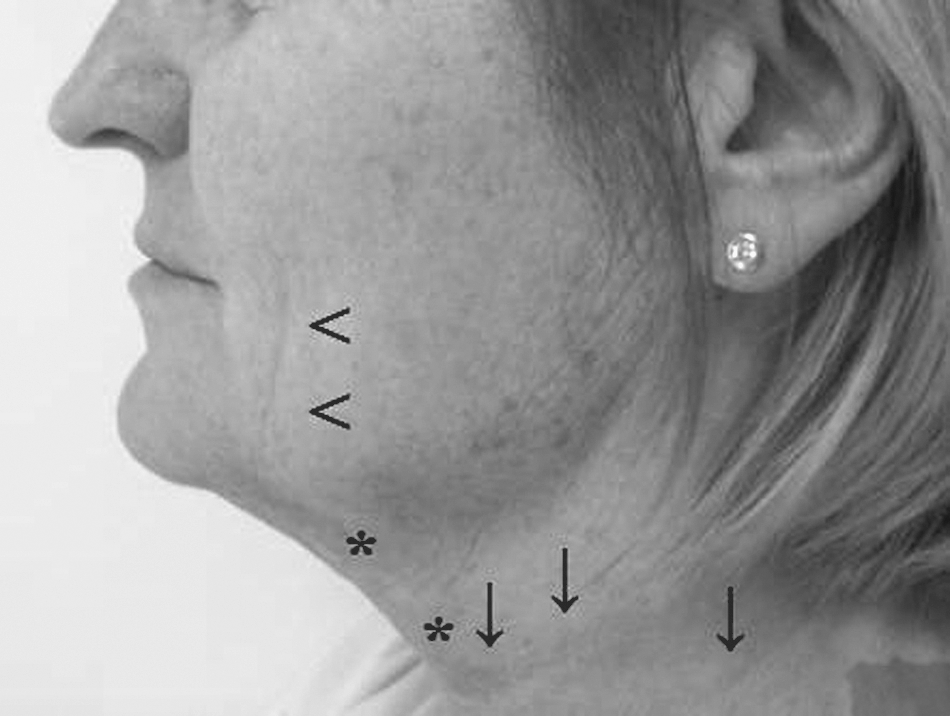
Case 3: Nine months after the final 3D treatment session: improvement of facial (arrowheads) and neck (arrows) rhytids and neck laxity (asterisks) is seen.
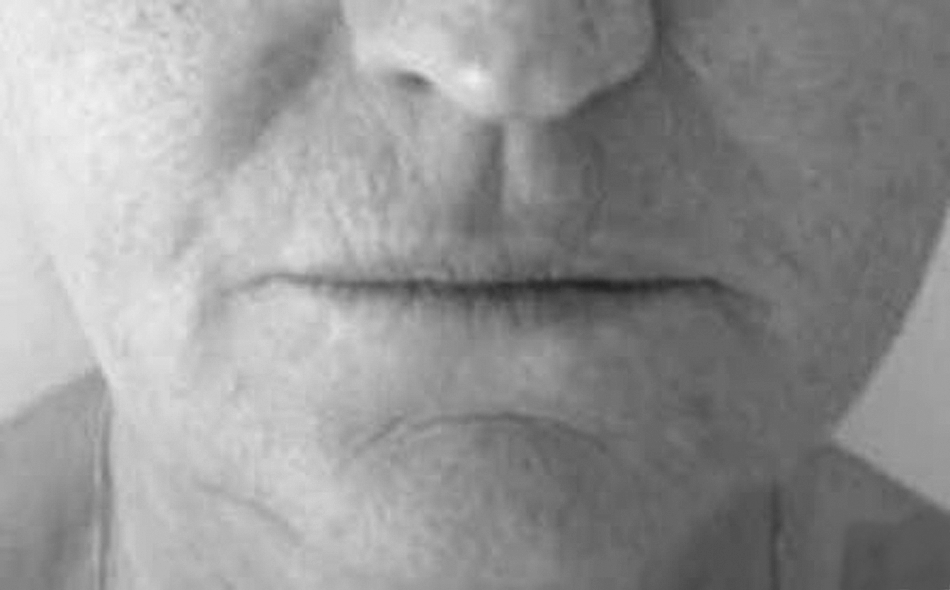
Case 3: Clinical appearance of perioral and chin creases prior to treatment with the 3D procedure.
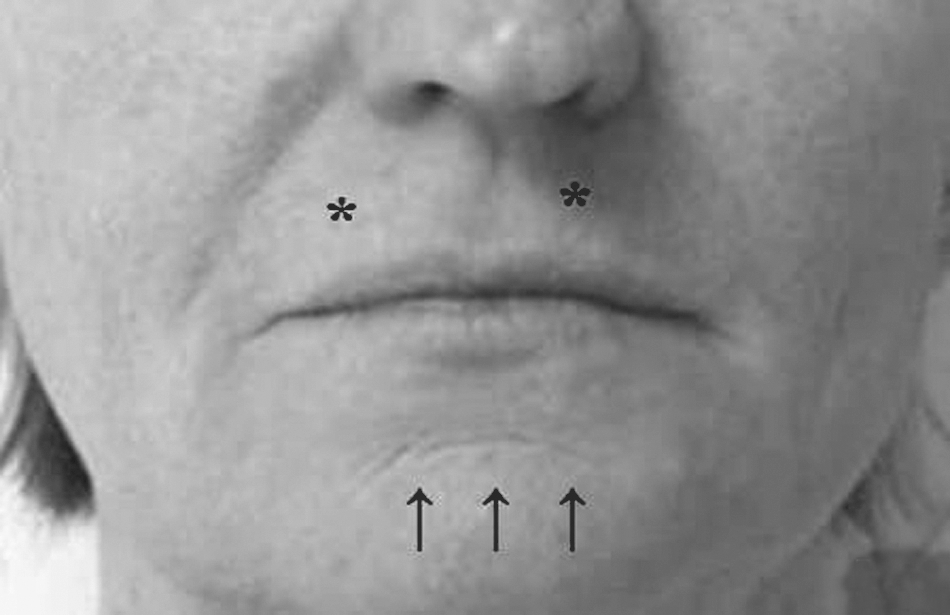
Case 3: Nine months after the final 3D treatment session: improvement of perioral (asterisks) and chin (arrows) creases is seen.
Case 4
The 3D procedure was applied to a 36-year-old female patient with skin of phototype II. Three months after the final treatment session (Figures 10 and 11), doctor and patient satisfaction scores were both 2.

Case 4: Clinical appearance of the patient's nasolabial and marionette lines before treatment with the 3D procedure.
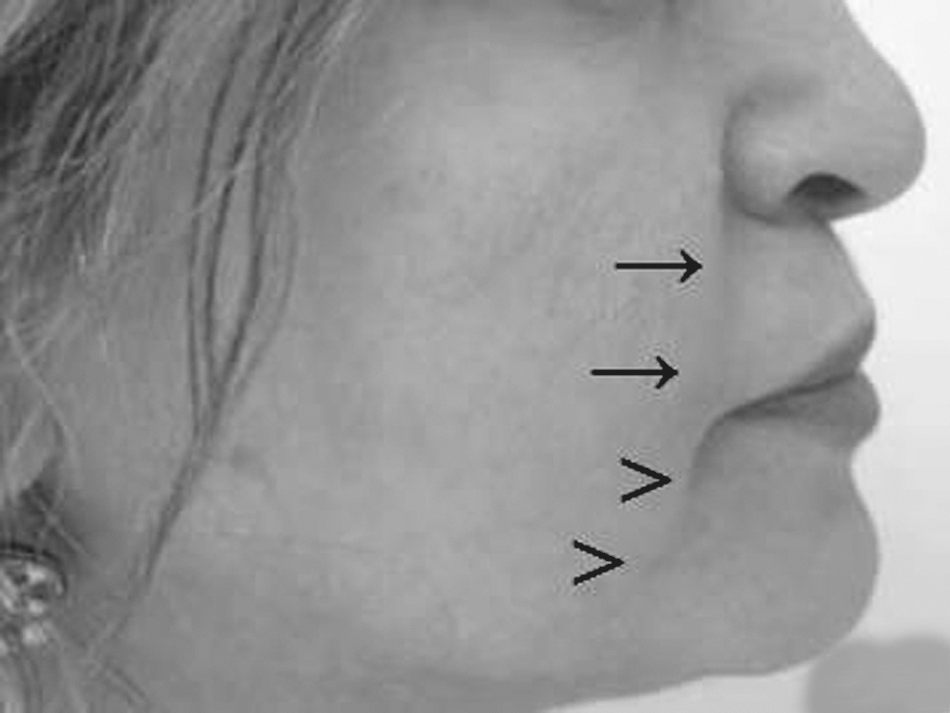
Case 4: Three months after the final 3D treatment session: improvement of nasolabial lines (arrows) and marionette lines (arrowheads) is seen.
Results
For the photogenesis procedure, there were no differences in side effects. In all of the patients, brown spots developed over the sun spots following the application of BBPL and these were shed off spontaneously within 10 days. Development of these brown spots decreased significantly towards the final treatment session as a result of bleaching of skin color. All patients were advised to refrain from touching these spots and to let them disappear spontaneously.
Vesiculation developed in only two patients during the 1100–1800 nm IRLS treatment. This was probably due to improper fitting of the hand piece to the face of the patient, resulting in incomplete skin cooling. These patients were advised to use topical fucidic acid cream. The vesicles resolved in one week without any scar formation.
Patient and doctor satisfaction levels are shown in Table 2. We compared doctor and patient satisfaction with respect to gender, skin type, season, and age group. The results showed that there was a significant difference between groups in terms of doctor satisfaction. Doctor satisfaction was significantly higher for female patients (p < 0.001) than for male patients, and for patients aged 60 or higher (p = 0.028) than for younger patients. Female patients as a group were significantly more satisfied with the procedure (p = 0.003) than male patients. The patients who were dissatisfied with the 3D procedure were those whose expectations of the procedure were high and who had comparatively more subcutaneous fat than other patients.
Patient and doctor satisfactions levels following the 3D procedure were generally correlated. This correlation was especially evident in female patients, patients with Fitzpatrick skin phototype II, and patients who were younger than 50 or older than 60 years (Table 3).
Discussion
Sachiko et al. 11 inferred that collagen fiber production due to the wound healing process continued for three months following the irradiation of rats with 1100–1800 nm IRLS. In nonablative photorejuvenation, the collagen remodeling response is also delayed, and maximum regeneration occurs 30 to 90 days following treatment. 6,12 We therefore followed up our patients for at least three months. Whenever we observed immediate improvement, follow-up visits showed that this improvement was maintained and even increased, as seen earlier. 12,14
Taub et al. 12 reported their results from 42 patients treated by 1100–1800 nm IRLS. They observed improvement in 91.75% of their patients, with a mean improvement score of 1.8312. Obviously, our results are better than these results, as all of our patients showed some degree of improvement and the mean overall patient satisfaction score was 2.65. Alexiades-Armenakas 19 reported that pre- and post-treatment laxity grading scales were significantly different, with a 14.1% change following one to three 1100–1800 nm IRLS treatment sessions. Carniol et al. 14 treated 10 Caucasian females with 1100–1800 nm IRLS for facial skin tightening. They reported that the mean overall satisfaction of their patients was 6.4 on a scale of 0 to 10. 14 We found in our study that the female patients' mean overall satisfaction was 2.78 on a scale of 0 to 4, and this is comparable to their results. Ahn et al. 15 studied 1100–1800 nm IRLS for facial lifting in nine Korean women with Fitzpatrick skin types III to IV. They reported statistically significant improvement in all subjects but especially in the group that received two treatments separated by a one month time interval. 15 We also applied two 1100–1800 nm IRLS treatments, one month apart. Ahn et al. 15 reported an overall improvement score of 2.9 on a scale of 0 to 4 in the two-session treatment group using photographic evaluation 15 . Similarly, our doctor mean satisfaction scores were 3.03 for 37 female patients and 2.93 for the 27 patients with skin phototypes III to IV. Moreover, our results are comparable with those of Ruiz-Esperza 7 for a group of patients treated for cheek and neck flaccidity with high fluence and pulse parameters. One difference between our study and these previous studies was the fact that we combined 1100–1800 nm IRLS treatment with BBPL and Nd:YAG treatments and achieved similar or even better results in facial lifting. We also obtained additional positive effects with regard to skin texture, telangiectasias and wrinkles.
Non-ablative laser resurfacing procedures have the disadvantage of variability of response among patients and among different regions of the face in the same patient 3,14 . Even if the same parameters are used in treating the patients, there are variations between clinical responses, which range from minimal to complete clearing of wrinkles. 3 We also observed variations among responses between different patients.
We observed that obese patients with more subcutaneous fat are poor candidates for this procedure. Clinical improvement has been reported to be achievable but this has been less reproducible when there is voluminous subcutaneous tissue or thick and/or sebaceous skin. 12,14 We have also found that male patients are less satisfied with the procedure than female patients. This may be due to the fact that male patients have greater epidermal and dermal thickness and a larger percentage of sebaceous glands when compared with female patients. 20
Physicians must be confident that their patients have realistic expectations from this procedure. Results have not been so dramatic that they could be compared with the results of plastic surgery. 12 On the other hand, there is no down time, and no incisions or scars. Additionally, the patient will look more like himself or herself after the procedure. The results are associated with a remarkable “natural look” which cannot be achieved by plastic surgery most of the time.
Conclusion and Summary
In this study, we retrospectively evaluated 46 patients treated with the 3D procedure, using patient and doctor satisfaction as the end point. Rhytids looked better and dyschromia was lessened in all of our patients, and this resulted in a more youthful and freshened appearance. Stretching of the skin, prominent decreases in solar dyschromia and pore width, and reduction of rhytids were achieved in five sessions performed over a 10-week period. Our results support the general outlook that the safety profile of the 3D procedure is very good in the presence of adequate physician training. The results obtained were as satisfactory as those that can be expected from any other modern technology device in this field.
Footnotes
Acknowledgments
None
Author Disclosure Statement
No competing financial interests exist.