
Abstract
Introduction
High-power lasers have been used as tools on many surgical procedures and have been shown to be effective, safe, and advantageous when compared to other surgical techniques. 1,2 Some lasers may also kill bacteria. 5 On the other hand, many surgical wavelengths may cause thermal damage to the tissue and affect healing in many ways. 1,4
Several light sources operating at low energy levels at both the visible or infrared spectrum have been shown to be effective in treating inflammatory conditions, in the reduction of edema and pain, 11 and in improving wound healing and repair. 12 The use of this therapy does not cause cell damage since no thermal effect is caused by the light. 14 These days, both coherent and noncoherent light sources have been successfully used in the modulation of biological phenomena of several origins. 3
This study aimed to assess, histologically, the effects of the use of two types of phototherapies, laser (λ650 nm) or polarized light (λ400–2000 nm), on the healing of cutaneous surgical wounds created with a λ970-nm diode laser on the dorsum of rats.
Animal and Methods
This study was approved by the animal ethics committee of the Universidade do Vale do Paraíba - UNIVAP (no: a043/cep/2007). Thirty-one young adult (∼90 days old) male Wistar rats (∼350 g) were kept under natural conditions of light, humidity, and temperature at the animal house of the Instituto de Pesquisa e Desenvolvimento of UNIVAP during the experimental period. The animals were fed with standard laboratory pelted diet and had water ad libidum. The animals were kept in individual metallic cages on a day–night light cycle with controlled temperature during the experimental period. Under general anesthesia (1% atropine, 20 mL, Fagra®, 0.04 mL/100 g; 21 10 mL of 10% Cetamina® (Syntec, São Paulo, Brazil), 0.1 mL/100 g and 10 mL of 2% Cloridrato de Xilazina®, (Syntec, São Paulo, Brazil), 0.1 mL/100 g) 22 the dorsum was shaved and a 20- × 2-mm wound was created using a λ970-nm diode laser (4 W, φ ∼320-μm fiber (Sirona®, Bensheim, Germany). The animals were given antibiotics immediately after surgery (Pentabiótico®, Fort Dodge®, São Paulo, Brazil, 0.02 mL/100 g). The animals were then randomly distributed into 3 groups (G1, GII, GIII). Group I acted as untreated control. Each group was then subdivided into 3 subgroups according to animal death time: immediate (n = 5), day 7 (n = 3), and day 14 (n = 3). Subjects of GII and GIII were further treated with two types of phototherapies (laser or polarized light). Animals of GII were treated with laser light λ655 nm, 30 mW, φ ∼3 mm (Kondortech®, São Carlos, São Paulo, Brazil), 12 J/cm2]. Laser light was applied transcutaneously and fractioned on 6 contact points at the wound margins (6 × 2 J/cm2). The treatment was carried out at every other day during the experimental periods (7 or 14 days). Subjects of GIII were daily illuminated with a polarized light source (λ400–2000 nm, 40 mW, φ ∼5.5 cm (Bioptron®, Wollerau, Switzerland); focal distance of 10 cm; dose per session 12 J/cm2). Animal death occurred immediately and at 7 and 14 days after surgery and was carried out with an overdose of general anesthetics. A 16-cm2 specimen was removed and fixed in 10% formalin for 24 h. The specimens were routinely processed to wax, cut (5 or 3μm), and stained (HE, sirius red) or immunomarked (monoclonal antiactin, α-smooth muscle actin (Sigma-Aldrich®, St. Louis, MD, USA) at the Oral Pathology Laboratory of the School of Dentistry of the Federal University of Bahia. Each specimen underwent histological analysis carried out by an experienced pathologist in a double-blind manner. Three slides were made of each specimen. The criteria used for this analysis were adapted from one used previously by our team (Table 1). 23 When applied, each criterion was scored as absent, discrete, moderate, or intense according to the percentage of the phenomena observed. The percentage of occurrence of each score was analyzed using Minitab 15® software. Statistical analysis was carried out using the Fischer exact test or Kruskall–Wallis test, both at a significance level of 5%.
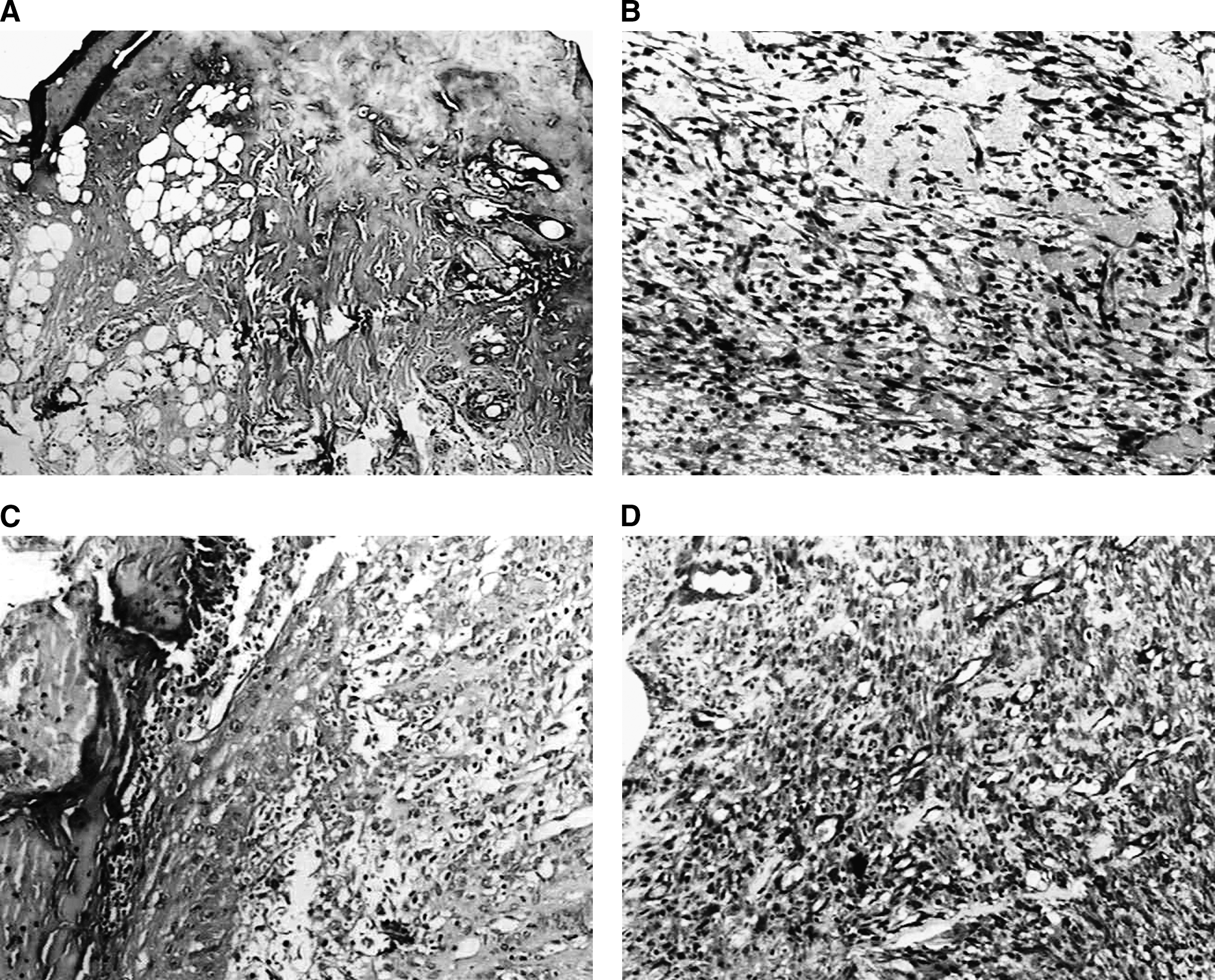
Immediately after surgery, control (GI) specimens showed tissue necrosis extending down to the hypodermis (Fig. 1A); there were some piknotic nuclei and collagen fibers far from the wounded site. Seven days after surgery the wound was covered by a thick crust and no re-epithelialization could be seen. Inflammatory reaction (acute, chronic, and mixed) was discrete. The presence of granulation tissue was intense at this stage, and this was rich in blood vessels. Large numbers of fibroblasts and intense deposition of collagen matrix were also observed. The number of myofibroblasts was discrete in 100% of the cases (Fig. 1B). At day 14, the wound was still covered by a thick crust and re-epithelialization was not seen in 33.3% of the cases. For 66.67% of these cases, the epithelium covered less than 50% of the wound (Fig. 1C). Inflammatory reaction was discrete and of varied type; the amount of granulation tissue was moderate and moderately vascularized. A marked number of fibroblasts and intense deposition of collagen matrix could also be observed at this time. Myofibroblasts were markedly seen on most specimens (66.67%) (Fig. 1D).
(
On laser-irradiated subjects (GII), at day 7, ulceration was observed and was covered by a crust of variable thickness with the presence of necrotic remnants. Epithelium was absent in all cases. Inflammatory reaction varied from discrete to moderate and was acute, chronic, or mixed. An intense deposition of collagen was observed on the wounded site, and angiogenesis varied from moderate to intense. There was a large number of fibroblasts placed parallel to the wound surface. Collagen deposition was moderate at this stage. The number of myofibroblasts was discrete on all subjects (Fig. 2A). At day 14, the presence of a crust of varied thickness was noticed, and the inflammatory reaction was discrete, chronic, and of mixed cellularity. Epithelium was not seen on 20% of the specimens. In 40% of the cases in which epithelium was present, it covered less than 50% of the wounded site. For 20% of the cases, epithelial recovery covered more than 50% of the wound, and for 20% of the cases 100% of the wound was covered by epithelial tissue (Fig. 2B). Deposition of granulation tissue was either discrete or intense and showed moderate angiogenesis. A large number of fibroblasts and moderate deposition of collagen matrix were also seen at this stage. A moderate amount of myofibroblasts was seen on 80% of the cases (Fig. 2C).

(
On subjects illuminated with polarized light, at day 7 after surgery, the presence of a thick crust and necrotic debris was seen on 60% of the cases; on the other 40%, no necrosis tissue was seen. Re-epithelialization was not seen on 80% of the wounds and covered less than 50% of the wound on 20% of the subjects. A discrete chronic inflammatory reaction was seen and was either chronic or of mixed cellularity. There was intense deposition of granulation tissue associated with intense angiogenesis. There was a large number of fibroblasts and moderate deposition of granulation tissue (Fig. 3A). A moderate amount of myofibroblasts was seen on 80% of the cases (Fig. 3B). Tissue edema was seen in some specimens. At day 14, 60% of the wounds showed crusting. Re-epithelialization was seen on 100% of the wounds on 60% of the subjects. For 20% of the cases, the epithelium was observed covering less than or more than 50% of the wounded site (Fig. 3C). The amounts of granulation tissue and angiogenesis were moderate. Inflammation was discrete and chronic on 60% of the cases. The number of fibroblasts was large, and intense deposition of collagen matrix was seen at this stage (Fig. 3D); both were parallel distributed to the wound surface. The number of myofibroblasts was larger in 80% of the subjects (Fig. 3E). A summary of the results is given in Table 2.

(

In the order seen in Table 1.
Statistical analysis showed significant differences in the number of myofibroblasts at day 7 between the two phototherapies; larger numbers were seen when the polarized light source was used (GIII, p = 0.04). At day 14, significant differences were seen between subjects illuminated (GIII) and irradiated (GII) (p = 0.05). Time was also important. Significant differences (p = 0.01) were seen between 0 and 7 days on irradiated (GII) and illuminated subjects (GIII) for re-epithelialization. There were also significant differences in the number of fibroblasts on illuminated subjects (GIII, p = 0.04). At day 14, significant differences were seen in the number of myofibroblasts on all groups
Discussion
Optimization of wound-healing processes with light sources is widely described in the literature. 8,10 This optimization is due to the effect of several wavelengths on the cells, and this is particularly seen on cells under some type of stress. However, the effects of light on thermally damaged tissues are not well reported in the literature.
Surgical laser wounds involve a different healing process, especially for wounds produced by wavelengths that cause heating of the tissues. This heating results in cell damage of different intensities depending on the distance from the impact site. These changes are mainly seen within the first week of the repair. The lack of cell viability on the thermally damaged area is considered the main factor in delaying re-epithelialization. 6 The literature also reports the presence of fewer myofibroblasts on this lesion. This aspect is the cause of minimal wound contraction and scarring. 31
In the present study, we found that wounds treated with laser phototherapy (GII) showed better response at day 14 when re-epithelialization was in a more advanced stage. It was also found that the number of myofibroblasts on these subjects was significantly different over the healing time (7 to 14 days). However, this number was smaller than that observed on controls, as previously reported. It has been reported that the use of high doses does not improve the proliferation of these cells. It is possible that such higher doses may further stress the cells and reduce migration and proliferation, viability, and mitochondrial activity. Our results suggest that smaller doses (4 to 8 J/cm2) may be more effective in inducing an increase of myofibroblastic proliferation.
The positive effect on myofibroblastic proliferation was also found on illuminated subjects at early stages of the healing process. At day 7, the number of myofibroblasts was significantly higher than on laser-treated subjects. 19 An overall tendency for a more advanced process was also detectable in this group. 3 The tendency for an increase in the number of myofibroblasts was also seen at the end of the experimental period, as well as a more pronounced deposition of collagen matrix. Inflammation was discrete and more advanced on illuminated subjects. 3 The overall observations of the present study are suggestive of more advanced repair on illuminated subjects when compared wih control and laser-treated subjects.
There is an overall tendency to use polychromatic light sources for the treatment of wounds. This use increases as positives results are reported elsewhere. It is important to note that the benefits reported in the literature are very similar to those reported when monochromatic light sources are used. 3 There are also reports that the use of polychromatic noncoherent light possesses beneficial effects for wound healing, mainly for fibroblasts and myofibroblasts, as found in the present study. 19 It is very important that specific protocols be observed owing to the differences in many parameters observed in the polarized light sources currently marketed. 3
When using thermal lasers such as those in the present study, the observed delay in healing, owing to cellular damage, is caused by heat. 2 However, this negative effect may be minimized by the use of certain wavelengths, including polarized light. In the present study, we found a significant increase in the number of myofibroblasts at early stages, more advanced re-epithelialization during the experimental time, and increased collagen deposition on illuminated subjects.
The results of the present study have shown that the effect of using laser light was more evident at early stages of the healing and that using polarized light improved the resolution of the inflammatory reaction, increased the deposition of collagen, increased the number of myofibroblasts, and quickened re-epithelialization during the experimental time.
Footnotes
Author Disclosure Statement
No competing financial interests exist.