
Abstract
The aim of this study was to evaluate the apical sealing of dentinal tubules after root-end surface cutting by using Er:YAG and Nd:YAG lasers. After root-canal instrumentation and filling, apices of 50 extracted maxillary canine human teeth were resected by Er:YAG with 400 mJ, 10 Hz, for 30 sec. The samples were randomly assigned to five groups (n = 10): (GI) treated without root-end cavity, but with Nd:YAG (1.0 W, 10 Hz, 20 sec) for dentinal tubules sealing; (GII) treated with root-end cavity without the use of Nd:YAG; (GIII) treated with root-end cavity and Nd:YAG application; (GIV) treated with root-end cavity made by Er:YAG with no focus and without Nd:YAG application; and (GV) treated without root-end cavity and without Nd:YAG application. The root-end cavities were performed by using Er:YAG at 300 mJ, 10 Hz, for 20 sec. Subsequently, all teeth were waterproofed and immersed in 2% methylene blue for 48 h in a vacuum environment. The samples were longitudinally sectioned, and microleakage was measured. ANOVA and the Fisher LSD test showed that GIV was less susceptible to microleakage than were the other groups (p < 0.05). Interestingly, the use of the Er:YAG with no focus showed superior dentinal tubule sealing in comparison with the other groups, even with or without root-end cavity and Nd:YAG application.
Introduction
The appropriate root-end sealing by retrograde filling has seemed to avoid the microorganisms and metabolic-products penetration through the apical, periapical, and root-canal systems. With the development of both new root-end preparation techniques and biomaterials, appropriate apical sealing could be promoted, increasing the success of periapical surgery. 1 Among the different surgical modalities, resection followed by root-end preparation, which comprises the root-apex removal and the execution of the apical root-end cavity for subsequent root-end filling, can be highlighted. For the accomplishment of such a procedure, rotary burs with profuse water cooling have been used. However, because of the rotary-instrument type and inclination used, irregularities on the root-canal walls, besides excessive exposure of the dentinal tubules, could be produced, which would contribute to treatment failure. 2,3
In endodontics, Nd:YAG laser has been used for bacterial reduction in infected root canals 4 and for reduction of dentinal permeability 5 and structure alteration. 6 –8 The Er:YAG laser has been used in periapical surgery for apical resection, 9 and it has been effective in the treatment of periapical lesions. 10 Because of its use without direct contact with the dental structure, this laser has not caused vibration, therefore presenting a low risk of both contamination and adjacent tissue trauma. 1
Therefore, the aim of this present study was to evaluate the apical sealing of the dentinal tubules when exposed to Er:YAG for apical resection and root-end cutting associated with Nd:YAG irradiation.
Materials and Methods
This study was conducted according to the Ethics Committee of the Positivo University (no. 150/09). Fifty extracted fully developed maxillary canine human teeth, stored at the Human Teeth Bank in a saline solution renewed once a week, with single and straight canals, were divided into five experimental groups with 10 teeth each. After preparing a conventional coronal access cavity for each tooth, a no. 10 K-file (Dentsply Maillefer , Ballaiques, Switzerland) was inserted into the canal until it was visible at the apical foramen, and then 1 mm was subtracted to determine the working length. The canals were prepared by using a crown-down technique with K-files to a master apical file size no. 50 (Dentsply Maillefer). The preparation of the middle and cervical thirds was made by using Gates-Glidden burs. The apical patency was maintained throughout preparation with the use of a no. 15 K-file, by using 2 ml of 2.5% sodium hypochlorite irrigation solution between filings. The final irrigations were made with 17% EDTA solution, followed by 2 ml of sodium hypochlorite solution (2.5%). All teeth were filled with gutta-percha and Endofill root-canal sealer (Dentsply Maillefer Industry and Trade Ltd., Petropolis, Brazil) by using the thermoplasticized technique with a gutta-condensor no. 60 (Dentsply Maillefer Industry and Trade). Finally, the crowns were restored by using composite resin (Filtek Z250; 3M-ESPE, St. Paul, MN). All teeth were stored in a kiln at 37°C and 100% humidity for 24 h.
Subsequently, all groups underwent root-end resection (3 mm) at a right angle to the long axis of the root, performed with an Er:YAG laser (Dental Twinlight; Fotona Medical Laser, Ljubljana, Slovenia) without contact with the structure, with a focal distance of 1.5 mm, pulse energy of 400 mJ, frequency of 10 Hz, and pulse duration of 30 sec.
In groups II, III, and IV, root-end preparations were made with three consecutive applications of the laser with a pulse energy of 300 mJ, frequency of 10 Hz, and pulse duration of 20 sec. In groups II and III, the focal distance was 1.5 mm, whereas in group IV, the irradiation distance was 2.5 mm, for the application without focus, under the same parameters of 300 mJ, frequency of 10 Hz, and pulse duration of 20 sec.
In groups I and III, the sealing of the dentinal tubules was performed with the laser Nd:YAG (Dental Twinlight; Fotona Medical Laser) after the noncontact mode at a potency of 1.0 W, frequency of 10 Hz, pulse duration of 20 sec, focal distance of 1.5 mm, and in parallel/single direction sweeping movement (Tables 1 and 2). Er:YAG laser was manually applied through a 1.5-cm-long fiber tip, with diameter of 940 μm, without contact mode, with distillated water-spray cooling (20 ml/min at 70 psi). Nd:YAG laser was applied without water-spray cooling, and the optic fiber was used in a direct-contact mode to the tooth. All root ends were prepared by one single operator. The root-end cavities were considered complete when all preparations, including the filled canals, presented 3-mm deep class I cavities and no visible gutta-percha remained on the cavity walls.
The teeth were waterproofed with two layers of epoxy resin (Araldite-Ciba-Geigy S.A., Taboao da Serra, Brazil) and two layers of nail polish, except for the apical surface that had been cut. The dental crowns received a final wax layer. All specimens were submerged in a 2% methylene blue solution, for 48 h, in vacuum atmosphere (160 mm Hg). Afterward, all teeth were rinsed for 48 h in running water, and the waterproof layers were removed with the aid of a scalpel. Vertical grooves were made in the buccal and palatal faces of all specimens, until the teeth were longitudinally split. A Perfilometer (Nikon, Tokyo, Japan) was used to assess the microleakage extension (apical-crown direction).
Data obtained among groups were statistically analyzed by using Statistica 6.1 program (StatSoft, Inc., Tulsa, OK, 1984–2003).
Results
Data obtained were submitted to a normality test (Lilliefors test), ANOVA test (in which F (4,35) = 6.4994; p = 0.00051), and to the Fisher LSD (Least Square Difference) post hoc test, in which p < 0.05. Therefore, statistical significance was analyzed, that is, the groups had different means and variances. Group IV (Er:YAG, no focus) showed the highest apical sealing, statistically superior to groups I, II, III, and V (p < 0.05). Figure 1 expresses the standard deviation (SD) values of microleakage extension, and Table 3 shows the relation between laser and microleakage extension.
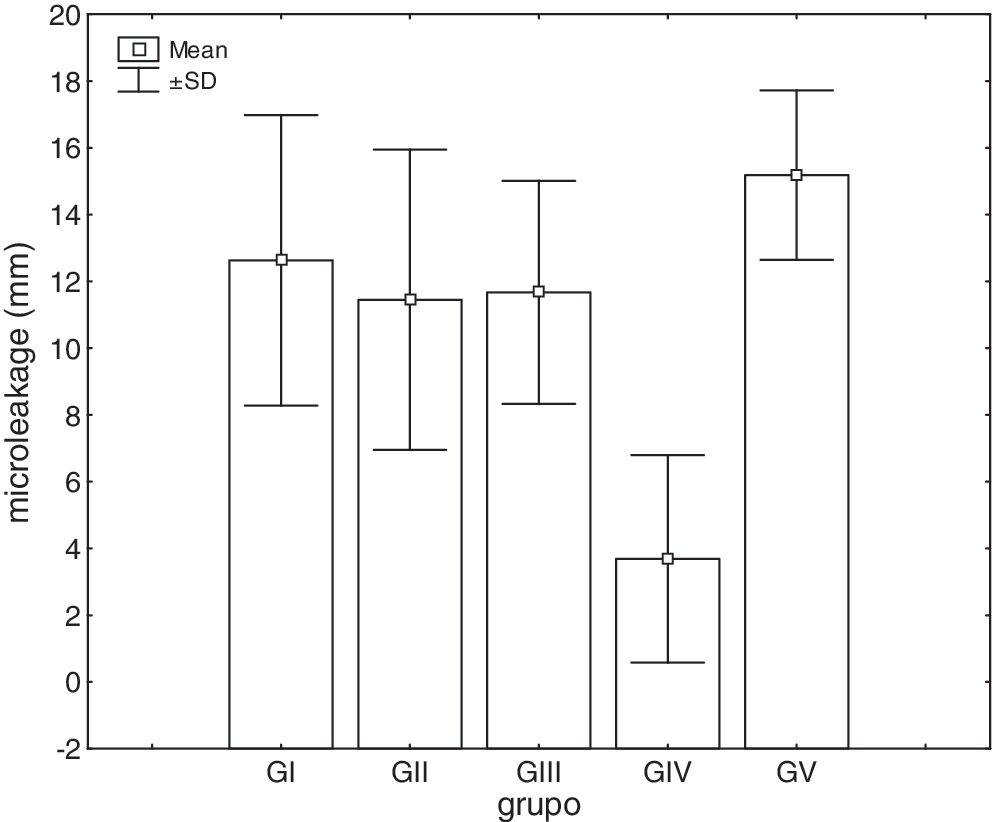
Standard deviation values of microleakage extension.
Discussion
In this study, we accomplished the resection with laser Er:YAG according to other studies. 11,12 Er:YAG offers advantages, such as the absence of discomfort and vibration, contributing to minimize the contamination of the surgical area and reducing the adjacent tissue trauma. 13,14 Its clinical application has been related to the execution of root resection, justifying its use in this study, in which the results obtained could be applied to clinical practice.
In dental-tissues preparations, the residual smear layer could be disadvantageous if it were not removed, because it would inhibit either the action of the irrigation solution, intracanal medication, or adequate contact of the sealer with dentinal tubules. The use of the laser was introduced in endodontics to produce disinfection and smear layer removal. 15,16 However, irradiation with either Er:YAG or Nd:YAG alone has not been able to remove the smear layer completely. 17 –19
Apical microleakage could be evaluated by different study methods, for example, by using dye solutions, tomographies, 20 transparent tooth technique, 21 or bacterial leakage. 22 Fluorescent dyes have been used as leakage tracers because they are easily detectable, easily registered in images, nontoxic and inexpensive, and require short immersion periods, besides providing reproducible results. 23 This study used the waterproof technique and a 2% methylene blue solution for dye penetration, because this is an old and widely known method. This dye solution has a superior penetration capacity in relation to other dyes. 24 Studies that evaluated the sealing ability in root-end cavities prepared by either laser, ultrasonic device, or burs showed better results with the use of the laser. 1,25 The irradiation with Er:YAG and CO2 for both the root-end resection 26 and dentinal surface treatment has been demonstrated to reduce the permeability to methylene blue solution. 27 In this study, CO2 laser was not used; however, group IV (Er:YAG, 2.5 mm, no focus) produced the greatest apical sealing, which was significantly better than the other groups, even in comparison with group II, in which the same parameters were used, except the lack of focal distance (1.5 mm). However, some studies showed that the sealing provided by laser use on surfaces that had undergone apicectomy, per se, would not result in an appropriate sealing. It would be necessary to fill the root-end cavity with either endodontic sealers or composite resins, for example. 28,29 Nevertheless, in our study, the cavities were not sealed by any material, because the aim of this study was to verify the apical sealing after laser use.
When ultrasound has been used, apical sealing has not been as satisfactory as the sealing provided by laser use for preparing the root-end cavity. Laser would favor the smear-layer removal, therefore allowing a better adaptation of the retrofilling material, by creating tags. 30 Laser application also would result in a more irregular dentinal surface, with retention areas that would allow a greater mechanical adhesion between the filling material and dentine. 31 Conversely, Nd:YAG has not promoted these irregularities on dentinal surface, but has resulted in dentinal tubules sealing. 32 It is worth noting that the sealing performed by the retrofilling material would be the result not only of the mechanical adhesion with the irregular dentine but also of the type and composition of the material used.
A poor root-end cavity sealing could lead to therapy failure. In an attempt to improve and even compensate for the possibility of sealing failure provided by the material, we sought to verify in this study the laser sealing ability, which was used both for root-end cutting and for cavity preparation (Er:YAG), besides the treatment of the apical surface that had undergone apicectomy (Nd:YAG). Er:YAG laser is capable of cutting hard tissue, with the advantage of not causing the excessive heating of the structure. Its clinical application in cavity preparation has produced favorable outcomes. 33
In our study, we used teeth with root canals prepared and subsequently filled with gutta-percha and endodontic sealer. Regarding microleakage, it is worth noting that laser application on gutta-percha could result in the formation of empty spaces between the canal obturation and dentinal walls, as was observed by the study of Paghdiwala, 30 who found such gaps. This presence of gaps in root-canal obturation could lead to doubts about the laser sealing ability. However, in this study, such gaps in root canal obturation were not observed after laser application.
Gouw-Soares et al. 27 observed smaller microleakages in samples apicoectomized with both CO2 and Er:YAG when compared with samples prepared with a high-speed bur. Conversely, Kimura et al. 34 observed that radicular canals prepared with Er:YAG laser did not showed less leakage than those conventionally prepared. It is worth highlighting that these authors made neither apicectomies nor root-end cavities, preparing all root-canal lengths.
Although the thermic effect on periapical tissues was not monitored in this study, it has been a concern after in vivo laser use. Kimura et al. 35 measured the radicular surface temperature during the root-canal preparation with Er:YAG and water-spray cooling. These authors observed an increase smaller than 6°C at the apical area, therefore suggesting that the thermic effect on the periodontal ligament would be minimal. In our present study, water-spray cooling was used for Er:YAG laser irradiation (20 ml/min at 70 psi) .
Further research on the effect of Er:YAG laser irradiation for both apicectomy and root-end cavity preparation, besides Nd:YAG laser irradiation for dentinal surface treatment, is necessary, previous to clinical application.
Conclusions
Based on the methods and parameters used in this study, the Er:YAG laser without focus (2.5 mm) showed the most apical sealing, regardless of both the root-end cutting procedure and the association with the Nd:YAG irradiation.
Footnotes
Acknowledgments
We thank CeFOP/IFSC-USP (University of Sao Paulo, Sao Carlos, Brazil) and Vanderlei Salvador Bagnato (CeFOP/IFSC-USP Coordinator) for the technician-scientific support.
Author Disclosure Statement
No competing interests exist.