
Abstract
Introduction
Low-level laser therapy (LLLT) has been used clinically since the first successful cases reported by Professor Andre Mester and colleagues. 5,6 Cameron 7 reported that the frequency of the laser light, as well as the type tissue being irradiated, determines the depth to which light penetrates. Laser light with wavelengths of between 600 and 1,300 nm optimizes the depth of penetration in human tissue at 1 to 4 mm and is therefore most frequently used in the clinical setting. Laser light with a longer wavelength, such as the (infrared) diode produced by the gallium arsenide (Ga–As) or gallium aluminum arsenide (Ga–Al–As) lasers penetrates more deeply, 8 whereas laser light with a shorter wave length, such as red light produced by the He–Ne laser penetrates human skin very superficially. Research findings have shown that 99% of low-level laser is absorbed in the superficial 3.6 mm of human skin. 7
Studies on the influence of continuous-wavelength diode lasers on burn healing have been few and have shown inconsistent results. 8 –12 Although Cambier et al., 8 Schlager et al., 9,10 and Al-Watban and Delgado 11 reported that irradiation of burns with different wave lengths, powers, and energy densities produced no beneficial effects on the wound-healing process, Meirele et al., 12 in a recent study, indicated that 660-nm laser was effective for improving the healing of third-degree burns in diabetic rats. Baxter 13 reported that, although a large percentage of the (diode) low-level laser instruments used in clinical practice are continuous-wave output, most units currently available in the United Kingdom allow some forms of pulsing of their output for pulsed units. The application of frequency is growing rapidly, and a review of the literature showed several cellular studies, 14 –16 an in vitro model of a fetal mouse limb growth, 17 and three clinical trials 18 –20 would suggest that this parameter be critical to at least some biologic and medical effects of this parameter. Thawer et al. 17 investigated the effects of a 904-nanometer Ga–As laser on the growth and development of fetal limb tissue. Thawer et al. 17 found that there was an increase of dermal cell number and collagen-fiber thickness after administration of lower frequencies of laser (500 and 3,000 Hz). These frequencies of laser also produced a greater amount of dermal collagen. In another study, Karu et al. 21 investigated the effects of a 1,300-nm continuous-wave laser diode and a 950-nm modulated superluminous diode laser, which had frequencies of 2, 26, 700, 1,000, and 5,000 Hz. With both diodes, their effects on the rate of Escherichia coli, WP2 division, were examined. They mentioned that their results indicate that one of the critical parameters of laser irradiation when acting on living cells is the pulse duration and/or the frequency. 2
A review of the literature has revealed that no study regarded the effect of pulsed-wave LLLT on the deep second-degree burn healing process. Conversely, several studies reported the effects of pulsed diode lasers on skin-wound healing. 22 –24 Al-Watban and Zhang 22 evaluated the effects of pulsed continuous wave (PCW) and detected the role of wound healing in rats by using both pulsed and CW LLLT. They reported that the percentage of relative wound healing was 4.32 in 100 Hz, 3.21 in 200 Hz, 3.83 in 300 Hz, 2.22 in 400 Hz,1.73 in 500 Hz, and 4.81 in CW. They concluded that LLLT using pulsed CW laser at appropriate dosimetry and frequency can provide acceleration in wound healing in rats. The 100-Hz frequency had a better effect than other pulse frequencies used in the study. The effects of treatment with the CW laser were greater than the pulse frequency. The frequency of pulsed CW laser was not found to increase wound healing in rats compared with normal CW laser.
Recently, Demir et al. 23 investigated the effects of electrical stimulation and laser treatment on wound healing in rats. They concluded that electrical current and laser treatment both have beneficial effects during the inflammation, proliferation, and maturation phases of a wound. More recently, Matic et al. 24 made a rectangular defect of all skin layers at the dorsal part of the rat neck under general anesthesia. They used an 890-nm wavelength of the semiconductor laser. It was of pulsed character with a frequency of 1,500 Hz and impulse duration of 300 nsec. They found that decrease of the average surface area of the wounds in the laser-treated group was significantly higher than that of control group.
However, the benefits of pulsed diode lasers in wound healing are still controversial, and many other investigators found no improvement in wound-healing processes. 25,26 Because of these contradictory results, no consensus exists of the effects of LLLT in the wound-healing process. Recent skin wound-healing and burn-healing studies have used various diode lasers with different wave lengths, laser powers, and stimulated doses. Concerning the type of laser and the sufficiency of the wavelength, no clear recommendation can be made. Conversely, the low-level pulsed diode laser has not yet been examined in deep second-degree burn-healing treatment. The recent investigations contain no deep second-degree burn healing for a 890-nm infrared diode laser with a 3,000-Hz frequency. Therefore, the aim of the present study was to examine the influence of LLLT by using a 3,000 Hz–pulsed infrared diode on the healing of deep second-degree burns in rat. Infection is a major cause of morbidity and mortality in burns, 29,30 so we also examined microbial flora of the burns.
Materials and Methods
Animals and study design
Seventy-seven adult male Wistar rats, 4 months old, weighing 250 ± 30 g, were used in this study. They were provided with food and water ad libitum. Rats were divided into groups 1, 2, 3, and 4. Two deep second-degree burns were made at the proximal and distal parts of the dorsal skin of the thoracic region of each rat (Fig. 1). The proximal burn was considered the experimental burn. The distal burn was considered the control burn. The proximal burn of group 1 was treated with LLLT with the radiating head, without switching on the machine, and was considered the placebo group. Proximal burn of groups 2 and 3 were treated with two different energy densities of infrared diode lasers, so no differences existed between groups 2 and 3 and group 1, except LLLT. The proximal burn of group 4 was treated 3 times per week with topical application of nitrofurazone 0.2% (Iran Nago Pharmaceutical Co., Tehran, Iran) over the course of the study. Treatment was started in all groups immediately after burning. Distal burns of all rats were considered their relevant control burn. All burn wounds were examined macroscopically and microbiologically. Table 1 shows the distribution of the rats in study groups.

Diagram of location of burns: P, proximal; D, distal.
Systemic effects of LLLT have been reported by the study of Rochkind et al. 27 Khadra et al. 28 have speculated that LLLT can stimulate the release of substances such as growth factors and cytokines into circulatory system, and so could affect the untreated side of an experimental animal or subject. To ascertain the possibility that laser treatment of a proximal burn might influence healing of the distal burn thorough a systemic effect, we conducted separate experiments by dividing rats into placebo and treatment groups. Laser treatment was applied at 2.3 and 11.7 J/cm2 to the laser-treated groups, and probable systemic effects of LLLT were compared against the healing of placebo rats receiving no laser treatment.
Burning of animals
On day zero, all rats were anesthetized with 50 mg/kg ketamine hydrochloride, injected intramuscularly along with 5 mg/kg diazepam. The dorsal hair of the thoracic region of rats was shaved and cleaned with povidone–iodine. Each rat was kept in a special box that had a 3 × 3-cm hole. At first, the proximal part and then the distal part of the thoracic region of each rat was exposed separately to the external tip of a 5-cm-long cylinder, 22 mm in diameter, and connected to a source (kettle) of boiling water with a 5-L capacity for 3 sec (Fig. 1). A pilot study was performed, and our previous study using histologic examination revealed that the epidermis and most of the dermis were burned. 31 The burned skin was 3.8 cm2 in area. 31 All procedures were approved by Medical Ethics Committee of Shahid Beheshti University, M C.
Treatment
Proximal burn of groups 2 and 3 were exposed to a pulsed infrared laser (MUSTANG 2000 with L07 radiating head made by Technica Co., Moscow, Russia). The specifications of the laser are shown in Table 2. LLLT began immediately after burning. To administer laser irradiation, the burned area and normal surrounding skin were divided into eight equal squares (1 × 1 cm) with the tip of the laser source ∼5 mm above the skin of the center of each square, directing it perpendicular to the target tissue for the designated time (that is, 62 sec for group 2 and 310 sec for group 3. 32 It is notable that LLLT was restricted to 3 times per week. The duration of LLLT was 1 J/cm2 energy density per day for group 2, and 5 J/cm2 energy density per day for group 3 at each point (center of square) for 7 days were calculated, and then the time was divided by three, so there was 2.3 J/cm2 energy density for group 2 and 11.7 J/cm2 energy density for group 3.
Microbiologic examination
On days 7, 15, and 30, microbiologic samples were taken from the burned skin of rats. Swabs were taken from burns under anesthesia. The samples were cultured and tested for identification of Staphylococcus epidermidis, S. aureus, S. saprophyticus, Subtilis, Lactobacillus, Diphtheria, and Pseudomonas aeruginosa by using the routine methods of microbiology originally described by Fingold and Martin, 33 Baron and Fingold, 34 and Brook et al. 35 The number of rats in each microbiologic group is shown in Table 3. The data for each microorganism were compared between proximal burns of study groups and between proximal and distal burns of each group by using the χ2 test. Colony-forming units (CFUs) of each sample were counted semiquantitatively. The data of distal burns and proximal burn of rats and the data of proximal burns of groups were compared by independent-sample Student's t test. The data are expressed as mean ± SD. A value of p ≤ 0.05 was considered statistically significant.
Clinical examination of burn size
Images of the burn area of group C rats were taken by a digital camera (5-megapixel Canon Power Shot G6 digital camera, Osaka, Japan), and the surface was measured with Adobe Photoshop (AP) CS3 extended (Version 10.0) Image. An image of each rat was taken 5 times on days 0, 7, 14, 21, and 28. For measuring the burn area, the image was put on a grid. The image was equally divided into four regions (1, 2, 3, and 4). The holes of all regions that were completely occupied by the burn were counted. The holes of No. 1 and No. 3 regions that were partially occupied by the burn were counted as well. The holes of No. 2 and No. 4 regions that were partially occupied by the burn were not counted.
The percentage wound size was calculated by using the following formula:
where S 0 is the surface area of the wound on day 0, and Sn is the surface area of the wound on the indicated day. 36
The surface area of two burns in each rat was compared by using independent-sample Student's t test. The surface area of placebo and laser-treated burns and nitrofurazone-treated burns of the study groups were analyzed by using ANOVA in each week and between each group. All data are expressed as mean ± SD. Statistical significance was set at p ≤ 0.05.
Results
Microbiologic examination
Statistical analysis of the incidence of microbial flora is shown in Table 3. Bacillus subtilis was found in an experimental burn of one rat of group two (one of six) in comparison with the three rats of group one (three of six) on day 7. A significant difference was found between group one and group two (χ2 test, p = 0.046). No trace of Bacillus subtilis was found in the experimental burns of groups 3 and 4 on day 15, whereas experimental burns of three rats of group 2 (three of six) exhibited Bacillus subtilis. A significant difference was found between groups 3 and 4 and group 2 (χ2 test, p = 0.033, p = 0.046, respectively). Staphylococcus aureus was not found in experimental burns of group 3 on day 28, but it was found in experimental burn of three rats of group 1 (three of seven) (χ2 test, p = 0.05).
Results of CFU count
Statistical analysis of the incidence of CFU-count flora is shown in Figs. 2, 3, and 4. No significant differences were noted in the incidence of CFU-count flora within groups and between groups.
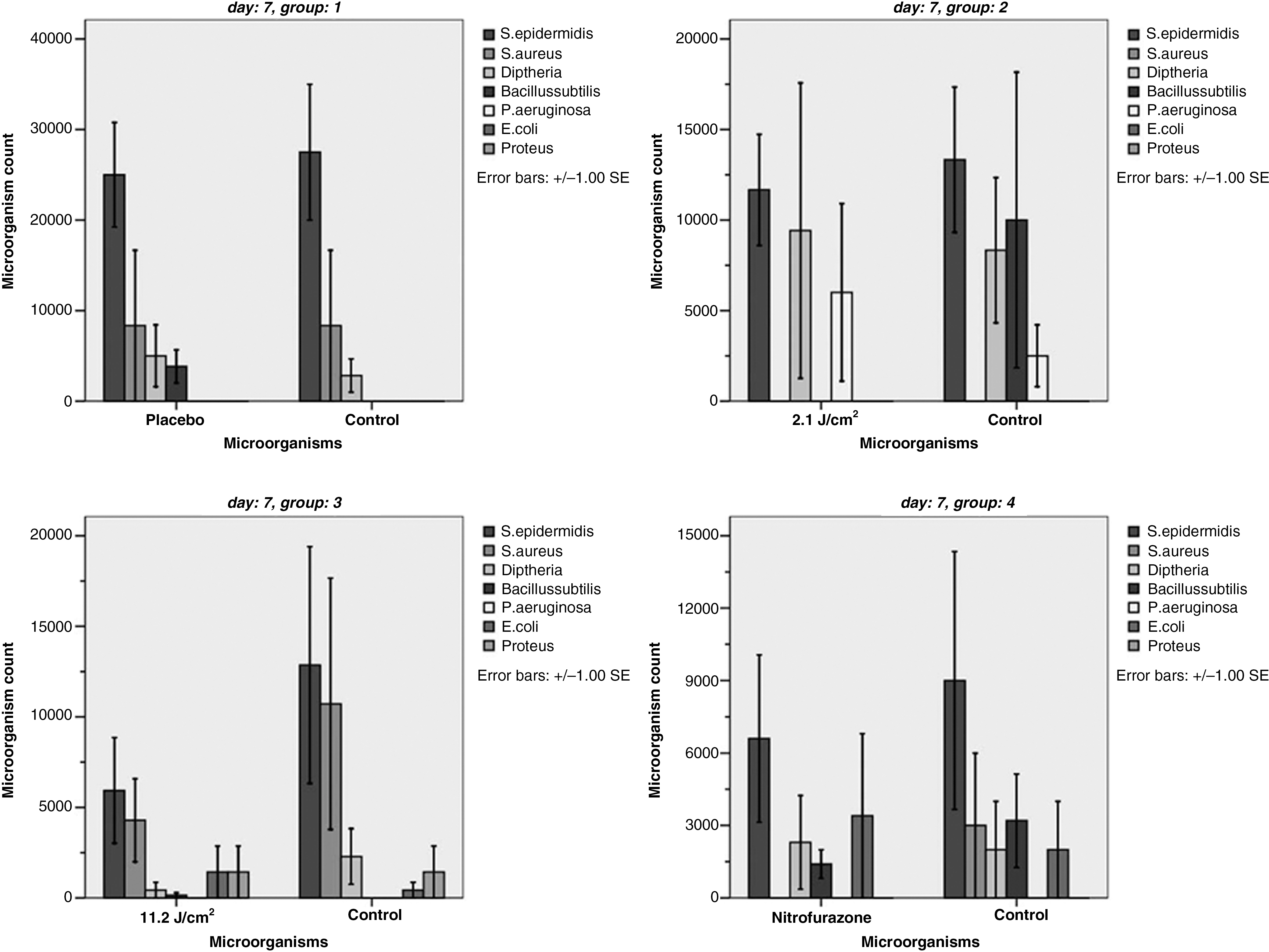
Mean ± SD of microorganism counts of study groups on day 7. No significant differences were found of the incidence of CFU-count flora within groups and between groups.
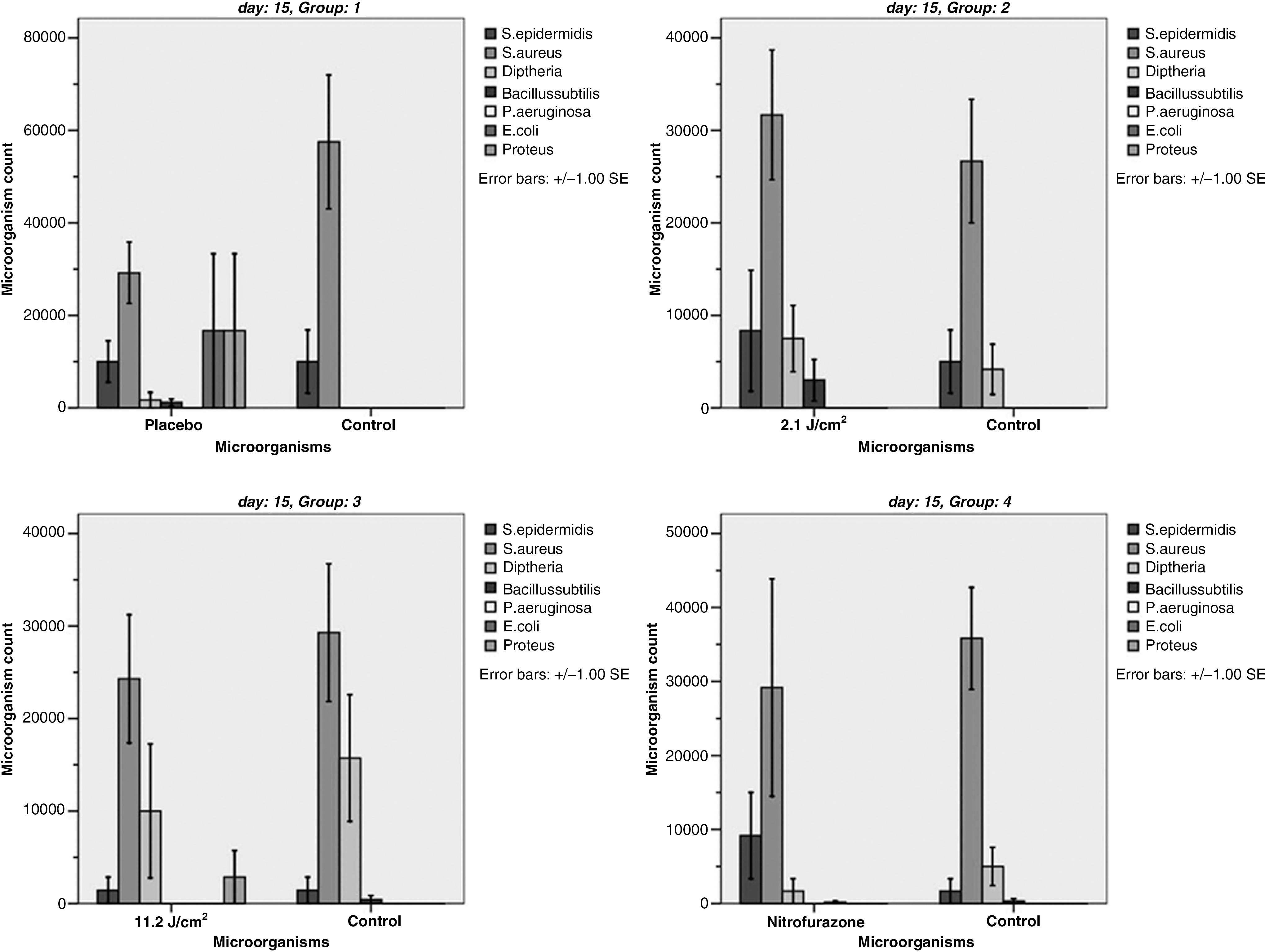
Mean ± SD of microorganism counts of study groups on day 15. No significant differences were found of the incidence of CFU-count flora within groups and between groups.

Mean ± SD of microorganism counts of study groups on day 28. No significant differences of the incidence of CFU-count flora were found within groups and between groups.
Clinical examination
Statistical analysis of the wound-closure examination is shown in Fig. 5. The results of statistical analysis of between groups at each week are classified into week 1, weeks 2 and 3, and week 4.

Wound-closure rate represented as a percentage of the wound size after burn induction at sequential intervals. Analysis of variance showed that LLLT with 11.7 J/cm2 significantly increased the wound-closure rate 2 weeks (0.915 ± 0.310) and 3 weeks (0.677 ± 0.397) after burning, compared with placebo burns of group 1 (1.413 ± 0.319, 1.116 ± 0.436, respectively; ANOVA, LSD test; p = 0.045 and p = 0.046, respectively). Significant increases of wound-closure rates of laser-treated burns of group 3 were noted in comparison with laser- treated burns of group 2 (p = 0.044). Independent-sample t test showed that LLLT with 11.7 J/cm2 significantly increased the wound-closure rate of the experimental burns of group 4, at 4 weeks after burning (0.211 ± 0.146) compared with the control burns (0.707 ± 0.480; p = 0.039). Significant increases of the wound-closure rates of nitrofurazone-treated burns were seen in comparison with the control burn (p = 0.016).
The results of statistical analysis within each group at sequential intervals are classified into weeks 1, 2, and 3, and week 4.
ANOVA test showed significant differences within each group between sequential intervals in most cases (ANOVA test, p < 0.05) except the following cases: Day 0 and week 1, and also week 1 and week 2 in all groups. Weeks 2 and 3, as well as weeks 3 and 4 in group 1. Weeks 3 and 4 in group 2. Weeks 2 and 3 in group 3 (Fig. 5).
Discussion
Despite the failure of some studies 8 –11 to show beneficial effects of low-level diode lasers on burn healing on healthy and normal animals, the present investigation for the first time demonstrated that pulsed-wave LLLT can significantly accelerate the wound-closure rate of a deep second-degree burn model in normal and healthy rats.
The biostimulatory effect of pulsed LLLT in the current study is demonstrated by the significant increase of the wound-closure rate of laser-treated burns in comparison with the placebo group at 2, 3, and 4 weeks after burning, whereas nitrofurazone-treated burns showed a significant increase of the wound-closure rate compared with placebo burns only 3 weeks after burning. It seems that LLLT was more effective than nitrofurazone ointment in the healing of a third-degree burn model. LLLT, when used appropriately, can stimulate the healing of injured tissue as it does that of the dermis. 37 Investigations into mechanisms involved have shown that many of type of cells whose interaction results in dermal repair can be affected in a therapeutically advantageous manner by treatment with LLLT both in vitro and in vivo. Mast cells and macrophages can be stimulated to release growth factors and other substances, and the proliferation of fibroblasts, endothelial cells, and keratinocytes maintained in adverse conditions can also be stimulated. The development of granulation tissue is mainly controlled by the growth factor released from macrophages. 37
In present investigation, we could not find that the effects of 2.3 J/cm2 LLLT of the deep second-degree burn healing process compared with its control burns. One proposed mechanism by which LLLT stimulates the wound-healing process is by absorption of light energy by mitochondria, which increases cell energy and stimulates the release of chemical mediators. 38 –40 It would appear that such a mechanism did not occur in the 2.3 J/cm2 laser-treated burns of the present study, as well as in the studies of Cambier et al., 8 Schlager et al., 9,10 and Al-Watban and Delgado. 11 This may be due to insufficient light energy reaching the cells. Allendorf et al. 41 suggested that laser-light penetrations of tissue and eschar debridement might be concerned within wound healing. Wounds that are not debrided, such as wounds in the current study, may not allow the maximal amount of light to reach the tissue. Our results suggest that pulsed LLLT at a dosage of 11.7 J/cm2 produces a significant increase in the wound-closure rate and confirms the findings of Matic et al. 24 that pulsed LLLT significantly accelerated the wound-closure rate of a surgically induced cutaneous wound. Whereas the results of present study and of the study of Matic et al. confirmed the positive effect of pulsed LLLT on burns and acute skin wounds, other studies failed to show a positive effect of pulsed LLLT on the impaired wound-healing process. 25,26 By using a Ga Al As 890-nm multidiode (n = 60) array unit (270 Hz; maximum rated output, 300 mW), Lowe et al. 26 examined wound healing in mice that had been exposed to x-ray irradiation. They found that although wounds treated with X-ray irradiation showed delayed wound healing, treatment with 890-nm light therapy did not have a significant effect on wound closure at doses of 0.18 and 0.54 J/cm2 and only further delayed wound healing at a dose of 1.54 J/cm2. Using a similar animal model of radiation-impaired wound healing in mice, Walker and colleagues 26 found no hastening in wound healing with 660-nm Ga Al As laser (5 kHz; 15 mW 0.5, 1.5, and 4 J/cm2 for three groups).
The statistically significant difference was found in the wound-closure rate of burns between the laser-treated (proximal) burn of group 3 and the placebo burn (distal) of group 1, 2 and 3 weeks after burning. These results of current study are in agreement with those of the Reddy et al. 42,43 studies. Reddy et al., in their first study, made two wounds in each streptozotocin-induced diabetic (STZ-D) rat. The left wound in each animal was treated with an He-Ne laser. Measurement of the biomechanical and biochemical properties of the laser-treated wounds indicated a significant increase in maximal load and soluble and insoluble collagen in laser-treated wounds compared with control wounds. Reddy et al. reported that the results of their pilot study and also the main part of their study indicated that laser treatment had no systemic effects on the contralateral wound healing. The left wound of each animal was treated with infrared radiation. The right wound served as control. The results from the biomechanical analysis indicated that the laser used in the study significantly increased the tensile strain and toughness compared with the control wound. Reddy et al., in another study, 43 used the same animal model and also the wounding model. Reddy did not report a systemic effect of laser treatment on contralateral wounds, so, based on the results of current study and those of Reddy et al., 42,43 we conclude that LLLT had no systemic effects on contralateral wound healing. However, Rochkind et al..27 reported that irradiation of low-power laser on a crushed injured sciatic nerve in the right leg in a bilaterally inflicted crush injury significantly increased the compound action potential in the left nonirradiated leg as well.
Although most bacterial infections of the skin prove to be minor, a few such dermatologic entities are significant, to the point of being fatal. Their course can be extremely rapid and will lead to dreadful complications. The mortality rate is usually up to 30–50% and depends on the type of infection, underlying disease, and immune status. Patients usually need to be hospitalized, sometimes in intensive care or burn units. They should be treated systemically with appropriate antimicrobial therapy plus aggressive supportive care. 44 Conversely, Robson 45 reported that wound infection can be viewed as a failure of wound healing caused by an imbalance of bacteria.
Microbiologic examination showed few pathogenic microorganisms in the control burns; however, pulsed LLLT decreased significantly the incidences of S. aureus and Bacillus subtilis compared with group 1 (placebo burns). The current results provide little evidence of an inhibitory effect of pulsed LLLT on microbial flora of a deep second-degree burn model.
It may be beneficial to examine the burns by histologic methods to detect differences between study groups at the cellular level; therefore, further histologic studies are suggested.
We conclude that irradiation of a deep second-degree burn model with a 11.7 J/cm2/890 nm pulsed low-level laser in rat significantly increased the wound-closure rate compared with control burns, and the inhibitory effect of the LLLT on microbial flora of the burn was minimal.
Footnotes
Acknowledgments
We thank Mrs. Jamileh Rezaei; we also thank Mrs. Habibie for her assistance in microbiologic examination, and we thank the Vice Chancellor of Research of Shaheed Beheshti University, M.C., for financial support.
Author Disclosure Statement
No conflicting financial interests exist.