
Abstract
Introduction
The relation between malocclusion and muscle morphofunctional aspects in the masticatory system is not yet fully understood. 10 Unilateral occlusal alterations in animal experimental models have shown adaptation of the masseter muscle caused by unilateral exodontias, by unilateral occlusal abrasion or by insertion of an unilateral occlusal splint. 11 Previous studies investigated different factors regarding occlusion and masticatory muscle features, among them, muscle spindles, muscle morphology, ultramorphology, electrophysiological recordings, radiographic recordings, and histologic and histochemical analysis. 12 –16 Human and rat occlusion arrangements have intrinsic anatomic and behavioral differences; therefore, caution should be adopted when conclusions of experimental studies in rats are extrapoled to humans; nevertheless, these previous clinical studies suggested that it might be a valid model, and their findings corroborate this view.
It is known that the most important signs and symptoms of TMDs are headache; pain; reduced or impaired mobility of the mandible; TMJ sounds; and tenderness of both the masticatory muscles and the temporomandibular joint (TMJ). 17 Based on these features, the treatment of TMDs involves more than one therapeutic modality to maximize their complementary effects. 18 –20 Among the treatments currently in use, muscle relaxants have been prescribed to reduce skeletal muscle tone and chronic orofacial pain and to alleviate the increased muscle activity. 21 –24 Another therapeutic approach reported in the literature is the use of light sources, including LPT. 25 –35 Nevertheless, no therapy has appeared capable of overcoming the others.
One approach to assess muscular disorders is to analyze muscular fatigue. A major type of fatigue is metabolic, caused directly or indirectly by the accumulation of metabolites (inorganic phosphate, Pi), adenosine diphosphate (ADP), magnesium ions (Mg2+), and reactive oxygen species and by the reduction in substrates (ATP, creatine phosphate, and glycogen). 36,37
It is known that inorganic phosphate, which increases substantially during muscular fatigue, may enter the sarcoplasmic reticulum (SR), combine itself with Ca2+, and form an insoluble precipitate of calcium phosphate (CaPi), leading to reduced SR Ca2+ release and the consequent decline of muscular performance. 38
The “gold standard” used on studies involving muscular fatigue is the intact perfused muscle under central control. For selected muscle groups, it is easy to measure the decline of force, and muscles can be studied with electromyography (EMG) or biopsy. 39 The role of the electron microscopy in the diagnosis of muscular disease is limited. Standards of normality are by no means established, and the accurate interpretation of abnormalities depends mainly on the technical excellence of the material examined. 40,41
Conversely, new methods to assess tissues at the molecular level have been used in several diagnostic applications on biologic samples. Raman spectroscopy is an optical tool that allows less-invasive and nondestructive analysis of tissues, allowing one to obtain precise information on the biochemical composition of the tissue. 42 A previous report 43 demonstrated the presence of lactic acid in tibiae muscle in rats, and another used Raman spectroscopy to investigate the effects of LLLT on the healing of dental implants of rabbits by monitoring the level of calcium phosphate after surgery. 44 Another study reported the use of Raman spectroscopy to monitoring protein structure in muscle. 45
The aim of the present study was to use Raman spectroscopy to measure the levels of CaPi and to use this as marker of muscle fatigue in muscles subjected to occlusal wear and treated with LPT or muscle-relaxant therapy or both in a rodent model.
Methods and Materials
After approval by Animal Ethics Committee of the School of Dentistry of the Federal University of Bahia (Protocol 019/06), 40 male adult Wistar rats weighing 300 ± 350 g were housed at the animal house of the School of Dentistry of the Federal University of Bahia. The animals were kept on 12:12 h light/dark cycle, were fed with the standard pelted diet, and had water ad libitum. The animals were randomly divided into three groups with 10 animals in each: occlusal-wear group (G-1), occlusal wear + LPT (G-2), and occlusal wear + muscle relaxant (G-3). Ten animals were used for baseline data without experimental treatment.
Under intraperitoneal general anesthesia (ketamine, 0.10 mL/100 g, + xylazine, 0.25 mL/100 mg), animals of groups 1, 2, and 3 had unilateral amputation of the left inferior and up molar cusps with a round diamond burr irrigated by saline solution to simulate an occlusal-wear situation. Care was taken not to cause pulp exposure or damage.
The animals of G-2 had the left masseter muscle region shaved and received LPT beginning 24 h after occlusal-wear simulation. The LPT protocol (λ830 nm, 4 J/cm2, 40 mW, φ ∼2-mm spot; Kondortech Laser Unit, São Paulo, Brazil) was performed at two contact points 1 cm apart, at 2 J/cm2 per point, for 2 min (1 min per point). This procedure was repeated every other day for 14 days for half of the animals and for 30 days for half of the animals. Animals of G-3 were treated with a daily intraperitoneal injection of dantrolene (Cristália, SP, 2.5 mg/kg in 0.5 ml of H2O), beginning 24 h after occlusal-wear simulation.
Half of the animals of each group were killed with an overdose of general anesthetics at days 14 and 30 after cusps removal, and the ipsilateral masseter muscles of the sides of the amputated cusps were excised and divided into two samples. One of the halves was routinely processed for light microscopy, and the other half was kept in liquid nitrogen for Raman spectroscopy.
The qualitative light-microscopic analysis was carried out on H&E-stained sections by an experienced pathologist in a double-blind manner and consisted of the assessment of the presence of granulation tissue, inflammatory reaction, and muscle fibers.
For Raman spectroscopy, the specimens were stored in liquid nitrogen to minimize the growth of aerobic bacteria, and because chemical fixation is not advisable because of fluorescence emissions from the fixative substances. 44,46,47 Before Raman study, the samples were warmed gradually to room temperature, and 100 mL of saline was added to the surface during spectroscopic measurements. For Raman measurements, a λ830-nm diode laser (300 mW) provided near-infrared excitation. A spectrograph (250 IS; Bruker Optics, Billerica, MA) with a spectral resolution of ∼8 per centimeter dispersed the Raman scattered light from the sample, and a liquid-nitrogen–cooled deep-depletion CCD (model LN/CCD-1024-EHR1; Princeton Instruments, Tucson, AZ) detected the Raman spectra. The system was controlled by a microcomputer, which stored and processed the data. 44,46,47 The laser power used at the sample was of 80 mW, with a spectral acquisition time of 30 s. Three points were measured of each specimen. All spectra were collected on the same day to avoid optical misalignments and changes in laser power.
The mean value of the intensity of the peak (958 per centimeter, phosphate m 1 ) was determined by the mean of the peaks in this region. This intensity is related to the concentration of CaPi on the muscle. The data were analyzed with MatLab5.1 software (Newark, NJ) for calibration and background subtraction of the spectra. For calibration, the Raman spectrum of a solvent indene with known peaks was used because of its intense bands in the region (800–1,800 per centimeter) of our interest. 44,46,47 The naphthalene spectrum was also measured each time the sample was changed to be sure that the laser and collection optics were optimized. To remove the ‘‘fluorescence background’’ from the original spectrum, a fifth-order polynomial fitting was found to give better results, facilitating the visualization of the peaks of CaPi (−958 per centimeter) found in the muscle. This routine can also remove any continuum, offset background noise, because of CCD readout and cooling.
The differences between groups were tested by using analysis of variance (ANOVA) or t test. Statistical analysis was performed by using Minitab 14.0 software (Minitab, Belo Horizonte, MG, Brazil).
Results
Light microscopy of the masseter muscle showed bundles of muscle fibers separated by thin connective tissue septa, rich in blood capillaries, in all groups. No major differences were observed between specimens killed at day 14 and day 30 (Fig. 1).
Photomicrography of the masseter muscle representing morphologic aspects of all groups (G-2, 14 days), showing the normal aspect of muscle fibers. H&E (40×).
The Raman spectra of the muscles showed prominent vibrational bands related to tissue composition. The value of the mean intensity of each Raman shift of CaPi was obtained from all readings of each group at the muscle surface. The intensity of the Raman shift was directly related to the concentration/incorporation of the CaPi precipitate. We used ANOVA to assess the effects of the treatments on the intramuscular concentration of CaPi as determined by Raman spectroscopy (Table 1). The overall results showed no significant differences as regards the Raman shift of the CaPi on the masseter; this may be attributed to the fact that despite of the use of two treatments, the studied condition was the same. However, when time is considered within each treatment group, and compared with baseline data, a significant difference is found in the concentration of CaPi.
The data from G-1 showed increased intensities of CaPi at day 14 when compared with the baseline, this being observed to the end of the experimental time. However, this was not significant (Fig. 2). G-3 also showed no significant difference in relation to baseline data (Fig. 3).
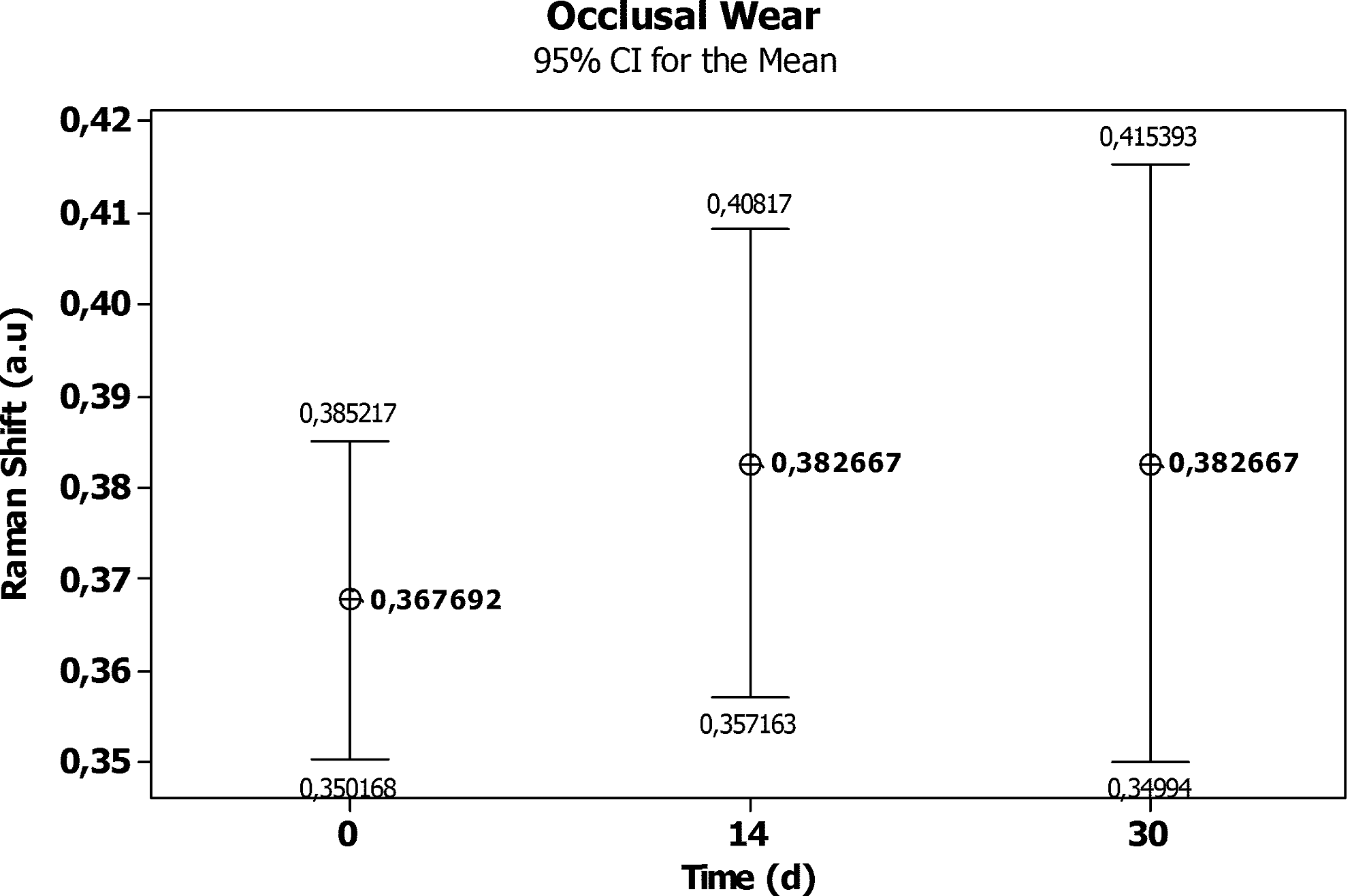
Averages of intensities of CaPi (960 per dentimeter) on masseter muscle on Group 1 (significance level, 0.05).

Averages of intensities of CaPi (960 per centimeter) on masseter muscle on Group 3 (significance level, 0.05).
The data from G-2 showed significant differences (p = 0.001) between the two times. An increase in the level of CaPi at day 14 was detected and was not significantly different from the baseline. However, at the end of the experimental period, a significant decrease in the level of CaPi was noted (Fig. 4). Figure 5 shows the effect of LPT on the reduction of the levels of CaPi at the end of the experimental time. It may also be noticed that, despite the lack of significant differences between groups, a discrete increase in the deposition of CaPi in groups G-1 and G-2 was found at day 14, significantly reduced only in G-2 at the end of the experimental time. G-2 shows significant differences when compared with the baseline data as well as with G-1.
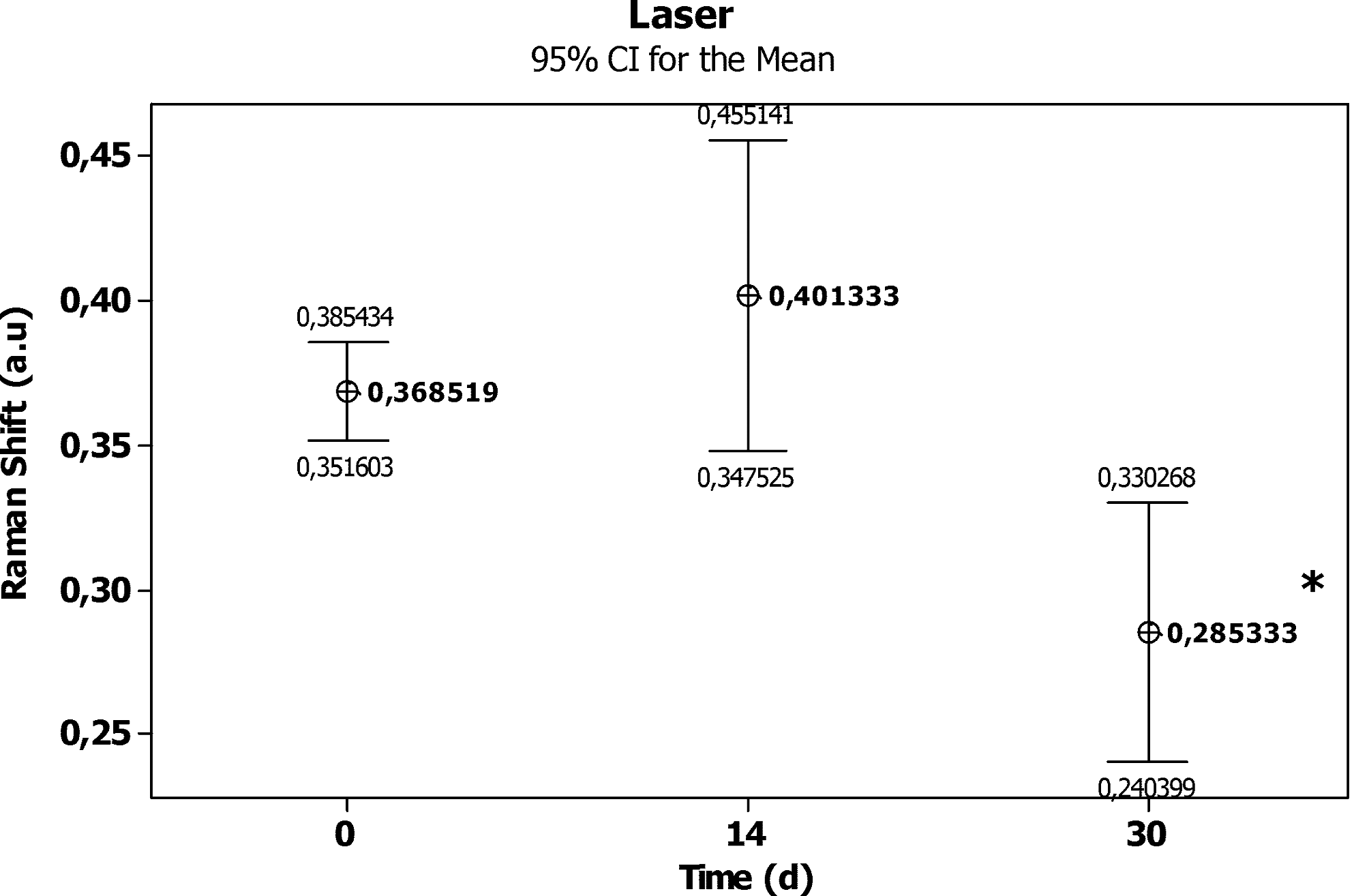
Averages of intensities of CaPi (960 per centimeter) on masseter muscle on Group 2 (significance level, 0.05).
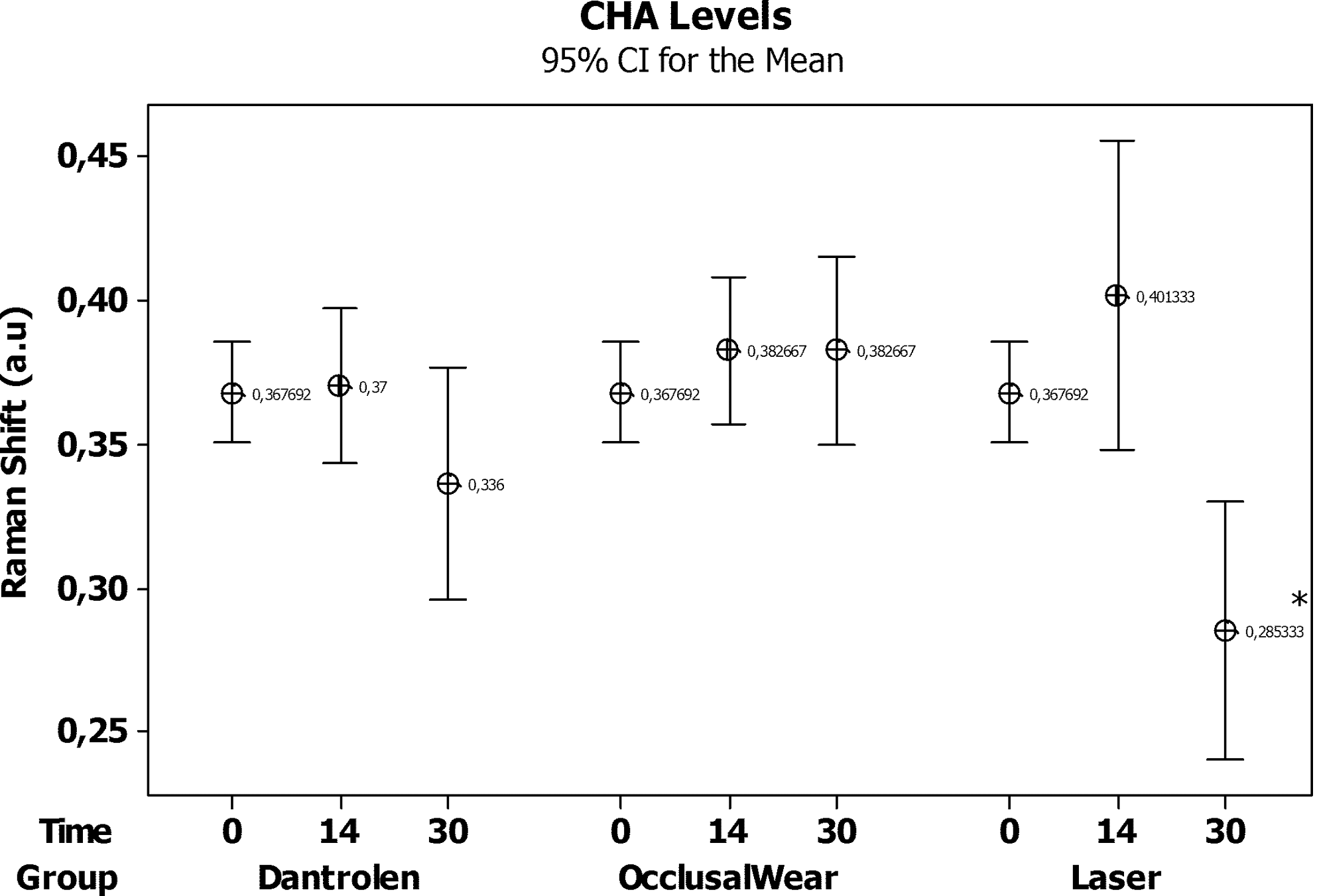
Averages of intensities of CaPi (960 per centimeter) on masseter muscle compared with baseline (significance level, 0.05).
Discussion
The present study failed to show any significant difference between the groups as regards the morphologic aspect of the injury (left side). It may be inferred that the injury was similar in all groups and that the morphologic aspect of the injured area was not significantly different from the observed prior trauma (baseline). The fact that no significant morphologic differences were found between the experimental groups may be due to the sample size as well as to the physiologic mechanisms of adaptation, low-light microscopy resolution, and the relatively short experimental time. It is possible that long-term trauma may cause significant differences.
Conversely, we found such differences in their behavior when we studied muscle fatigue by using the measurement of the levels of CaPi as determined by Raman spectroscopy. To our knowledge, this is the first report of such a finding, and our results demonstrate the importance of deep awareness in regard to the muscular changes that occur in TMDs.
In the present study, we used the occlusal-wear animal model to simulate alteration of the tooth occlusal status similar to that observed in patients with missing teeth. This model has been previously used, 10 –16 resulting different degrees of morphologic and physiologic alterations in masticatory muscles, especially on the masseter. Previous studies showed that the ipsilateral muscles to occlusal wear have more injuries than do the contralateral muscles. 21,22
In the present investigation, all groups showed similar Raman intensities of the peaks of CaPi. The animals submitted to occlusal wear, despite showing the highest Raman intensities, were not significantly different from the others (Table 1). This aspect may be indicative of the lack of a direct cause–effect relation between occlusion and muscular injury.
Conversely, if we consider that all groups had the same trauma (occlusal wear), we may assume that the increase of CaPi levels seen at day 14 was due to the occlusal trauma. However, this increase was not significant when compared with the baseline data. This aspect may be indicative of the lack of relation between occlusal trauma and TMJ disorders. It seems that occlusal trauma was not capable to alter significantly the metabolism of the muscle. Several factors may have influenced our results, including the possibility that the occlusion itself may not show a significant influence on the metabolism of masticatory muscles, particularly in relation to the masseter; unilateral occlusal wear was not able to cause significant muscular damage; the presence of contralateral teeth may have kept muscular tonus; or, as mentioned previously, the time of observation might not have been enough to cause severe trauma on the muscle; or the small sample size.
Another aspect mentioned in the world literature is that animals may develop an engram, a muscular motor-pattern adaptation of movement. This adaptation is merely a neuromuscular adjustment of an abnormal situation aiming to keep the teeth in their normal relation; 48 the muscle would be able to bring back its tonus, reestablishing its cell metabolism and the levels of metabolites. We would then assume an initial alteration of the metabolism, which would be followed by normal functional restoration.
Although the influence of occlusion on mastication is well documented elsewhere in the literature, its influence on and the physiopathologic mechanism of masticatory muscles are not so well understood. 5,7,8 In this context, therapeutic approaches aim to increase patients' awareness of the etiology of the symptoms; to promote muscular relaxation; to reduce muscular hyperactivity and reestablishment of both muscle and joint movements; to relieve pain, spasm, and edema; and to allow the recovering of normal function. 9,17,20,49
Treatments such acupuncture, exercises, massages, drugs, thermal therapy, electric stimulation (TENS), ultrasound, occlusal splints, and laser therapy (LLLT) have been used to treat this complex pathology. 19,50 Some of these methods were previously evaluated, and contradictory outcomes have been reported regarding their effectiveness in treating TMDs. 20
Figure 5 shows the different behaviors of untreated (G-1) and treated (G-2 and G-3) subjects. G-1 showed an insignificant increase of CaPi levels in relation to the baseline data at day 14. This increased level was maintained up to the end of the experimental period. Conversely, subjects in groups G-2 and G-3, in which the occlusal trauma was followed by one of the treatments, also had an initial increase in the level of CaPi at day 14 that was followed by a reduction up to day 30. However, only animals treated with LPT (G-3) showed a significant reduction at this stage when compared both with its baseline and with G-1. This may be indicative of a protective effect of laser therapy. The lack of previous reports using Raman spectroscopy as assessment of the chosen animal model makes a full understanding of our findings difficult.
Even though the occlusion-wear model has been used in previous studies, 10,15 Raman measurement had not been used in such areas, so ethical constraints prevented us from using a larger sample, as no previous reported indication of our model existed in the literature. This is the first report of such a finding, and our results demonstrate the importance of deep awareness in regard to the muscular changes that occur in cases of TMDs. Even with a small sample, we were able to show significant statistical differences between the groups. Based on this outcome, it is possible to pursue several studies regarding laser, TMJ, and laboratory research.
On groups G-2 and G-3, we used two treatment approaches known to have a role on TMDs of both occlusion and muscular origin. The use of muscle relaxants and LPT are reversible therapies that have been mentioned in the literature as means of treating TMDs. 21,24 –26 Because of the difficulty of determining the etiology of the TMD, definitely multifactorial, and the possibility that the symptoms are secondary to some other masticatory disorders, the initial treatment is then reversible. 20,24,30 The success of any therapy depends on the expertise of the clinician, as well as on the elimination of possible etiologic factors. No single treatment modality has been proven to be better than any other at treating TMDs. 51,52
In myogenous disorders, we assume that elevated intracellular Ca2+ levels influence the pathophysiology of TMDs. 21 It could be assumed, therefore, that drugs interfering with the release of Ca2+ in muscle fibers may have a beneficial effect in myogenous TMDs by interrupting the vicious cycle that is held responsible for persistent muscle hypercontraction. 23,24
Previous studies have shown that the use of the muscular relaxant dantrolene was capable of reducing or protecting muscular fibers from developing fatigue or even from tissue injury. 23,24 A previous study using dantrolene (10 mg/kg) found reduced numbers of vacuolated muscle fibers, nearly abolished the occurrence of myofibril hypercontraction and intermyofibrillar edema, and showed a significantly decreased level of Ca2+ in the tissue. 21 This effect was attributed to a partial blocking by the drug of the release of Ca2+ by the sarcoplasmic reticulum. 23
In this study, although no statistically significant difference was found, the use of this drug resulted in lower Raman intensities than those in the occlusion-wear group. This may be because this drug decreases skeletal muscle excitation–contraction and consequently the depletion of ATP and creatine phosphate. The Pi in skeletal muscle originates mainly from these two metabolic products.
This drug is not usually used for TMJ; therefore, it does not have an established dosage for this purpose. The dose of 2.5 mg/kg used in this study was the earlier dose for malignant hyperthermia, a rare genetic disorder, and is 4 times less than that used by Bani et al. 21 (2001) and may have not been enough to have caused important alterations in the Ca and Pi association.
Many reports exist in the literature on the use of laser light, but its effects on biologic tissues remain controversial and inconclusive. 27,28,31 –35,53,54 Our results show that the use of this therapy results in a long-term benefit for the masseter muscle under occlusal wear.
LPT is a new therapy compared with others that have been used to treat muscular pain, but the biologic mechanisms behind the beneficial results observed in clinical trials remain unclear. 29,49 LPT may be carried out at different wavelengths of both the visible and the near-infrared spectra (λ632.8, λ650, λ805, and λ904 nm). 25,26,31 –35,53,54 In contrast to other studies, 49,50 this study used λ830 nm with 4 J/cm2 and 40 mW because this protocol in infrared wavelengths had been successful in reducing pain in patients with TMD and increased the active range of motion and improved muscle tenderness. 53,54
Our results showed that the use of laser light reduced the level of CaPi within 30 days when compared with baseline and the occlusion-wear group. This may indicate that laser light created a protective mechanism against fatigue. Laser-irradiated subjects had a significantly lower level of CaPi at day 30 than at day 14. This may be suggestive of a long-term effect of the treatment caused by a sustained delivery of energy to the muscle. Because the laser group at 14 days had the highest outcome, it is possible that 28 J at 14 days was insufficient to protect muscle tissue against fatigue, and the use of a minimal-treatment dose (56 J) may be necessary to cause such a response from the muscle.
Although the findings of the present study were restricted to a specific set of parameters and the optimal treatment parameters (for example, wavelength, dosage, number of treatment sessions) have not been agreed on, 27,30 it has been shown that the beneficial results achieved previously are observed with the use of IR wavelengths. 34,49,50,53,54
Our results do not exclude occlusion as a cause of TMDs but show that LPT may be considered an effective therapeutic approach to treat such conditions. Although these are preliminary findings, they suggest that Raman spectroscopy is a valuable instrument for the measurement of the metabolic products seen in skeletal muscles under fatigue, as well as to study the relation between occlusion and muscle dysfunction. It may be concluded that occlusal alteration did not caused morphologic alterations of the masseter muscle under fatigue but resulted in changes of the level of CaPi that were less compromising when the laser light was used.
Footnotes
Author Disclosure Statement
No competing financial interests exist.