
Abstract
Introduction
Despite all the developments, demineralization around orthodontic brackets still presents a major problem for orthodontic patients. Contraction in the degree of polymerization causes shrinkage strain, marginal gaps, and eventually marginal leakage (microleakage) at the tooth–adhesive interface. 3 Microleakage between composite–enamel and/or composite–bracket interfaces may cause serious caries.
Caries development in the form of so-called “white-spot lesions” on the labial surfaces is a serious side effect of treatment with fixed appliances. 4,5 The prevalence of white-spot lesions after fixed orthodontic therapy is reported to range from 50% to 70%. 6 For that reason, Ogaard and Rolla 6 found that fluoride applications have limited effect on preventing decalcification. They suggested that fluoride agents could be further improved by the adding antibacterial agents.
Another attempt is using chlorhexidine (CHX) solutions. CHX solutions are most widely used as oral antiseptics in clinical dentistry. This is based on their low toxicity and high spectrum of antibacterial activity. 7 This solution is the most potent antimicrobial agent to combat Streptococcus mutans. 8 It has also been suggested that CHX combined with thymol in a varnish could have lower bacterial activity in plaque while maintaining an ecologic balance, have excellent adsorption to tooth surface, and be well tolerated. 9 Its application does not impair the sealing ability and bond strength of adhesive materials, 10 although in specific situations, some studies showed interference of chlorhexidine in adhesion. 11,12
Adhesive systems that possess antibacterial activity may be useful for eliminating harmful effects caused by bacteria and may contribute to better prognoses for minimal restorative treatments of dental caries. 13 Imazato et al. 14 previously reported incorporation of an antibacterial monomer 12-methacryloyloxydodecylpyridinium bromide (MDPB) into a self-etching primer. The experimental primer containing MDPB has been demonstrated to exhibit antibacterial effects against oral bacteria and a bond strength similar to that of the parent product. 15 Accordingly, the experimental primer is considered to be beneficial in eliminating the harmful effects caused by the bacteria remaining after cavity preparation. 16 Based on the results obtained for this experimental material, a single-bottled 5% MDBP-containing primer was developed, and an adhesive system using this primer was commercialized as CPB.
A search continues for materials and techniques that ensure adhesion to tooth structure and minimize the potential for microleakage. In dentistry, laser technology is one of the last developments that may have an impact on the reduction of microleakage. 17 The KTP laser emitting at 532 nm, representing a frequency-doubled Nd:YAG device, has been introduced mainly for tooth-bleaching procedures in dentistry and can be delivered through a wide range of fibers in a constant or a pulsed mode. 18 This laser has also been used for some other dental applications similar to Nd:YAG laser, including root-canal disinfection, treatment of dentine hypersensitivity, and soft-tissue surgery.
In the clinical situation, long-term bracket-to-enamel bond strength may be important for successful and effective patient treatment. Long-term bonding durability was maintained with the thermocycling test. 19 Thermocycling is used to simulate clinical conditions and to enhance the human applicability of bonding agents.
The purpose of this study was to assess the microleakage of adhesive–bracket and bracket–enamel interfaces after applying CHX, CPB, and KTP laser to etch the enamel with the thermal-cycle procedure. This is the first study to observe microleakage under metal brackets after KTP laser irradiation to etched enamel surfaces in orthodontics.
Materials and Methods
Sixty caries-free and intact human upper premolars readily available and extracted for orthodontic purposes were collected. Teeth with hypoplastic areas, cracks, or gross irregularities of the enamel structure were excluded from this study. The criteria for tooth selection dictated no pretreatment with a chemical agent such as alcohol, formalin, hydrogen peroxide, and so on. The teeth were removed from soft-tissue remnants and calculus, and before the starting procedure, the surface of each tooth was cleaned and polished with pumice and rubber cups for 30 sec. The teeth were randomly separated into three experimental groups and one control group, each containing 15 teeth and stored in distilled water until the bonding procedure.
The groups received the following bracket-bonding procedures: Group 1 (control group). No antibacterial solution was used. A 37% phosphoric acid gel (3M Dental Products, St. Paul, MN) was used for acid etching for 15 sec. The teeth were rinsed with water for 15 sec and dried with an oil-free source for 15 sec. In all etched cases, the frosty white appearance of etched enamel was apparent. Transbond XT bonding system (3M Unitek, Monrovia, CA) was used each tooth, according to the manufacturer's instructions. Group 2. A 37% phosphoric acid gel (3M Dental Products) was used for acid etching for 15 sec. The teeth were rinsed with water for 15 sec and dried with an oil-free source for 15 sec. A 2% CHX cavity cleanser (Drogsan, Ankara, Turkey) was applied with a minibrush tip, placed in contact for 60 sec, and then dried with mild air flow. Transbond XT bonding system (3M Unitek) was used each tooth according to the manufacturer's instructions. Group 3. A 37% phosphoric acid gel (3M Dental Products) was used for acid etching for 15 sec. The teeth were rinsed with water for 15 sec and dried with an oil-free source for 15 sec. Teeth were irradiated at 1 W, 11 J/cm2, with KTP laser (Smartlite D; Deka, Calenzano Firenze, Italy) and the laser beam was delivered by a 200-μm-diameter optical fiber for 15 sec. The distance between the fiber and teeth was 1 mm in a perpendicular position. Transbond XT bonding system (3M Unitek) was used on each tooth according to the manufacturer's instructions. Group 4. The Clearfil Protect Bond (Kuraray, Osaka, Japan) self-etching primer was applied to teeth and left in place for 20 sec. After drying the etched surface with mild air flow, the bonding agent was applied on the etched-primed enamel and light-cured for 10 sec.
Orthodontic upper premolar metal brackets (Generus Roth, GAC, NY) were used in this study. The average bracket surface area of the bracket base was determined to be 12.4 mm2.
All the brackets were bonded with the same composite resin, Transbond XT (3M Unitek) and light cured for 20 sec from the mesial and distal sides of the brackets, respectively. All light curing was performed with a visible-light curing unit (Hilux; 40 sec/1-mm increment; Benlioğlu Dental, Ankara, Turkey). The curing light built-in radiometer was used to check for light efficiency before starting each tooth.
Specimens were stored in distilled water for 24 h at 37°C, after which thermal cycling was performed at 5°C to 55°C for 500 cycles with a dwell time of 30 sec and a transfer time of 10 sec, in accordance with ISO/TR 11405 recommendations. 20
The thermal cycle is used to simulate clinical conditions and to enhance human applicability of bonding agents. Before dye penetration, the apices were sealed with sticky wax, and the specimens were coated with two consecutive layers of nail varnish up to 1 mm from bracket margins. Specimens were then immersed in 0.5% basic fuchsin solution (Wako Pure Chemical Industry, Osaka, Japan) for 24 h. After thorough rinsing with distilled water, the samples were air-dried, and each specimen was sectioned longitudinally with a low-speed diamond disk (Isomed Buehler, Lake Bluff, IL) with water coolant in the buccolingual direction. The most-stained half of the tooth was used to evaluate the microleakage. All sections were examined by two experienced investigators under a stereomicroscope (SMZ 800; Nikon, ) at 20× magnification in a blinded fashion. Each section was scored for microleakage at the incisal and gingival levels along both interfaces (bracket–adhesive interface and adhesive–enamel interface). Scoring was done according to the following criteria
34
: Score 0: No dye penetration between the bracket–adhesive or adhesive–enamel interface. Score 1: Dye penetration restricted to 1 mm into the bracket–adhesive or adhesive–enamel interface. Score 2: Dye penetration into the inner half (2 mm) of the bracket–adhesive or adhesive–enamel interface. Score 3: Dye penetration into 3 mm of the bracket–adhesive or adhesive–enamel interface.
In cases of disagreement between scoring, consensus was obtained by using the greater score. Statistical evaluation of microleakage scores was subjected to a one-way ANOVA and among the test groups was performed by Kruskal–Wallis test with significance set at p = 0.05.
Results
The results indicated that all the groups exhibited microleakage between either the adhesive–enamel interface or the bracket–adhesive interface. When adhesive–enamel interface along both gingival and incisal microleakage was considered, no statistically significant difference was found among all groups (p > 0.05) (Table 1). In addition to this, no statistically significant difference was observed among all groups in terms of microleakage when the bracket–adhesive interface along both gingival and incisal was considered (p > 0.05) (Table 2).
p = 0.227, NS (p > 0.05). p = 0.353; NS (p > 0.05).
SD, standard deviation; NS, not significant.
p = 0.861, NS, (p > 0.05). p = 0.798, NS, (p > 0.05).
SD, standard deviation; NS, not significant.
The lowest microleakage scores were observed in the control group (Fig. 1), and the highest microleakage scores were observed in the 2% CHX group (Fig. 2).
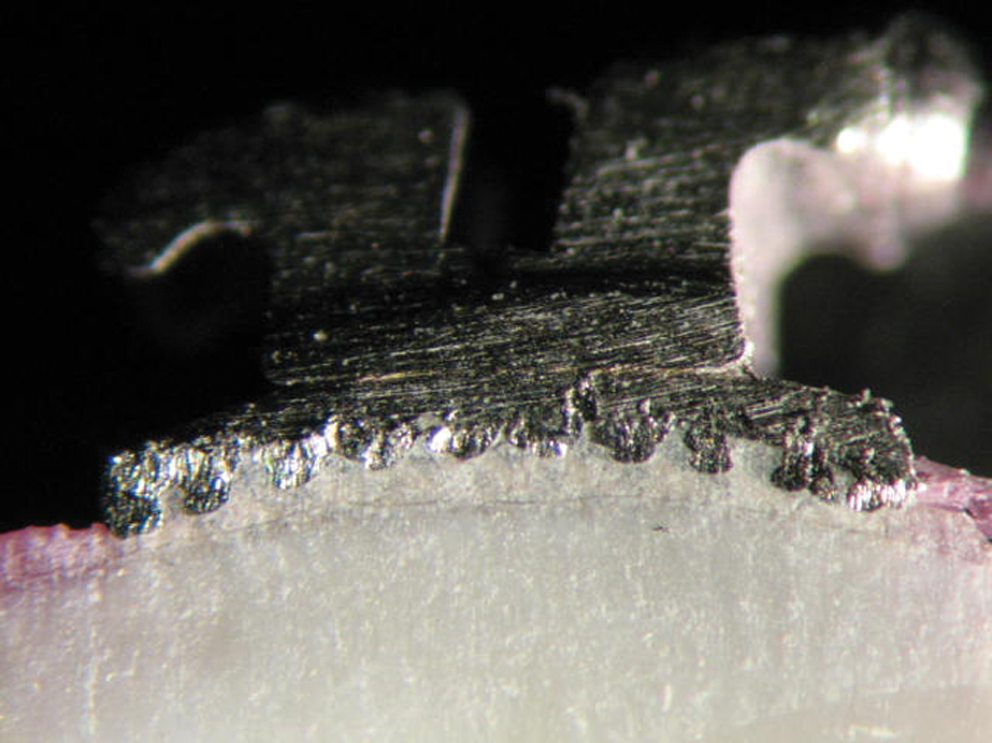
No microleakage under a metal bracket.
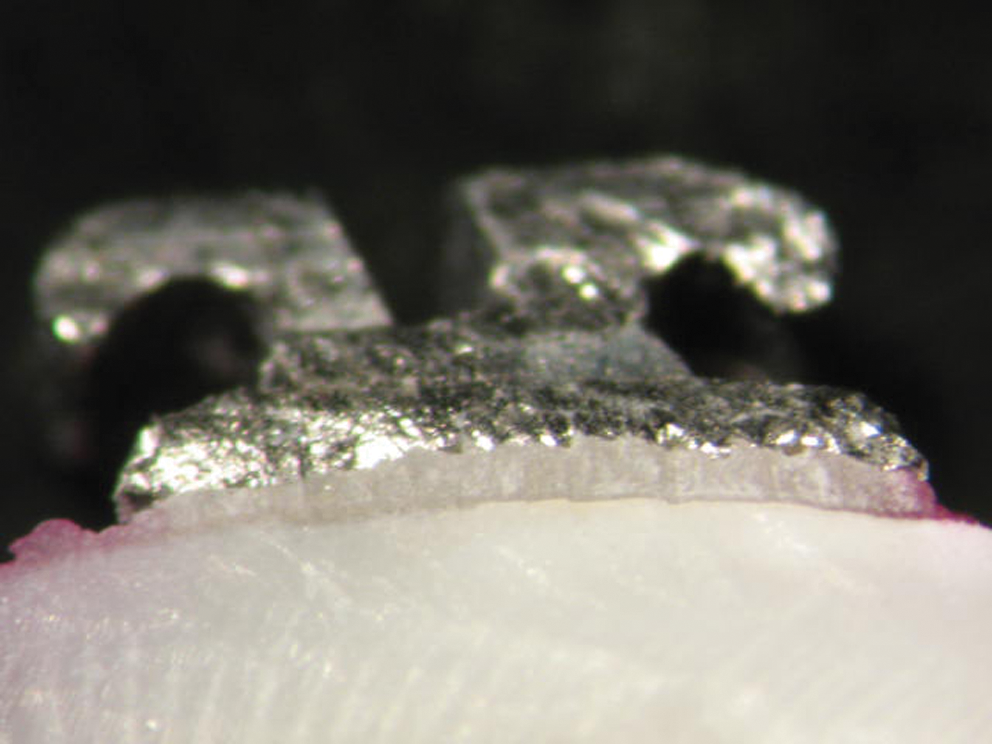
Microleakage under a metal bracket.
Discussion
For restorative dentistry clinics, microleakage is the seeping and leaking of fluids and bacteria between the tooth or restoration junction and the interface. Microleakage increases the likelihood of recurrent caries and postoperative sensitivity. From the orthodontic point of view, microleakage presents the likelihood of formation of white-spot lesions on the enamel at the adhesive–enamel interface. 21 O'Reilly and Featherstone 22 showed that visible white lesions can develop within 4 weeks. Although microleakage-oriented caries is a well-documented entity in the restorative dentistry literature, the potential of caries adjacent to and beneath orthodontic brackets still remains an underestimated threat to the permanent tooth, especially with regard to long-term fixed therapy.
In this study, basic fuchsin was used to detect microleakage on the gingival and incisal sides. Different methods have been used to disclose microleakage. Dye leakage is probably the most common method used. The principal advantages of this technique are its low cost and ease of application. 23
In the present study, a sequence of temperature changes from 5°C to 55°C for 500 cycles with a dwell time of 30 sec was chosen, as this was believed to represent a suitably discriminatory challenge. The thermal-cycling test involves subjecting specimens to extreme temperatures that simulate intraoral conditions. Thermal alterations induce stress between a tooth substrate and a restorative material at the bonding interface. Therefore, thermal stress of the adhesive material may cause gaps between the adhesive material and enamel surface and lead to microleakage. 24
Phosphoric acid is one of the best methods to use in bonding resins to enamel. An optimal etching pattern is achieved by using phosphoric acid concentrations of 30% to 40% for 20 to 30 sec on untreated enamel. The use of acid to increase microscopic roughness, by selectively removing mineral crystals, to improve the retention of composite restoratives has become a standard process for dental preparation. 25 In the present study, no statistically significant difference was found between all groups, when the adhesive–enamel interface and the bracket–adhesive interface of both gingival and incisal microleakage scores were compared. Nevertheless, the 37% phosphoric acid group showed the lowest mean microleakage scores of all groups. Our results were similar to those of previous studies. 26 –28 However, a potential disadvantage of enamel etching is the complete removal of the smear layer and exposure of dentinal tubules. Acid etching results in chemical changes that may modify the organic matter and decalcify the inorganic component. 29 The disadvantages of etching with phosphoric acid are loss of surface enamel from 5 to 10 μm and weakening of the subsurface enamel. 30 As a result of this demineralization, enamel becomes more susceptible to caries attack, which is induced by plaque accumulation around the bonded orthodontic attachments. 28
Adding CHX to the sealant applied to the etched enamel surface could add increased protection around the bracket periphery. 27 In the present study, when the microleakage scores between adhesive and enamel surfaces, and the bracket and adhesive surfaces from incisal–gingival sides were compared, the differences between CHX group and other groups were not found to be statistically significant (p > 0.05). However, 2% CHX showed the highest mean microleakage scores of the groups. Previous studies compared the application 2% CHX to the enamel surface with control groups and did not find any differences on shear-bond strength values. However, these studies did not consider the microleakage after application of 2% CHX on an enamel surface. 31 Demir et al. 32 emphasized that an interaction may occur between CHX and the enamel-bonding surface. Our study showed that the application of 2% CHX may cause a greater microleakage than the other application methods.
The bonding system, CPB, is a two-step self-etch adhesive system, composed of a self-etching primer containing the antibacterial monomer, MDPB, and a fluoride-releasing adhesive. 33 The antibacterial monomer MDPB is a polymerizable biocide and has strong bactericidal activity against oral bacteria. 14,33 The present study showed acceptable microleakage scores. CPB mean microleakage scores were similar to 37% phosphoric acid scores. When the adhesive–enamel interface and bracket–adhesive along both gingival and incisal microleakage were compared, no statistically significant difference appeared among all groups. Our results were in accordance with the study of Arhun et al. 34 In orthodontic applications, polymerization shrinkage and subsequent microleakage is less a concern. 13 Orthodontic adhesive layers are very thin, and the adhesive at the edges of the bracket absorbs some shrinkage. In this way, the bracket is free floating, and the shrinkage can pull the bracket closer to the enamel. 35 That combination of etchant and primer into one system is advantageous, in that it reduces the application time and chair time, and this shorter chair time reduces the risk of saliva contamination.
In the present study, KTP laser energy was used after enamel etching with 37% phosphoric acid. This is the first study to assess microleakage beneath metal bracket with KTP laser, and this laser was used for enamel surface disinfection before the bracket bonding. We found no statistical difference between the KTP laser group and the other groups for microleakage. Also, the KTP laser and 37% phosphoric acid showed similar results. This study is not comparable with literature because no previous studies exist. However, previous studies compared the shear-bond strength of laser irradiation with acid etching. 36 –39
Yamamoto and Ooya 40 indicated that human enamel irradiated with the Nd:YAG laser was more resistant to acid decalcification than was an unlased enamel. Hossain et al. 41 showed that Nd:YAG laser irradiation can sufficiently melt and solidify the enamel and dentin surfaces and thus enhance resistance to artificial caries-like formation. We think that effect of KTP laser in the prevent of enamel caries and surface disinfection could be coupled to the potential of the Nd:YAG laser beam. Thus, KTP laser application on the enamel before the bracket bonding should be further analyzed to promote its use in dentistry.
Conclusion
The results indicated that all the groups exhibited microleakage between either the adhesive–enamel interface or the bracket–adhesive interface.
The lowest microleakage scores were observed in the control group.
No statistically significant difference was observed among all groups in terms of microleakage when the bracket–adhesive and adhesive–enamel interfaces along both gingival and incisal surfaces was evaluated (p > 0.05).
KTP laser and CPB showed lower mean microleakage scores than did CHX under metal brackets.
We suggest that antibacterial pretreatments such as CHX, KTP laser, and CPB can be used on the enamel and before placing the bracket, and these applications can prevent carious challenge under brackets.
Footnotes
Author Disclosure Statement
No competing financial interests exist.