
Abstract
Introduction
The laser has been used in dentistry for several decades. After Nd:YAG laser was first used by Stern et al. 7 to irradiate the surfaces of enamel and dentine in 1964, various lasers were rapidly applied to treat oral diseases, such as in removing soft tissue, increasing acid resistance, sterilizing root canals, and the treatment of dental desensitization, superficial caries, oral ulcers, and other oral mucosal diseases. 8 –10 However, it was rarely reported that lasers were applied to pretreat dentine surfaces before bonding.
In our previous study, we investigated the thermal and morphologic effects of pulse Nd:YAG laser on root-canal surfaces and found that the smear layer was removed efficiently by laser irradiation. 11 Other morphologic studies also reported that irregular honeycombs or craters were observed in the laser-irradiated area of enamel or dentine under scanning electronic microscopy (SEM), and the smear layer was removed. 12 –14 The melting and recrystallizing effect of laser irradiation caused rough dentine surfaces and orifices of dentinal tubules, sealed or partly sealed. The hypothesis was proposed that this roughness might offer more microspace for resin monomers to penetrate and form more resin tags, which might increase the bond strength of resin to dentine.
Therefore, pulse Nd:YAG laser was used to pretreat the human dentine surface before bonding in this study. The optimal laser-parameter combination was determined first and then compared with other surface pretreatment methods to investigate the effect of pulse Nd:YAG laser on human dentine adhesion.
Materials and Methods
Two-hundred ten caries-free, freshly extracted (due to orthodontic treatment) human premolars were collected after approval from the IRB. The teeth were immediately cleaned and stored at 40C in a distilled phosphate-buffered solution, which was changed every other day. All teeth were used within 2 months. To optimize the laser-parameter combination, 90 teeth were used and randomly divided into nine groups, as shown in Table 1. The other teeth were randomly divided into six groups: laser-irradiated group, acid-etched group, laser + acid group, 10-3 solution (10% citric acid and 3% ferric chloride) group, laser + 10-3 solution group, and negative control (unconditioned) group. Each group had 20 specimens: 10 for tensile-bond strength tests, and the other 10 for microleakage examination. The detailed treatments are shown in Table 2.
N = 10. The labeled groups showed statistical significance. (a p < 0.01: group 2 versus other groups; b p < 0.05: group 7 versus groups 1, 3, 5, and 6).
The labeled groups showed significant difference.
p < 0.05, the labeled groups versus other three groups; b p < 0.05, the labeled group versus all of the other groups.
The teeth used for the tensile-bond strength test were prepared as follows: first, the teeth were embedded in the self-cured acrylic resin (Shanghai Dental Factory, Shanghai, China); then buccal enamel was removed with a low-speed cutting machine (MF-PERFECTA, Burmoos, Austria) under water coolant; a flat dentine surface (more than 4 × 4 mm2) was obtained. Second, the dentine surface was polished with 200-, 400-, and 600-grit silicon carbide abrasive paper, and a thin paper with a 4 × 4-mm2 hole was fixed on each specimen. Finally, the exposed dentine surface was prepared as shown in Tables 1 and 2. The specimens of laser-irradiated groups were irradiated with pulse Nd:YAG laser (Friendly A4.0, Milan, Italy) in a scanning mode, each for 15 s. The laseroptic fiber (320 μm) was used in a standard position: perpendicular to the dental surface and ∼1 mm. The Single Bond primer (3M, Minneapolis, MN) was brushed onto dentine surface and light-cured for 10 s with a Halogen Curing Light (Elipar 2500; 3M ESPE) with a light intensity of 800 mW/cm. The Restorative Z100 Resin (3M) was applied to make a cone-shaped resin column (bottom >4 × 4 mm, about 4 mm high) and light-cured for 40 s on each side for 10 s. All the specimens were immersed in distilled water for 24 h at 370C.
The universal testing machine (WDW-10; Panasonic, Osaka, Japan) was used for the tensile-bond strength test in this study. Each specimen was mounted in the machine, and tensile force was applied to it through the self-made clamps, at a constant speed of 0.5 mm/min. The force value (N) recorded at the failure point was divided by exposed dentine surface (16 mm2) and converted to tensile-bond strength (1 Mpa = 1 N/mm2).
The fractured surface was examined under the stereomicroscope (10 × ), and the fracture pattern was assessed by the Adhesive Remnant Index (ARI), which is based on the remaining resin amount on the dentine surface (ARI score: 0, no resin left; 1, little resin left; 2, resin covering less than half of the bonding surface; 3, resin covering more than half of the bonding surface; 4, resin covering the whole bonding surface). 15 Then the fractured surface was dehydrated by serial ascending graded alcohol solutions, sputter-coated with gold, and examined under an SEM (Jeol JMS 5200; Tokyo, Japan).
Sixty teeth used for microleakage experiments were prepared with a class V cavity (∼4 mm long, 4 mm wide, and 2 mm deep) in the buccal surface, and the cavity walls were perpendicular to the dental surface. The gingival margin was ∼1 mm below the cemento-enamel junction, and the treatments were the same as the bond-strength test (Table 2). The same resin was placed just as one increment and light-cured, as described. All specimens were thermocycled between 40C and 600C for 24 h, with a staying time of 60 s (∼720 cycles). Before immersion in dye, apices of teeth were sealed with zinc oxide eugenol cement, and the dental surfaces outside 1 mm to the restoration margin were coated with nail polish. The specimens were immersed in 1% methylene blue solution for 90 min and then rinsed and sectioned longitudinally. The interface was observed under the stereomicroscope (10 × ), and the microleakage was assessed by the microleakage score (0, no microleakage; 1, microleakage less than half of the cavity wall; 2, microleakage more than half of the cavity wall; 3, microleakage reaching the cavity bottom; and 4, microleakage reaching the dental pulp).
The data were analyzed with SPSS 13.0 software. A one-way analysis of variance (ANOVA) was used to determine whether a significant difference existed between the experimental groups on tensile-bond strength. The Pearson χ2 Test was used to analyze the frequencies of different groups in ARI and microleakage scores.
Results
The statistical data of nine groups on tensile-bond strength are shown in Table 1. Bond strengths fluctuated when the specimens were irradiated by pulse Nd:YAG laser with different parameter combinations. When the frequency (Hz) was unchanged, the bond strength was reduced, with the power (W) increasing. When the power was constant, the bond strength increased, and then was reduced with the frequency increasing. Therefore, the low power (1 W) and the moderate frequency (15 Hz) contributed to dentine adhesion. Statistical analysis indicated that the mean tensile-bond strength of group 2 (1 W/15 Hz) was highest (8.87 ± 2.80 Mpa) and significantly different from those of the other eight groups (p < 0.01). Group 7 showed the lowest tensile-bond strength (2.28 ± 1.63 MPa) and a significant difference from group 1, 3, 5, and 6. Other groups showed no significant differences in tensile-bond strength (p > 0.05).
The mean tensile-bond strengths and the analyses of six experimental groups are shown in Table 2. The laser-parameter combination used in lased groups was 1 W/15 Hz, according to these tests. High tensile-bond strengths were found in laser-irradiated, laser + 10-3 solution, and 10-3 solution groups, and both were significantly different from those of other three groups (p < 0.05). In addition, the mean tensile-bond strengths of the acid-etched and laser + acid groups were significantly higher than that of negative control group (p < 0.05). No significant difference was found between any other two groups (p > 0.05).
The frequencies of the six experimental groups in each ARI score are shown in Table 3. High ARI scores were found in the laser + 10-3 solution (27) and laser-irradiated groups (25). The ARI score in the negative control group was lowest at only 2. The statistical analysis showed that the ARI scores of laser-irradiated group and laser + 10-3 solution group were significantly higher than those of acid-etched group, laser + acid group, and negative control group (p < 0.05), which indicated that more resin was left on dentine surfaces in the first two groups. In the four groups left, the negative control group was significantly different from all other groups (p < 0.05). As expected, SEM results showed that adhesive fractures occurred in the resin for most specimens of the laser-irradiated group and the laser + 10-3 solution group (Fig. 1A and E). However, most failures occurred at the interface of resin to dentine in the acid-etched group, laser + acid group, and negative control group (Fig. 1B, C, and F). For the 10-3 solution group, failures occurred partly in the resin and partly at the interface of resin to dentine (Fig. 1D).
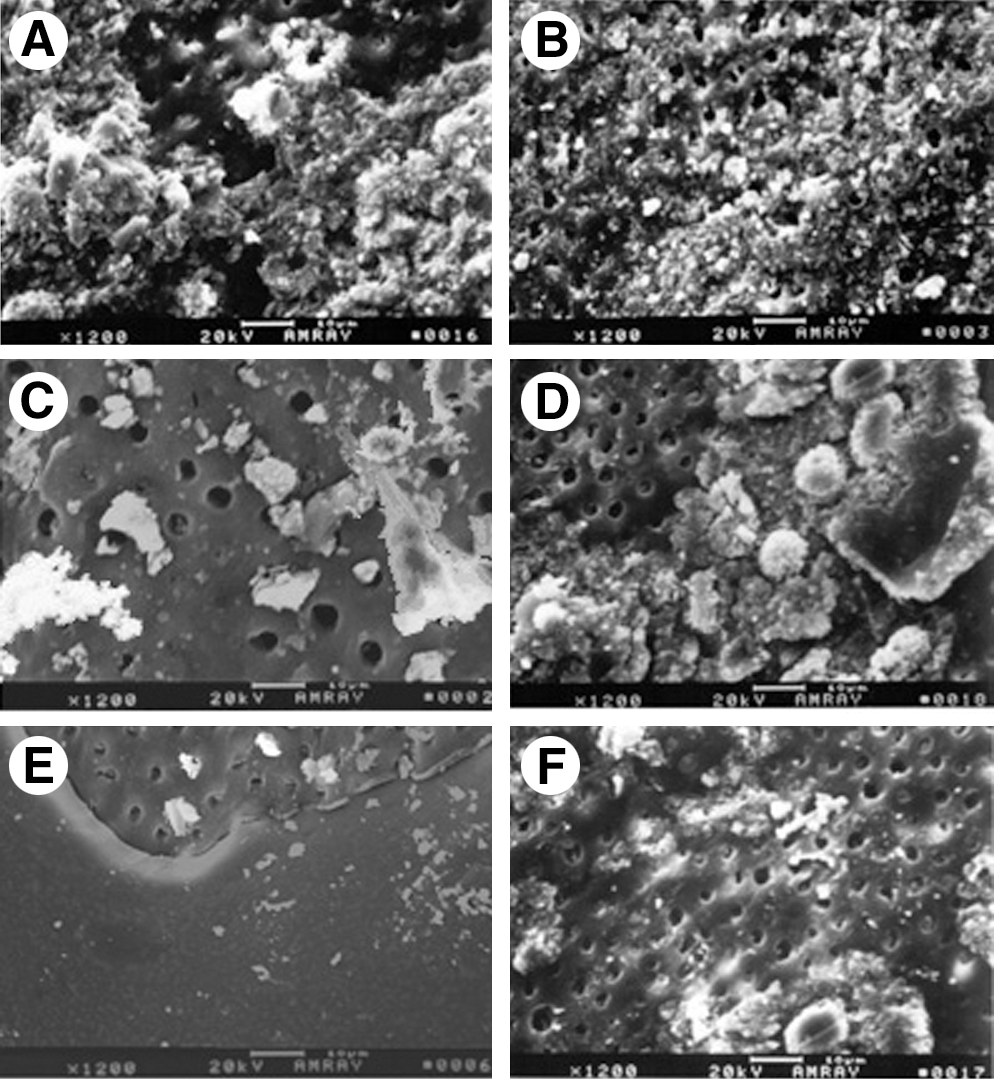
SEM results of characteristic debonded dentine surfaces. (
The frequencies in each microleakage score also are shown in Table 3. The low microleakage scores were found in the laser + 10-3 solution group (11) and in the laser-irradiated group (14), which indicated that the irradiation of pulse Nd:YAG laser and its association with 10-3 solution contributed to the adaptation of resin to dentine (Fig. 2A, E). The single 10-3 solution group still showed low microleakage (Fig. 2D), and the microleakage score was 22. However, the methylene blue solution reached the dental pulp in most specimens of the acid-etched group, laser + acid group, and the negative control group, whose microleakage scores were 35, 34, and 37, respectively (Fig. 2B, C, F). The statistical analysis indicated that the microleakage scores of the laser-irradiated group, laser + 10-3 solution group, and the 10-3 solution group were significantly lower than those of other three groups (p < 0.05). No significant difference was noted between any other two groups (p > 0.05).
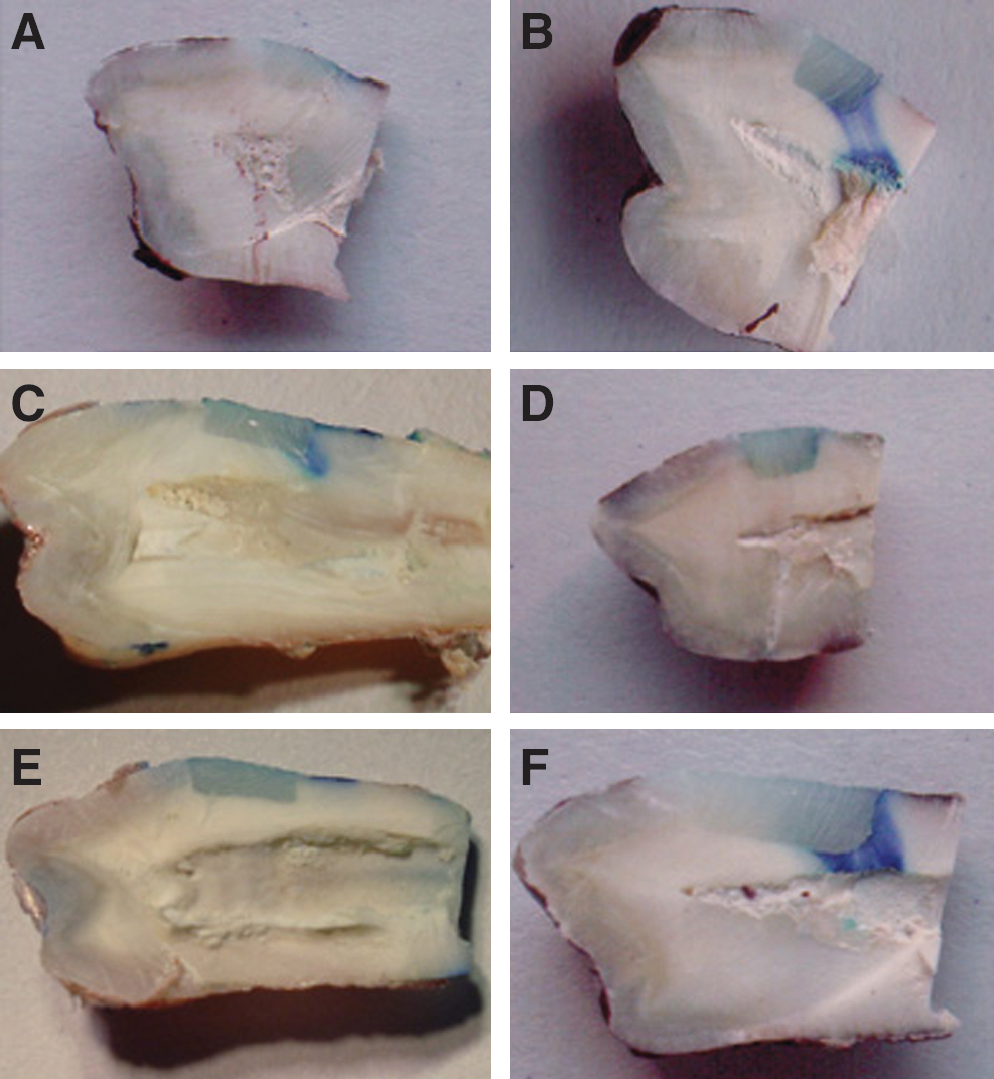
Typical samples of the resin/dentine interfaces of four groups tested on microleakage. (
Discussion
Dentine has a collagen-rich organic matrix between mineralized crystals, which is different from enamel, lacking significant amounts of organic components. Therefore, unlike enamel, adhesion to dentine has seen little improvement in the past decades. Evidence indicates that the Nd:YAG laser can cause dentine surface melting, followed by recrystallizing, and a rough area was observed, with many small scattered craters. 16 –18 The roughness may offer more microspaces for resin monomers to penetrate and form resin tags, which enhances the micromechanical retention and bond strength. That is why pulse Nd:YAG laser was selected as a preparation method for dentine adhesion in this study.
It is generally recognized that laser–tissue interactions include photochemical, photothermal, photodisruption, and photoablation processes. Two variables, output energy and frequency, affect the interactions of pulse Nd:YAG laser with dentine surfaces. Too-low output energy will not significantly change the dentine surface and too-high output will decrease the microhardness of the dentine surface, which is harmful to dentine adhesion. 19 Frequency, which determines the energy per pulse, affects the depth of the lased dentine surface and the thickness of the hybrid layer formed. It is necessary to filter the suitable energy and frequency to determine the effect of pulse Nd:YAG laser on dentine adhesion. To determine the effect of different laser parameters on tensile-bond strength of dentine adhesion and to optimize the laser-parameter combination for the subsequent comparison experiments, a series of experiments was performed. The results indicate that the groups irradiated with different laser-parameter combinations showed different tensile-bond strengths. The mean tensile-bond strength of the group irradiated with the parameter combination of 1 W/15 Hz was highest (8.87 ± 2.80 MPa) and significantly higher than those of the other groups. Therefore, 1 W/15 Hz is thought of as the optimal laser-parameter combination for dentine adhesion and was used in the subsequent comparing experiments.
It is well known that 35% phosphoric acid and 10-3 solution are commonly used in a pretreatment procedure in enamel/dentine adhesion. In our study, the effects of pulse Nd:YAG laser, 35% phosphoric acid, 10-3 solution, and their co-effects on dentine adhesion were examined. The results indicated that the groups of laser-irradiated, 10-3 solution, and laser + 10-3 solution showed good tensile-bond strength, whereas the other three groups of unconditioned, acid-etched, and laser + acid showed low tensile-bond strength. The 35% phosphoric acid has been well accepted as a pretreatment solution for enamel adhesion. However, it could not greatly improve the bond strength of resin to dentine in our study, and the mean bonding strength of 3.03 ± 1.73 MPa was higher than that of only unconditioned group. The same result was reported in a previous study. 20 Unlike enamel, dentine is built up by more-organic materials and water. Therefore, a deeper and richer collagen network is formed when dentine surface is etched by 35% phosphoric acid. It has been recognized that the infiltration of resin monomers is incomplete in the presence of a collagen network, and this will affect the bond strength. In addition, dentine has many dentinal tubules. As it removed the smear layer on the drilled dentine surface, acid-etching simultaneously enlarged the orifices of dentinal tubules, which reduced the mechanical interlocking between the composite material and the dentine and could not enhance the bond strength. In this study, even the laser-irradiated dentine surface was significantly changed by 35% phosphoric acid in the laser + acid group, which resulted in lower mean tensile-bond strength compared with that in the single laser-irradiated group.
The 10-3 solution, which contained 10% citric acid and 3% ferric chloride, has a softer etched effect than the 35% phosphoric acid. Previous studies reported that a 10-3 solution prevented the demineralized dentinal matrixes collapse and caused dentinal matrixes to be stiff, which contributed to dentin adhesion. 21, 22 In this study, the fairly good tensile-bond strength was obtained in the 10-3 solution group and was significantly higher than those of unconditioned, acid-etched, and laser + acid groups. But the mean tensile-bond strength of the 10-3 solution group was greatly lower than that of the laser-irradiated group, although no significant difference was noted. This indicated that pulse Nd:YAG laser showed a better effect for dentine adhesion. A similar result was obtained by Paranhos MP et al., 23 that Nd:YAG laser irradiation followed by a self-etching adhesive system contributed to the bond strength of resin to dentine. Dayem et al. 24 also reported in their study that Nd:YAG laser could remove the collagen network from acid-etched dentine and increased the penetration depth of the adhesive-bonding system.
The mechanism of pulse Nd:YAG laser increasing the tensile-bond strength of resin to dentine has not been completely clarified. Many studies have been done about this aspect in recent years, and evidence indicates that the irradiation of pulse Nd:YAG laser could partly remove the smear layer and cause the dentine surface tissue to melt and recrystallize. 12 This photothermal effect of pulse Nd:YAG laser made the dentine surface rough and the orifices of dentinal tubules sealed or partly sealed. It also integrated the rest of the smear layer with the sound dentine tissue, which eliminated the weakness in the hybrid layer between resin and dentine and increased the bond strength. 25 These effects of pulse Nd:YAG laser on the dentine surface may also contribute to the bond strength of resin to human dentine.
In this study, we also found that the irradiation of pulse Nd:YAG laser followed by 10-3 solution contributed to dentine adhesion. The mean tensile-bond strength of the laser + 10-3 solution was highest in all experiment groups, by an increase of 2.15 MPa compared with the single 10-3 solution group. No significant difference was found between these two groups. It was possibly because the specimen number of the experimental groups was not large enough in this study. Further studies are required to clarify the co-effects and the mechanism of pulse Nd:YAG laser and 10-3 solution on the bond strength of resin to human dentine.
The SEM observations coincided with the results obtained in tensile bond–strength tests. In most specimens of the laser-irradiated group, the laser + 10-3 solution group, and the 10-3 solution group, whose means of tensile-bond strength were higher, adhesive fractures occurred in the resin, and a large amount of resin was left covering the dentine surface. However, most fractures occurred at the interface of resin to dentine in the negative control group, acid-etched group, and laser + acid group, which indicated that a weak layer existed between resin and dentine. The SEM observations further revealed that the irradiation of pulse Nd:YAG laser, treatment with 10-3 solution, and their co-effect greatly contribute to the optimal bond strength of resin to dentine.
Although irradiation of pulse Nd:YAG laser and acid-etching by 35% phosphoric acid or 10-3 solution can both remove the smear layer and cause the dentine surface to be rough, the mechanisms are different. Acid etching causes the dentine surface to be demineralized, whereas pulse Nd:YAG laser makes the dentine surface melt and recrystallize, vaporize water and organic components, and produce many cracks and fissures. Whether pulse Nd:YAG laser contributes to the adaptation of resin to dentine is another question to answer. In this article, we also discuss the effect of pulse Nd:YAG laser on dentine permeability. The results indicate that the laser-irradiated group and the laser + 10-3 solution group had lower microleakage. In these two groups, no specimen was observed whose microleakage of methylene blue reached the cavity bottom under the stereomicroscope (10 × ). However, in the other groups (negative control, acid-etched, and laser + acid), in most specimens, the microleakage of methylene blue reached the dental pulp. Although acid etching or irradiation followed by acid etching showed higher bond strength and ARI scores compared with the negative control group, they produced no contributive effect in preventing the microleakage through the interface of resin to dentine. It was possibly because of the rich collagen network and the enlarged dentinal tubule orifices caused by 35% phosphoric acid.
Therefore, a conclusion can be drawn that the irradiation of pulse Nd:YAG laser with and without treatment with the 10-3 solution are both good methods to prepare for dentine adhesion because they not only increased the bond strength but also reduced microleakage, which could prevent secondary caries and protect the dental pulp from the outside deleterious stimulation. We must point out that all the results were obtained from experiments in vitro, and further studies in vivo are necessary before pulse Nd:YAG laser is used for dentine adhesion in clinical practice.
Conclusion
Based on our study, pulse Nd:YAG laser, 10-3 solution, and their cooperation showed favorable effects on bond strength and adaptation of resin to human dentine and can be used to pretreat dentine surface before adhesion. The optimal parameter combination of pulse Nd:YAG laser was determined to be 1 W/15 Hz in this study. The 35% phosphoric acid and its association with pulse Nd:YAG laser showed few contributive effects on human dentine adhesion and are not recommended for use as pretreatment methods in dentine adhesion.
Footnotes
Acknowledgments
We thank Prof. Dr. Huixia He for her kind reading and correcting of the manuscript and Prof. Zhiguan Zhang for his technical assistance. We also acknowledge financial support from the funding of Chongqing Science & Technology commission, China. (funding no. 20015421).
Author Disclosure Statement
No competing financial interests exist.