
Abstract
Introduction
Since laboratory composites are highly polymerized, the repair of these materials is challenging due to the reduced availability of unreacted methacrylate groups. 4 Numerous studies have investigated the effect of different mechanical and chemical surface treatments on composite repair bond strength. 2,5,6 Mostly it has been reported that a proper bonding between laboratory composite and the newly added direct composite can be achieved by the combination of mechanical surface treatment of preexisting composite and the use of intermediate bonding agents and silanes, which can enhance repair bond strength. 4,7
Recently, the use of pulsed erbium lasers such as Er: YAG laser and Er, Cr: YSGG laser has been considered for surface treatment of tooth structure and it has been reported that Er, Cr: YSGG laser is capable of producing surface roughness comparable to that produced by acid etching of enamel and dentin surfaces. 8,9 Studies have evaluated the effect of Er: YAG laser on ablation of composite resins, 10,11 and have reported that in the composite resin ablation, explosive vaporization is followed by hydrodynamic ejection. During this process, rapid melting produces powerful expansion forces as a result of changes in volume of the material upon melting. Moreover, surface protrusions are formed, which result from counteracting forces interacting with the composite resin structure, and these protrusions are ejected away from the surface as droplets. 11 It has been suggested that this type of effect takes place in the composite resin ablation subsequent to Er: Cr: YSGG laser irradiation by a similar mechanism to that seen in hard tissue ablation by Er: Cr: YSGG and Er: YAG lasers. 12
Since there is not sufficient information regarding the effect of Er, Cr: YSGG laser on laboratory composite repair, the present study compared the effect of three mechanical surface treatment modalities, including use of a diamond bur, air-abrasion, and Er, Cr: YSGG laser, on the repair bond strength of a laboratory composite resin.
Materials and Methods
Sample preparation
Sixty cylinder-shaped specimens, 4 mm in height and 6 mm in diameter, were produced by layering 2-mm-thick increments of a laboratory composite resin (Gradia, shade DA2, GC Dental Products Corp., Tokyo, Japan) in a plastic mold. Each increment was cured for 10 sec with a light-curing device (GC STEPLIGHT SL-I, GC, Tokyo, Japan) according to the instructions provided by the manufacturer. The last increment was covered with an Acetate strip (Hawe Neos Dental, Bioggio, Switzerland) and compressed with a glass slide in order to obtain a flat surface for the specimen after light-curing. Subsequent to curing of the second layer, the specimens were removed from the mold and were placed in the GC LABOLIGHT LV-III Curing Unit (GC, Tokyo, Japan) for 3 minutes for post-curing of the laboratory composite according to the manufacturer's instructions. Then the composite cylinders were embedded in acrylic blocks with a 2-mm slice of the specimens extruding from the acrylic blocks. The specimens were stored in distilled water at 37°C for 3 weeks; then they were randomly assigned to four groups of 15 specimens each.
In group 1 (control), the specimens did not receive any mechanical surface treatment.
In group 2, the surface of the laboratory composite was roughened for 3 sec with a coarse diamond bur (012 Cylinder Flat End, SS White Burs, Inc. Lakewood, NJ) placed tangential to the surface and rotating at a high speed with constant water spray. A new bur was used after five bur treatments. Then, the specimens were rinsed with distilled water and air-dried. The surface of the bur-ground sample under stereomicroscope (Nikon, Tokyo, Japan) at magnification × 40 is shown in Fig. 1 (a).
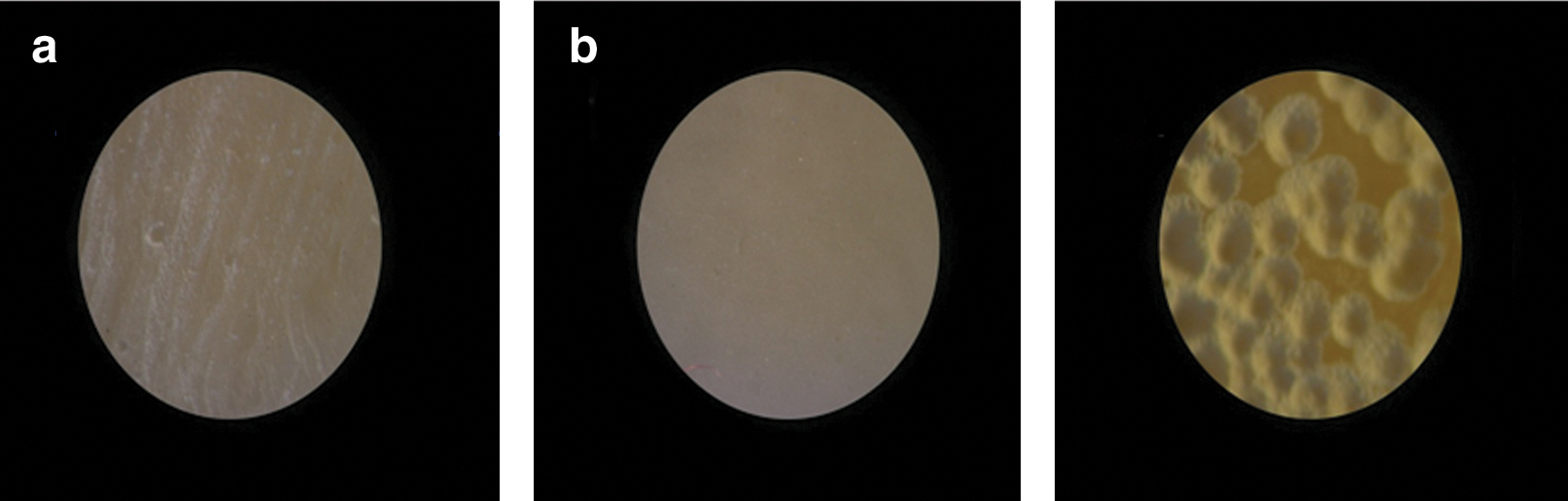
Images of the surfaces of bur-ground
In group 3, the specimen surfaces were air-abraded at a pressure of 60 PSI using an air-abrasion device (Microblaster Dento-Prep TM, Dental Microblaster, Denmark) for 10 sec with 50-μm aluminum oxide particles, with the tip positioned 5 mm away from the target and perpendicular to the specimen surface. Subsequently, the specimens were rinsed with distilled water and air-dried. The surface of the air-abraded sample under stereomicroscope is represented in Fig. 1 (b).
In group 4, an Er, Cr: YSGG laser unit (Biolase Europe GmbH, Paintweg 10, 92685 Floss, Germany) with a 600-μm-diameter G-type laser tip was used for surface treatment. This laser system emits photons at a wavelength of 2.78 μm that were pulsed with durations of 140-200 μs and a repetition rate of 20 Hz. The output power of this device can be varied from 0 to 6 W. Laser power of 2 W (100 mJ) at 15% air level and 10% water level, as determined to be optimal in a pilot study, was used. The beam was aligned to be perpendicular to the target area, and was applied at a 1 mm distance during an exposure time of 5 sec; subsequently, the specimens were rinsed and air-dried. The surface of the laser-treated sample under stereomicroscope is shown in Figure 1 (c).
In all of the groups, composite primer (GC Dental Products Corp., Tokyo, Japan) was used as a silane according to the manufacturer's instructions and was light-cured for 20 sec using a conventional quartz halogen light-curing unit (Astralis 7, Ivoclar Vivadent, FL-9494 Schaan, Liechtenstein) at a light intensity of 400 mW/cm2. Then, single-bottle adhesive resin (Adper TM Single Bond, 3M ESPE, Dental Products, St. Paul, MN, USA) was applied and cured according to the instructions provided by the manufacturer. Plastic molds 2 mm in length and 4 mm in diameter were placed over the test surfaces at the center of the samples. Then, a direct composite resin (Gradia DIRECT, shade A2, GC Dental Products Corp., Tokyo, Japan) was applied as a repair material with a thickness of 2 mm, and light-cured using an Astralis 7 curing unit for 40 sec at a light intensity of 400 mW/cm2. Following mold removal, the newly added direct composite was cured for 20 sec from each side, which added up to 80 sec. The specimens were individually stored in distilled water at 37°C for 24 h.
Shear bond strength test
The specimens were then subjected to a shear bond strength test 13 using a universal testing machine (Hounsfield Test Equipment, Model H5K-S, Tinius Olsen Ltd., Surrey, England). A crosshead speed of 1 mm/min was used to fracture the repaired surface interface. Shear bond strengths were recorded in Newtons and converted to megapascals (MPa). In order to determine failure modes, a stereomicroscope (Olympus SZX9; Olympus, Tokyo, Japan) was used at magnification × 30. Failure mode was classified as follows: 14
Adhesive (fracture at the interface between the laboratory composite and the direct composite)
Cohesive (fracture within the laboratory composite or the direct composite)
Mixed (adhesive-cohesive fracture)
Surface topography characterization
The surface topography of the laboratory composite in the control group and groups 2–4 following the different mechanical surface treatments and prior to adding a direct composite was characterized by atomic force microscope [AFM] (NanoScope® II, Digital Instruments, USA). Two extra specimens in each group were prepared for AFM characterization. AFM was used in contact mode using a silica nitride tip (with a nominal radius of 50 nm, apex angle of 45°, height of 2.8 μm, and 4 × 4 μm base) which was connected to a fixed substrate on a cantilever. The images were recorded with a scan rate of 1.9 Hz and a resolution of 512 × 512 or 256 × 256 pixels per image. For each specimen, two scans were performed at each specimen surface quadrant at a scanning area of 5 μm × 5 μm or 10 μm × 10 μm. The collected 3D topographical data were analyzed using data analysis software (NanoScope® III, Version 5.12r2, Digital Instruments, CA). For each group, the surface roughness was calculated by the root mean square (rms) of the values of the surface departures within the sampling area and is expressed in nm; furthermore, the surface area difference was calculated in percent [%] (the difference between the surface area following treatment and the surface area in its smoothest condition).
Statistical analysis
All data for bond strength, surface roughness, and surface area difference were analyzed using one-way ANOVA. Pairwise comparisons were made by Tukey test. Statistical significance was set at p < 0.05.
Results
Repair bond strength
Repair bond strengths in MPa (means and standard deviations) for the groups are shown in Table 1.
Values followed by the same letter were not significantly different by Tukey test. p < 0.05 was considered statistically significant.
There were statistically significant differences in bond strengths among the groups (F3,56 = 741.161, p < 0.0005). Two-by-two comparisons by Tukey test (Table 1) showed that there were significant differences in bond strengths between group 1 and the other groups (p < 0.0005). Furthermore, the differences in bond strengths between group 2 and groups 3 and 4 were statistically significant (p < 0.0005) whereas the bond strength differences between groups 3 and 4 were not statistically significant (p = 0.42).
Failure mode
Failure modes of the groups are shown in Fig. 2. Cohesive failures were observed only in groups 3 and 4. Adhesive failure was predominantly observed in groups 1 and 2 while in groups 3 and 4 failures were primarily mixed followed by adhesive failures.
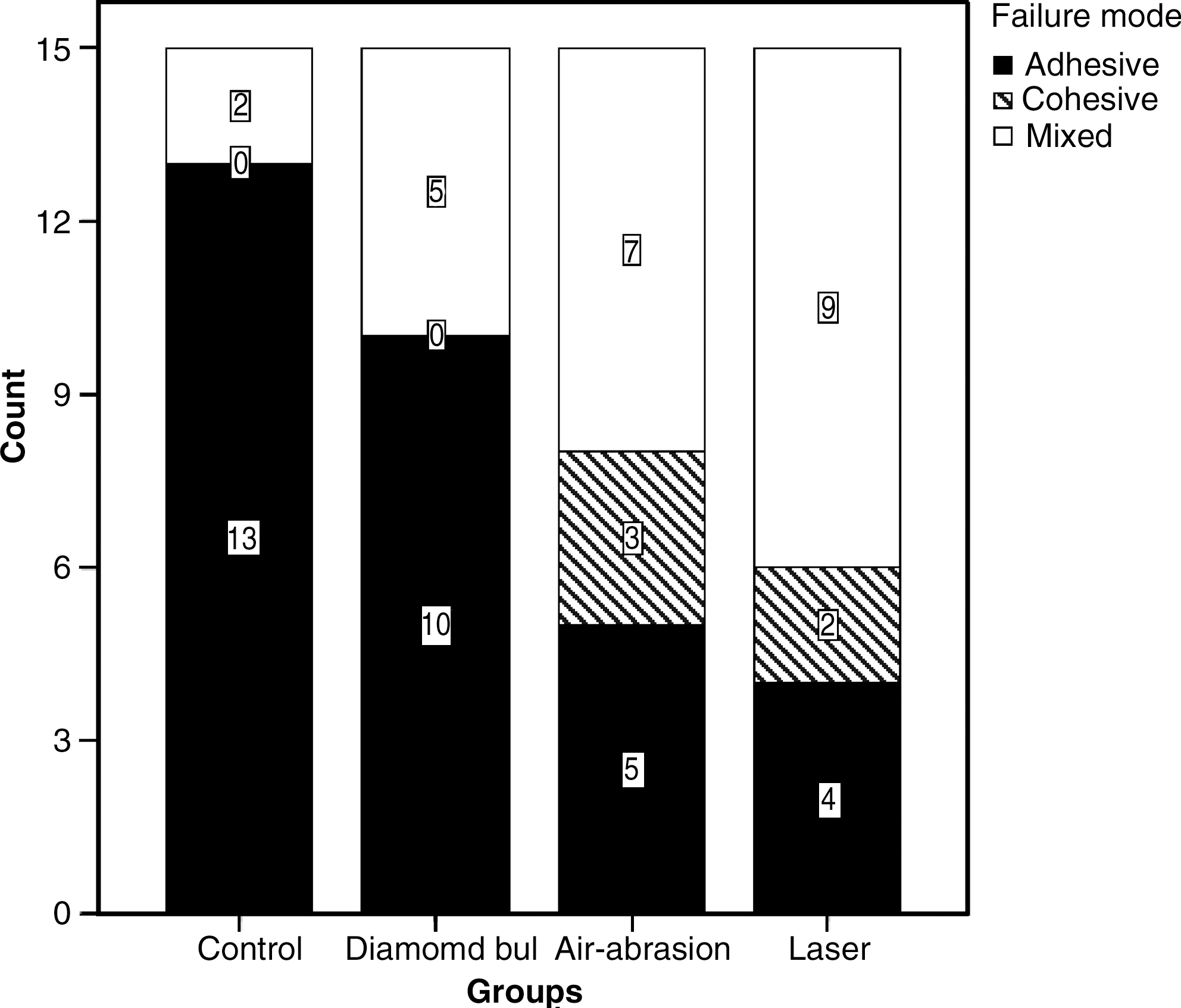
Failure modes of study groups.
Surface topography characterization
Selected AFM images of the surfaces of the non-treated, bur-ground, air-abraded and laser-treated laboratory composite specimens are presented in Fig. 3 (A-D). Group 1 represents a relatively smooth natural surface in the AFM image (Fig. 3A). A distinct ground grooved pattern is observed in the AFM image of group 2 (Fig. 3B). Macro-roughness and irregularities of smaller size are observed in the AFM image of group 3 (Fig. 3C). The AFM image of group 4 is characterized by a combination of macro and micro surface protrusions (Fig. 3D).
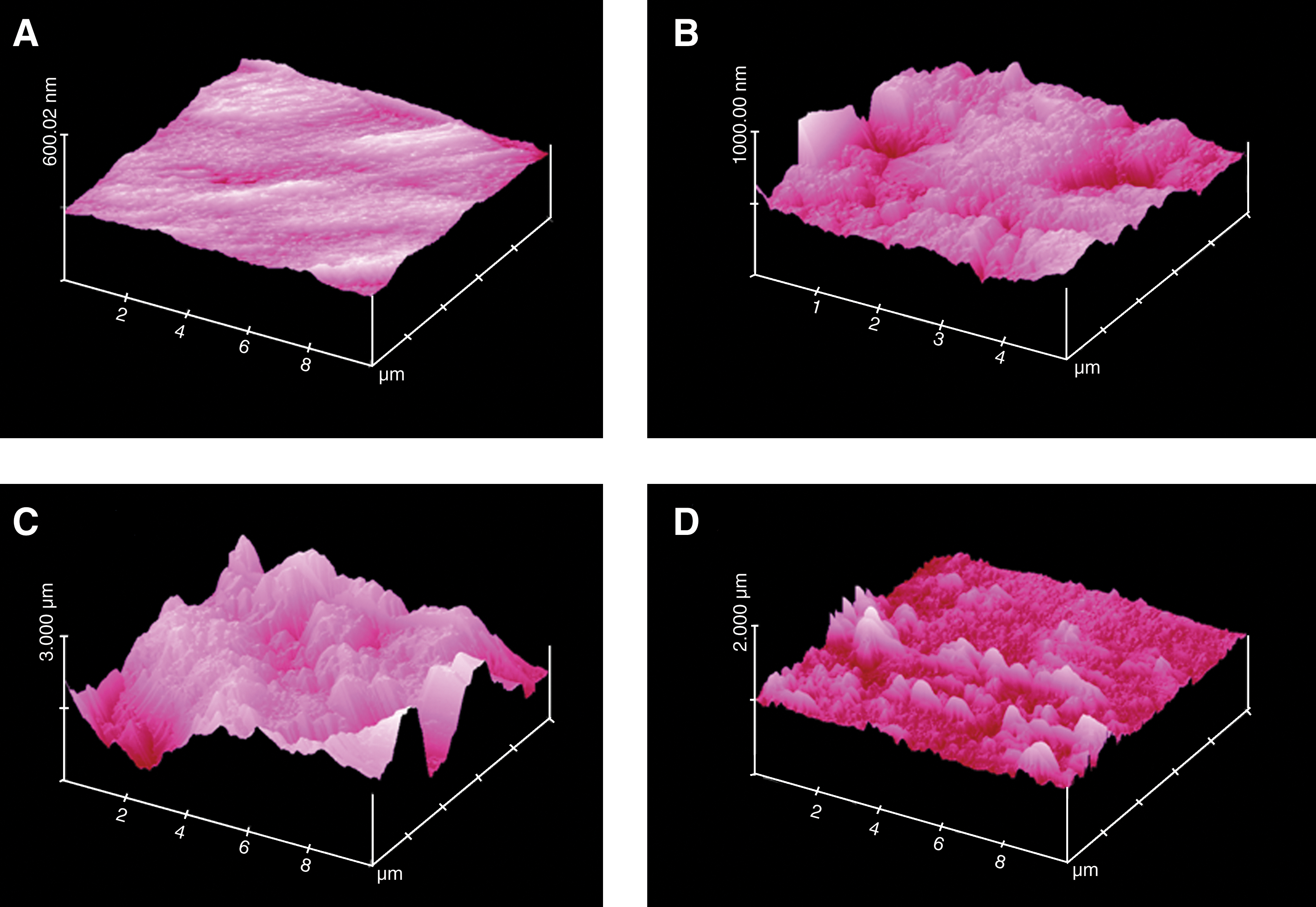
AFM 3D topographical images of the surfaces of the non-treated
The results of statistical analysis of the surface roughness (rms) and surface area difference (%) are presented in Table 2.
Mean values with dissimilar letters in the same column are statistically significant at p < 0.05.
There were statistically significant differences in surface roughness and surface area difference among the groups (p < 0.0005). The differences in surface roughness between groups 2 and 4 were not statistically significant (p = 0.12) whereas the differences between other groups were statistically significant (p < 0.0005). Regarding surface area difference, the differences between groups 3 and 4 were not statistically significant (p = 0.82) while there were significant differences between other groups (p < 0.0005).
Discussion
A successful repair procedure depends on high bond strength between the existing laboratory composite and the newly added direct composite. 14 In the current study, a bonding agent (Single Bond) and silane were used in all of the groups prior to adding the direct composite. This was done because the reportedly poor wettability properties of high-viscose newly added composite necessitate the application of a low-viscose bonding agent to penetrate the microcracks and irregularities in the matrix of the preexisting composite to obtain micromechanical retention. 15 Furthermore, the use of silane may improve bond strength by establishing covalent bonds between the monomers of the adhesive system and exposed fillers that have lost their layer of silane because of mechanical surface treatments. 7
The results of the present study demonstrated that the control group, with no mechanical surface treatment, had lower repaired bond strengths compared with the other groups with surface roughening. The results of the present study seem to be consistent with those of previous studies in which mechanical interlocking has been determined to be the most important factor in maximizing the repaired bond strength. 3,15,16 Moreover, mechanical roughening procedures increase exposure of fillers. 5 Therefore, combining silane treatment with mechanical roughening methods might produce better bond strength because of enhanced interaction between the exposed fillers and the adhesive system. In addition, the data obtained from AFM images revealed that the three mechanical surface treatments significantly increased the surface area in comparison with the control group, which can be considered an important factor in increased repair bond strength in groups 2 - 4.
According to the results of the preset study, surface treatment using air-abrasion and Er, Cr: YSGG laser results in higher repair bond strength values compared with surface treatment using diamond burs. It has been suggested that various mechanical surface roughening methods may lead to differences in smearing and matrix cracking and may affect bond strength. 15 It has also been reported that air-abrasion produces micro-retention features, while a diamond bur generates micro- and macro-retentive features. 14 In the presence of a bonding agent, higher bond strength is expected from air-abrasion, which yields micro-retention, because the adhesive resin infiltrates into the micro-irregularities of the laboratory composite surface, resulting in better surface wetting. 3, 7 The results of the present study coincide with those of Cavalcanti et al., who reported that surface treatment of direct composite with air-abrasion led to higher repair bond strength values compared with diamond burs. 14 In contrast, Bonstein et al. found that surface treatment with diamond burs resulted in higher bond strength compared with air-abrasion in the repair procedure of direct composites. 16 In addition, Bouschlicher et al. did not find significant differences between the efficacy of diamond burs and air-abrasion for direct composite repair when silane and bonding agent were used. 17 These differences might be attributed to the type of composite used, since composite composition and surface characteristics can affect the efficacy of mechanical surface treatment. 7 Moreover, various adhesive systems used in different studies might have led to discrepancies in the results since the penetration of the bonding agents into the surface irregularities is influenced by their viscosity and their surface tension. 18 In this study, AFM data of the air-abraded group showed a dramatic increase in surface roughness and surface area compared with the bur-ground group, which could have led to increased repair bond strength in the air-abraded group in comparison with the bur-ground group.
The higher repair bond strength in the laser-treated group compared with the bur-ground group might be attributed to the lack of a smear layer on the surface of the laboratory composite. In contrast to the bur, which wears out substrates such as restorative materials and produces a smear layer, laser ablates the restorative materials without smear layer formation, 10,12 and several studies have shown that Er, Cr: YSGG laser does not produce any smear layer. 8,12,19 Formation of a smear layer makes bonding of the adhesive resins difficult because of its low surface energy. 20
Regarding the AFM data, although there were no significant differences in surface roughness values between laser-treated and bur-ground groups, in the laser-treated group there was a significant increase in surface area compared with the bur-ground group. It is proposed that the increase in surface area as a consequence of surface treatment can be considered a better predicting factor for the formation of efficient repair bonding compared with surface roughness values.
The results of the present study did not demonstrate any significant differences in bond strengths between the laser-treated and air-abraded groups. In other words, Er, Cr: YSGG laser was as efficient as air-abrasion with aluminum oxide particles. According to the AFM data, air-abrasion results in increased surface roughness compared with laser treatment. One explanation might be the fact that laser treatment (with the parameters used in this study) resulted in hole formation on the surface of the laboratory composite, which was easily detectable under a stereomicroscope (Fig. 1 c), whereas the microstructures formed following air-abrasion were not detectable under a stereomicroscope (Fig. 1 b), and it seems that the laser-treated group is rougher than the air-abraded group macroscopically. However, by using AFM only, the topography of only a few limited regions such as inter-hole or intra-hole areas could be scanned. Therefore, the total roughness value could not be evaluated. Unlike the surface roughness, the surface area increased similarly in both groups and these results are in accordance with repair bond strength values. Because of some adverse effects on the human body of aluminum oxide aerosols used in the air-abrasion method, 21 Er, Cr: YSGG laser can be considered a safe alternative mechanical surface treatment modality for laboratory composite repair procedures.
Considering failure mode, previous studies have reported that if a composite repair tends to fracture cohesively, it can be assumed that the selected protocol is appropriate to bear the occlusal loads. 2,14 In the current study, cohesive failures were only observed in laser-treated and air-abraded groups. In the control and diamond bur groups adhesive failures were observed predominantly followed by mixed failures while in the laser and air-abrasion groups most failures were mixed followed by adhesive and cohesive failures.
It has been suggested that dental composite filler particles scatter the energy of laser while various components of the resin-based compartment absorb laser energy. 22 Since the components of the resin-based compartment in various laboratory composites may vary, affecting the ablation rate, 10 the effect of Er, Cr: YSGG laser treatment on different laboratory composites with various structures and chemical compositions should be evaluated in the repair procedure in future studies. Other studies using the microtensile bond strength test are warranted to further simulate clinical situations, since the bonded interface of small specimens in microtensile bond strength tests has a better stress distribution during loading, reducing the odds of crack initiation and propagation within individual specimens. 23 Furthermore, long-term studies are warranted to evaluate the bonding durability of Er, Cr: YSGG laser-prepared composites.
Conclusion
Within the limitations of this study, it was concluded that mechanical surface treatment using diamond bur, air-abrasion, or Er, Cr: YSGG laser results in higher repair bond strengths compared with non-mechanically treated controls. Moreover, treatment with laser shows almost no difference from air-abrasion, and both methods result in higher bond strengths compared with treatment with diamond bur.
Footnotes
Acknowledgments
The authors would like to thank the vice chancellor for research, Dr. Abdolhosein Kazemi, at Tabriz University of Medical Sciences for his financial support. Furthermore, the authors thank Dr. M. Abdolrahimi (D.D.S.), who edited the English manuscript of this article and Dr. M.R. Naimi-Jamal for his assistance in AFM imaging. This study was supported by a grant from Tabriz University of Medical Sciences.
Author Disclosure Statement
No competing financial interests exist.