
Abstract
Introduction
NaOCl is an effective irrigation solution against resistant endodontic microorganisms such as Enterococcus faecalis. 9 However, antibacterial agents may not affect microorganisms within deeper layers of dentin, because of their poor penetration depth. 10 Furthermore, bacteria such as E. faecalis have the ability to produce intra- and extraradicular biofilms that make their elimination difficult. 11 However, owing to the adjustable penetration depth of the laser irradiation, lasers can result in better access to complex regions of the root canal system that were inaccessible before. 12,13
Weichman and Johnson 14 were the first users of CO2 laser in endodontics to seal the apical foramen. Nd:YAG 15,16 and diode 17 –19 lasers, with their desirable disinfection properties, are widely accepted in endodontics. Also, erbium lasers such as Er:YAG and Er, Cr:YSGG lasers with water-absorption wavelengths of 2,940 and 2,780 nm, respectively, are suitable to remove dental hard tissues. When dental hard tissues are irradiated with laser, the water content evaporates, leading to a small burst in tissues along with minor thermal changes. Er, Cr:YSGG laser has thin and flexible endodontic fiber tips of various diameters and lengths to be used inside the root canals. 20
Previous studies have investigated the effect of various types of lasers on the eradication of E. faecalis. 21 –25 In a study carried out by Mehl et al., 26 the effect of Er:YAG laser was attributed to rapid evaporation of intracellular water, bacterial turgescence, thermal necrosis, and bacterial dehydration. Ramskold et al. 27 reported that using 15-s cycles of Nd:YAG laser with 15-s intervals does not increase the temperature and has no adverse effect on surrounding tissues. Moshonov et al. 28 used Nd:YAG laser at 4.5-W power and reported that NaOCl irrigation is still more effective than laser irradiation.
In most studies, low-power settings of this laser have been used to disinfect root canals without complete eradication of bacteria in infected root canals. 17,29 –32 Er, Cr:YSGG laser system is a new system that is effective in agitating a water irrigant in such a manner that the liquid cleans and shapes. The effect is believed to be athermal in nature; this would reduce the possibility of adverse temperature increase that might damage root canal dentin and cause irreversible tissue damage to the periodontal ligament. 33 –35 When dental hard tissues are irradiated by the Er, Cr:YSGG laser accompanied by water spray, not only is the temperature suppressed, but cutting efficiency also is increased. 36 Schoop et al. 31 concluded that the Er, Cr:YSGG laser has positive effect on E. faecalis because of a certain degree of the laser's light conduction within dentinal tubules in a higher penetration depth. They also reported that this laser removes the smear layer and debris from the root canal walls and opens the dentinal tubules' orifices. The aim of this study was to compare the effect of high-power settings of the Er, Cr:YSGG laser with that of NaOCl in reducing the number of E. faecalis in infected root canals.
Materials and Methods
Sixty freshly extracted maxillary central incisors with mature apices and straight roots were selected. Before the study, the teeth were stored in 3% chloramines T solution. Calculi and remnants of periodontal tissues were removed by ultrasonic devices. The teeth were decoronated by a disk (D&Z, Diamant, Germany) so that remaining root lengths were 12 mm; then the working length was established 1 mm short of the apical foramen by K-Flexofile 15 (Dentsply Maillefer, Ballaigues, Switzerland). Subsequently, no. 4, 3, 2, and 1 Gates Glidden drills (Dentsply Maillefer) were used to prepare the coronal third of the canals in a crown-down manner. Canal instrumentation was performed up to K-Flexofile 60 (Dentsply Maillefer) by using 0.9% saline as an irrigation solution. The smear layer was removed by the sequential use of 5.25% hypochlorite and 17% EDTA solutions for 3 min. 30
Bacterial inoculation
The teeth were sterilized in an autoclave at 121°C and a pressure of 15 psi for 20 min to remove all preexisting microorganisms. 30 To confirm sterility, the teeth were incubated in brain–heart infusion broth (Merck, Darmstadt, Germany) for 24 h at 37°C. Then each tooth was placed in a sterilized microtube. A pure bacterial culture of E. faecalis (ATCC 29212) was obtained from the Reference Laboratories of Iran Research Center, Tehran, Iran. Then the bacterial sample was subcultured to a brain–heart infusion agar (Merck) supplemented with 7% sheep blood (Baharafshan, Tehran, Iran) and incubated for 24 h at 37°C under aerobic condition. The grown and isolated colonies were then harvested and placed in Mueller-Hinton nutrient broth (Merck) and again incubated for 24 h at 37°C under aerobic condition. The E. faecalis culture in Mueller-Hinton nutrient broth was then calibrated to 2.5 × 108 colony-forming units per milliliter (CFU/mL) spectrophotometerically (the absorbance at 625 nm was between 0.11 to 0.13, roughly equivalent to the 0.8 MacFarland standard), which was confirmed by plate-count method; then 20 μL of the calibrated bacterial culture was transferred into the canal lumen of each tooth by using a sterile micropipette, and stored for 48 h at 37°C. Finally, all the canals were dried with sterile paper points.
Test groups
The teeth were randomly divided into four groups of 15 teeth each, as follows:
Group 1(the control group) was left untreated.
In group 2, Er, Cr:YSGG laser with a fixed repetition rate of 20 Hz, 2-W (100 mJ) output power, and 20% air and water levels was beamed into the canal by using a 200-μm-diameter Z2 fiber tip according to manufacturer's recommendations for canal sterilization (Biolase, Technology Inc., San Clemente, CA). This laser emits photons at a wavelength of 2,780 nm, and its pulse energy can be varied between 0 and 300 mJ. The fiber tip was inserted into the canals 1 mm short of the working length, and the laser was activated. Canal walls were irradiated by laser from the apical foramen to the coronal third. The total time of laser irradiation was 16 s in each canal, performed in two cycles of 8 s, with 30-s intervals between the two cycles.
In group 3, the laser was used in the same manner as in group 2 but at 3-W (150 mJ) output power. One percent NaOCl was used in group 4. The canals were irrigated with 1% NaOCl by using a 5-mL syringe and 21-gauge needles, and the irrigation was repeated at 5-min intervals. On the whole, 15 mL of NaOCl was used, and the total time of NaOCl contact with canal walls was 15 min. In a pilot study performed for the set-up of the study, keeping the teeth in a freezer for 1 h 30 was ineffective in saving the bacteria from thermal effects of dentin chip preparation. Therefore, all the teeth were kept in a freezer at −25°C overnight to avoid excessive heating of E. faecalis during drilling.
Disinfecting efficacy was determined by collecting dentin chips resulting from scraping the canal walls with no. 5 and 6 Gates Glidden drills (Dentsply Maillefer). The drills were inserted into the canals up to 1 mm short of the working length. A total of 10 mg of dentin chips from each canal was obtained and placed into microtubes, which were weighed before and during collection of dentin chips on an electronic weighing machine. The samples were then transferred to test tubes containing 2 mL of sterile normal saline and vortexed for 20 s; then serial 10-fold dilutions were prepared to a concentration of 10−7. Subsequently, 100 μL of each dilution was added to three Mueller-Hinton agar culture plates and incubated at 37°C for 48 h. After incubation, the number of the CFUs was counted on the plates. The mean number of CFUs for the three plates was calculated for the dilutions 10−2, 10−3 and 10−4. The resulting mean values were converted to the concentration of 10−3, summed, and then divided by three to obtain one CFU value for the laser-exposed samples and NaOCl and control groups.
The infected dentin was evaluated under an SEM before and after laser irradiation.
A Kolmogorov–Smirnov statistical test was used for testing normality for continuous variables. As the data were nonparametric, CFU values were subjected to a Kruskal-Wallis test for significant differences and the Mann-Whitney U test was used for group comparisons. Data were expressed as mean ± SD; p < 0.05 was considered statistically significant. All statistical procedures were performed by using SPSS Version 14.0 for Windows.
Results
The number of bacteria before and after laser irradiation and irrigation with NaOCl is presented in Table 1. The control group had the highest number of bacteria. In the NaOCl group, no bacteria grew on plates, and all the bacteria were eliminated. The results showed significant differences (χ2 = 31.97; p < 0.001) between the control group and the 2- and 3-W laser groups. According to the significant differences between the groups, the Mann-Whitney U test was used, and the results showed that in the control group (150 × 103 ± 18.9 × 103), significantly more grown bacteria were found compared with the 2- and 3-W laser groups (p < 0.001). No significant differences were noted between the 2-W (3.6 × 103 ± 1.7 × 103) and 3-W laser groups (2.3 × 103 ± 1.1 × 103) (p > 0.21).
SEM (VEGA II TESCAN, Cranberry, PA, USA) photomicrographs showed that before laser irradiation, the orifices of the dentinal tubules were open (Figs. 1 and 2). However, subsequent to Er, Cr:YSGG laser irradiation, the orifices of the dentinal tubules were partially or completely closed (Figs. 3 and 4).
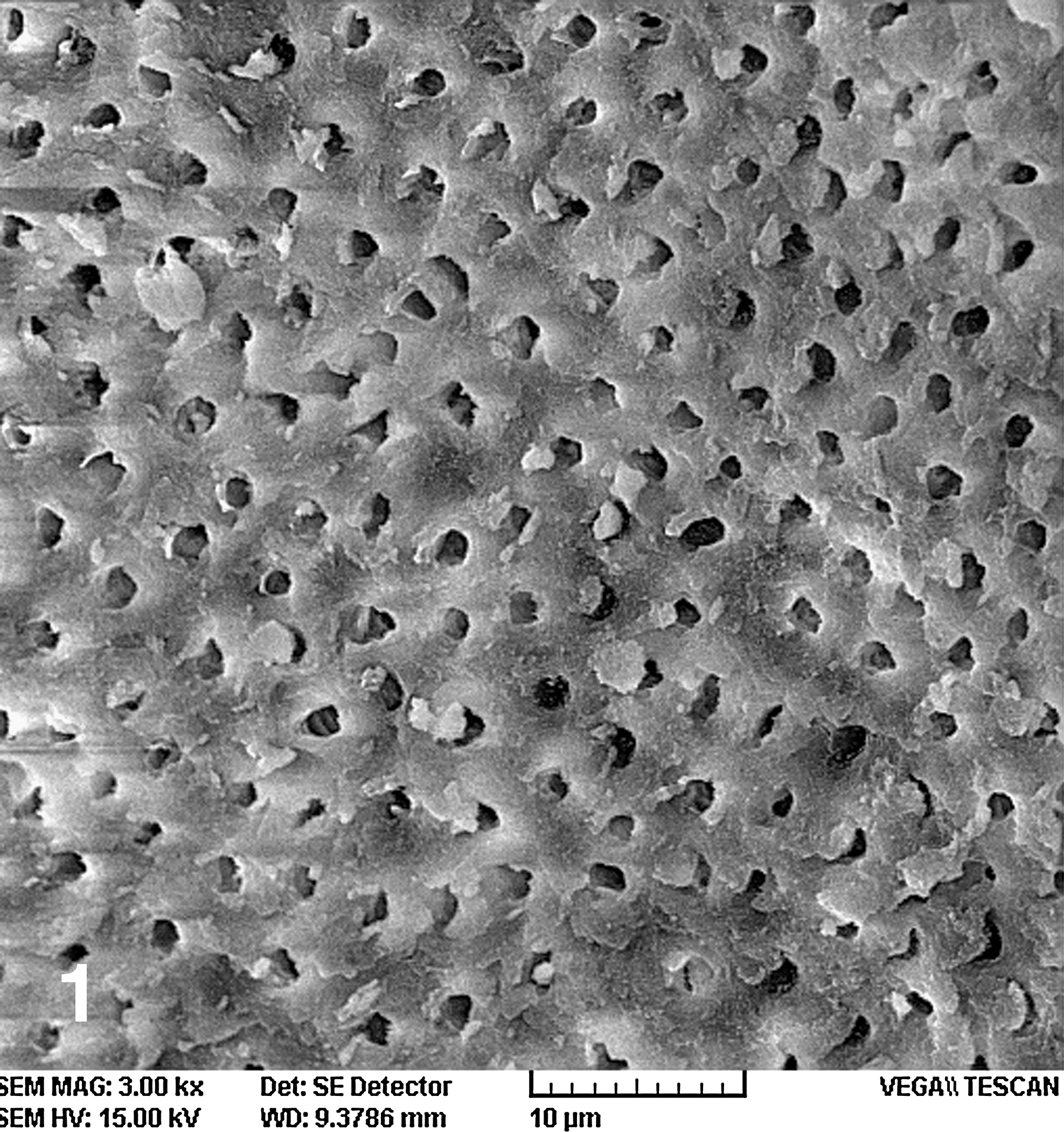
SEM images of infected dentin before Er, Cr:YSGG laser irradiation, group 1 (the control group); magnification, × 3,000.
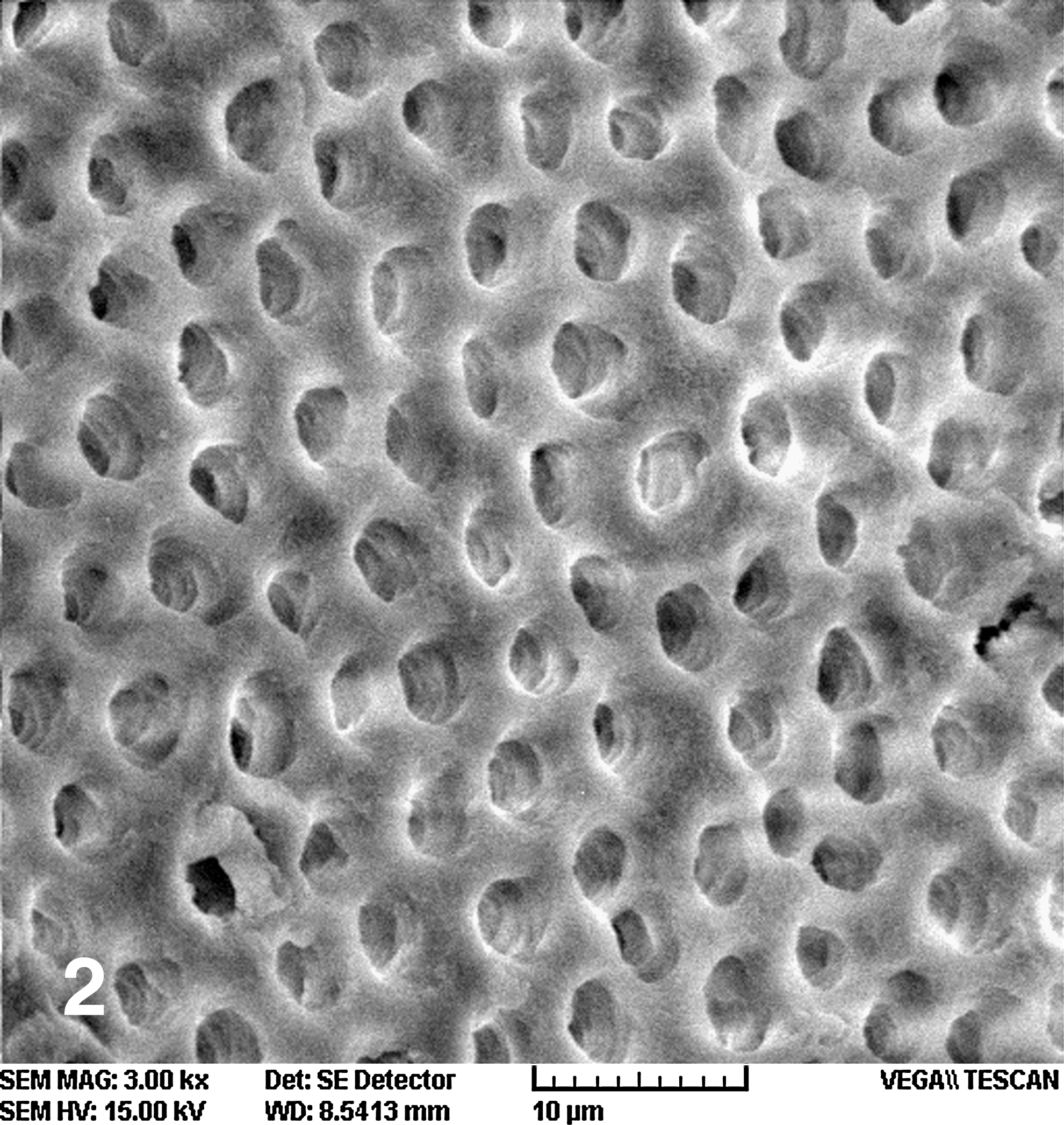
SEM images of infected dentin irradiated at an output power of 2 W by Er, Cr:YSGG laser, group 2; magnification, × 3,000.
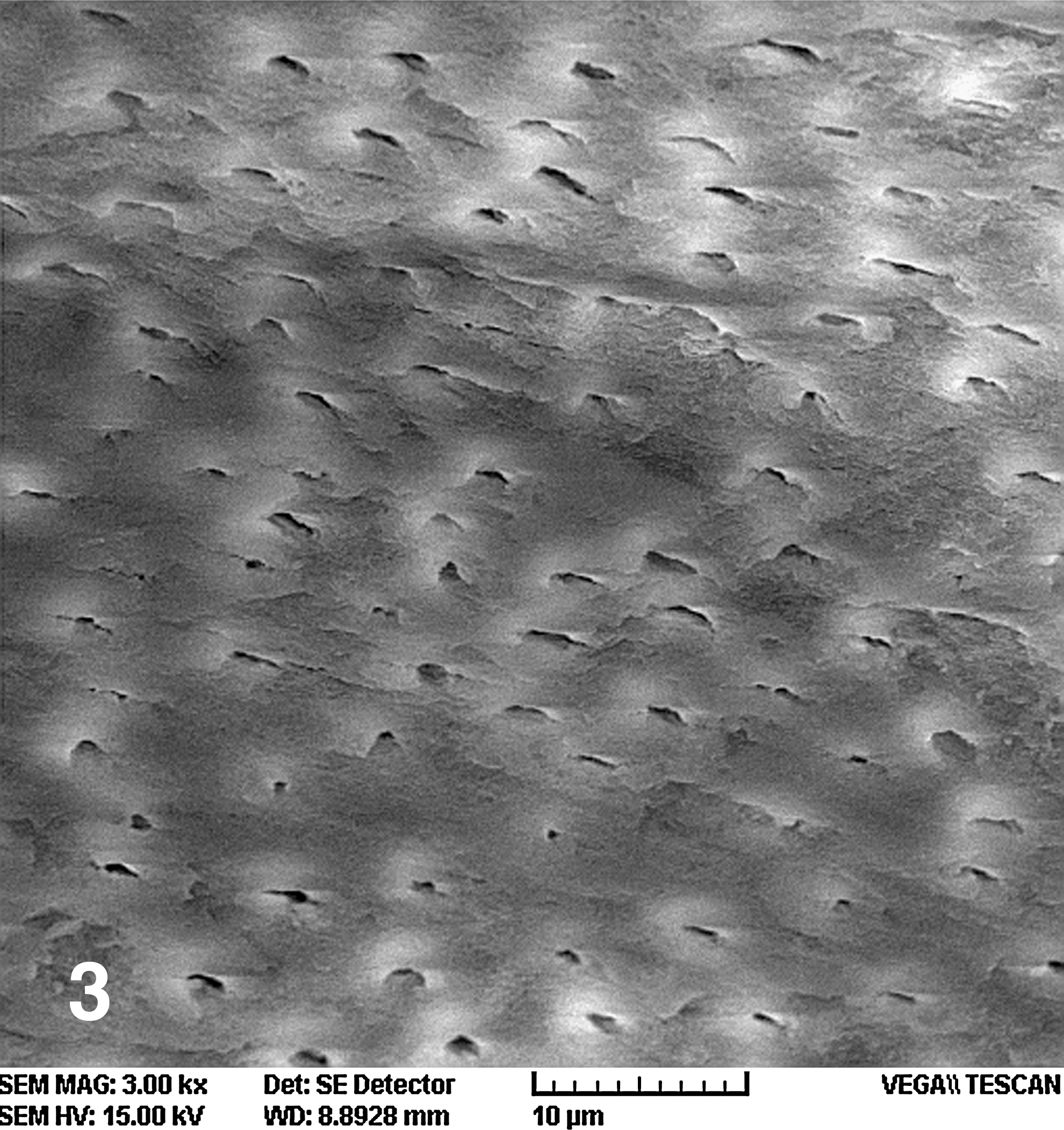
SEM images of infected dentin irradiated at an output power of 3 W by Er, Cr:YSGG laser, group 3, magnification, × 3,000.

SEM images of infected dentin before irradiation by Er, Cr:YSGG laser, group 4 (1% NaOCl); magnification, × 3,000.
Although 2- and 3-W output powers of Er, Cr:YSGG laser decreased the number of bacteria compared with the control group, they were unable to eliminate all the bacteria.
Discussion
E. faecalis is a microorganism found in failed root canal treatments and primary asymptomatic endodontic infections. 37 –39 Its high prevalence might be attributed to virulence factors, such as the ability to compete with other microorganisms, invasion to dentinal tubules, adhesion to collagen, and resistance against unfavorable nutritional conditions.
In the present study, E. faecalis samples were incubated with teeth for 48 h to use cells in the starvation phase rather than to use growing cells. This helped better simulate in vivo conditions, which would have a limited amount of nutrients available in the root canal. 40 During the experiments, the E. faecalis strains remained in the root canals for 48 h, grew, and contaminated the tubules, which is consistent with the results of studies by Moshonov et al., 28 Schoop et al., 31 and Siqueira et al., 41 using scanning electron microscopy, by Raucci-Neto et al., 42 by using light microscopy, and by Sedgley et al. 43 by using Brown and Brenn histologic staining.
The root canals of the teeth were cleaned and shaped; then the teeth were autoclaved and incubated with E. faecalis for 48 h, which is too short a time for bacterial biofilm to form within root canals. 44 According to Kishen et al., 44 bacterial biofilm shows the ability of microorganisms, especially E. faecalis, to form a calcified layer on root canal dentin and extraradicular regions, as evidenced by an increase in the carbonate and phosphate bands within 4–8 weeks, and may act as a factor contributing to their persistence after endodontic treatment.
In this study, a sampling procedure involving the scraping of the canal walls was used because grinding and culturing of dentin gave better quantitative information about the extent of the infection, and the teeth were kept in a freezer for cooling before sampling to avoid killing E. faecalis because of the heat from the drills during the sample-collection procedure.
In the present study, the antibacterial effect of the Er, Cr:YSGG laser was studied because it has the ability to reduce the number of E. faecalis and to remove the smear layer and debris. 31 This laser is newly marketed and is less harmful than other laser systems for hard tissues. 36 The antibacterial effect of Er, Cr:YSGG laser on intracanal bacterial count reduction has been investigated in a number of studies. Schoop et al. 31 used Er, Cr: YSGG laser at 1.5- and 2.5-W powers without air and water, significantly decreasing intracanal bacterial counts compared with a control group. These effects were compared with a situation in which no irrigation solutions were used. Eldeniz et al. 30 compared the effects of Er, Cr: YSGG laser on E. faecalis with irrigation with 3% NaOCl and reported that Er, Cr:YSGG laser with 0.5-W power and 20% air and water levels decreases the number of viable intracanal bacteria ≤ 4.3% compared with the control group but does not entirely eliminate them. In contrast, they also reported that 3% NaOCl inhibits E. faecalis growth and sterilizes the canals. Regarding the bactericidal effects of Nd:YAG and Er, Cr:YSGG laser with 1- and 1.5-W powers, and 2.5% NaOCl on E. faecalis, Wang et al. 32 reported that unlike the applied lasers, NaOCl completely eliminates all bacteria. Nd:YAG laser demonstrated better performance compared with the Er, Cr:YSGG laser. With the Er, Cr:YSGG laser, the bacterial load decreased to 23% at 1-W power, and to 4% at 1.5-W power in comparison with a control group. The applied powers did not demonstrate any significant differences in their antibacterial effects.
In the present study, the number of bacteria decreased similarly. Er, Cr:YSGG laser at 2- and 3-W output powers reduced the number of bacteria to 2.4% and 1.53% of the control group, respectively, and the reduction of bacterial load was not significantly different between these groups. Similar to studies carried out by Eldeniz et al., 30 Wang et al., 32 Moshonov et al., 28 and Piccolomini et al., 45 lack of bacterial growth was observed in all the specimens in the NaOCl group. It has been shown that deep dentin laser irradiation results in irregular surfaces with microcracks, removes a large amount of intertubular dentin, and leaves the peritubular dentin with protruding tubules. In contrast, in superficial dentin, it produces flat surfaces and similarly removes both intertubular and peritubular dentin at the same energy levels. 42
The inability of the Er, Cr:YSGG laser in eliminating all the bacteria may be attributed to deep penetration of bacteria into dentinal tubules, protecting them from the effect of laser irradiation. 44,46 E. faecalis shows more resistance against unfavorable conditions in starvation phase. 41 Another factor contributing to the inability of laser to eliminate all the bacteria completely may be uneven irradiation of all the surfaces of root canal walls and probably the presence of nonirradiated areas on the root canal wall.
It is necessary to perform SEM and histologic studies to determine the penetration depth of the Er, Cr:YSGG laser, bacterial penetration in the dentinal tubules, and their superficial eradication by the Er, Cr:YSGG laser to confirm the antibacterial effects of the Er, Cr:YSGG laser in endodontic treatment.
Conclusion
According to the results of the present study, the 2- and 3-W output powers of Er, Cr:YSGG laser have antibacterial effects on E. faecalis in root canals of infected teeth; however, their effect is less remarkable than that of a NaOCl solution.
Footnotes
Acknowledgments
We thank the Office of Vice Chancellor for Research, Tabriz University of Medical Sciences, for supporting this research study financially.
Author Disclosure Statement
No competing financial interests exist.