
Abstract
Introduction
Notwithstanding the evidences of neurological involvement, the etiopathogenesis of BMS is still unknown, and no efficient treatment is available. 9 A safe and accessible treatment is desired as an alternative for this limited range of therapies. Under this scenario, low-level laser therapy (LLLT) emerges as a potential candidate for this role. Several chronic painful conditions have been successfully treated with laser. The efficacy of LLLT has been demonstrated in chronic low back pain, 10 chronic myofascial pain syndrome in the neck, 11 and chronic neck pain. 12 With regard to burning sensation on the tongue, it has been reported that laser irradiation of the stellate ganglion, located anteriorly to the transverse process of the 7th cervical vertebrae, decreased the intensity of the pain. This effect would be related to the inhibition of the sympathetic outflow resulting in the normalization of the decreased blood flow in the affected area, leading to pain relief. 13
Several studies have been performed searching for the mechanisms involved with the analgesia induced by the laser. Increased production of serotonin, 14 an increase in ACTH and/or β-endorphin plasma levels, 15 and in β-endorphin precursor mRNA expression 16 have been reported as the mechanisms for laser-induced pain relief. Recently, it has been shown that low-level laser irradiation of neurons induced morphological changes (varicosity formation, mitochondrial clustering formation, and microtubule disarray), reduced the mitochondrial membrane potential, and blocked the fast axonal flow. The authors suggested that these changes led to the neural conduction blockage. 17
LLLT is a non-invasive, non-pharmacological alternative for treatments of painful conditions, with minimum adverse events. The evidence to date encourages investigation of LLLT for chronic painful disease where this is no effective treatment available, such as in BMS. Under this picture, this study aimed to investigate the effects of LLLT on the treatment of patients with BMS. In addition, the laser effect was evaluated on different affected oral sites. The null hypothesis tested was that laser therapy would not provide a reduction in symptoms.
Methods
Subjects
Thirteen subjects afflicted with a burning sensation in the mouth were selected at the Clinic of Oral Diagnosis of the Dentistry School at the University of São Paulo. Medical and dental histories were carefully taken, and a thorough oral inspection was performed. The inclusion criteria were as follows: complaint of burning sensation, oral mucosa with normal clinical appearance, not currently undergoing other treatments for BMS, normal laboratory results (full blood count, blood sugar), and no signs of hyposalivation. Hyposalivation was considered as values below 0.1 mL/min 18 for unstimulated whole saliva. Flow rate was assessed by collecting whole saliva during 15 min in a graduated beaker tube, after discarding the initial mouth content, with patients seated in a private room during the time of collection.
The local ethics committee approval was given, and written consent from all subjects was obtained. During the study, one patient referring to symptoms on the tongue presented with geographic tongue and was excluded. Another patient missed one treatment session and was withdrawn from the study. The remaining 11 patients (10 female and one male, aged 37–74 years, mean 64 years) presenting with a total of 25 sites affected by the burning symptom completed the study. Five subjects (45.5%) complained about hyposalivation, and five about taste impairment.
Symptoms evaluation
Burning intensity was evaluated in each referred region using a 100-mm visual analog scale (VAS), where 0 means no burning sensation and 100 the worst burning imaginable. The subjects were asked for rating the pain on separated VAS (VASsession) at the end of the laser treatment and at the 6-week follow-up. The baseline value of VAS (VASbaseline) was the data collected before the first laser irradiation. The percentage of improvement in symptoms was calculated as follow:
Treatment
The treatment consisted of weekly laser application for three consecutive weeks. The device used in this study was a class 3B diode infrared laser (Quantum, EccoFibras, Campinas, Brazil) with wavelength of 790 nm in a continuous wave mode, with a spot size of 0.03 cm2. The exposure time was calculated based on the fluence of 6 J/cm2, the radiant power of 120 mW, and the area to be treated. Each affected site was measured by drawing the affected area on graph paper that was overlaid on the mucosal surface. The laser was applied to each part of the mouth, keeping the probe in contact with the mucosal surface (Fig. 1), and the entire affected area was scanned during the irradiation. At each irradiated point, the time of exposure was 10 s and the energy delivered was 1.2 J. LLLT was performed separately on each affected site, and consequently the symptomatology was evaluated at every treated region. Thus each referred site was considered an independent variable.

Infrared photograph of the tongue irradiated by the laser (λ = 790 nm).
Protective glasses appropriated for 790-nm wavelength were used by patient and professional, as required for this class of laser. The output power of the equipment was measured using a calibrated power meter three times during the course of the study.
Statistical analysis
The variable responses used in the present study, VAS and percentage of improvement in symptoms, were summarized as mean and standard deviation. All data were analyzed with the Shapiro–Wilk W-test to assess the normality. Since data did not turn out to have normal distributions, the Friedman ANOVA followed by the Wilcoxon matched pairs test were applied to analyze the difference between the groups. For all tests, significance was accepted at p < 0.05. The software used was Statistica (StatSoft, Inc., Tulsa, OK).
Results
Mean VAS values of the 25 treated sites decreased significantly from the baseline data to the end of laser therapy and to the follow-up period. However, no difference was found between the end of laser therapy and the follow-up period (Fig. 2). The percentage improvement in VAS score was 80.4% at the end of the treatment and 63.4% after 6 weeks, with no significant difference between these two instances (p = 0.2). At the follow-up, five sites presented complete remission of the symptoms: two sites (palate and upper lip) of a subject with four sites affected, and all sites (lower lip, upper lip, and tongue) from another subject. Seventeen regions improved (11 were superior to the mean value), and three worsened. No patients reported any side effects.

Mean VAS data evaluated during the study. The p-value was calculated using the Wilcoxon test. Bars represent the standard deviation.
The tongue was the site most affected by BMS, afflicting 10 of 11 subjects (91%). Seven subjects (64%) presented burning sensation on the lower lip, four (36%) on the palate, and four (36%) on the upper lip. Three subjects reported one site affected by the burning symptom, four reported two sites, two reported three sites, and the other two reported four sites. Mean VAS values of these sites are presented in Fig. 3.
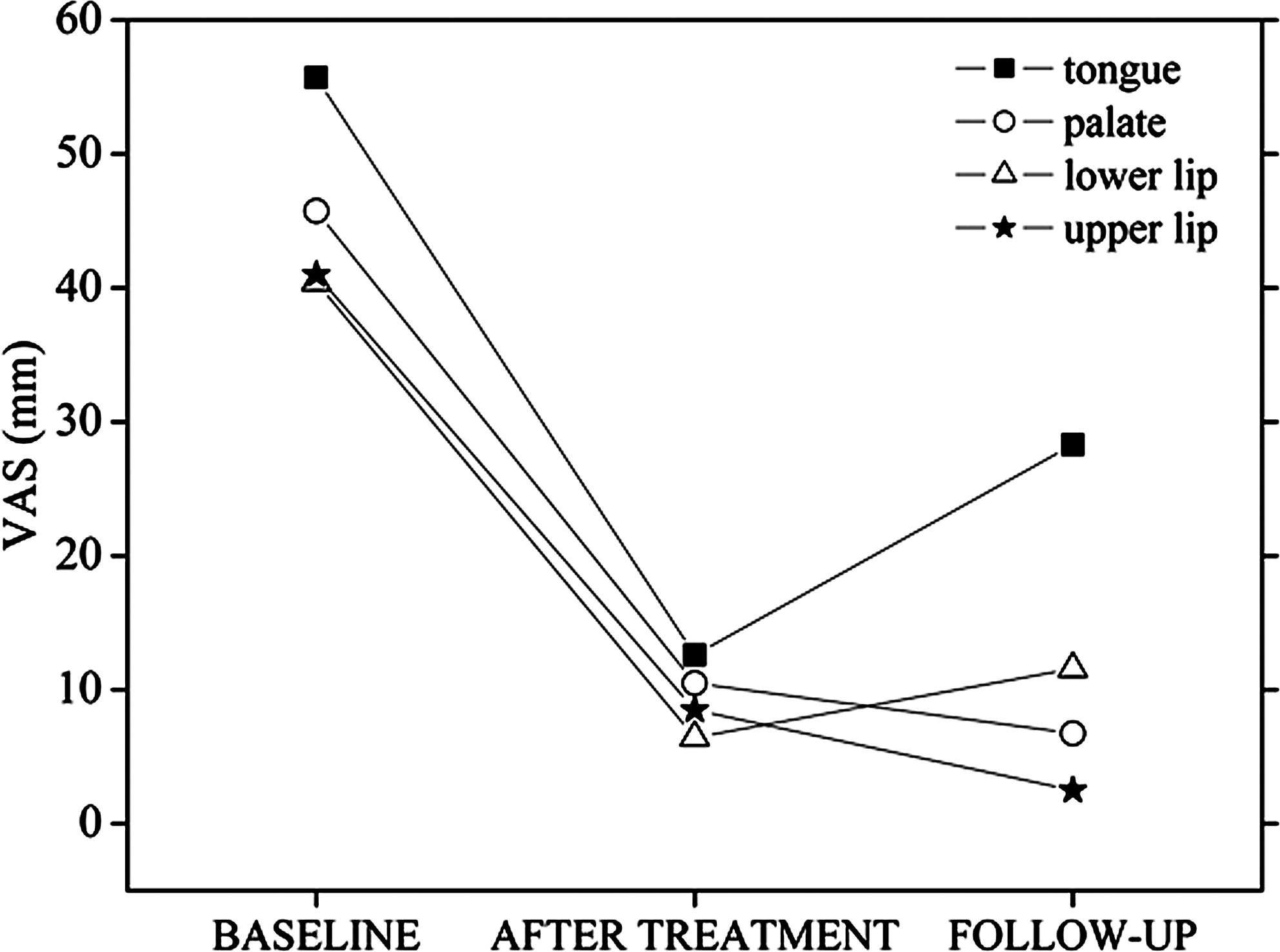
Mean VAS values of each mucosal site in three moments of the study.
Analysis of the VAS data pointed out distinct effects in the different regions treated on the same patient. The tongue was the only region to present a partial return of the burning sensation (Table 1) 6 weeks after the treatment (p = 0.026). The effects achieved after laser sessions were maintained at the 6-week follow-up on the palate (p = 0.24), the lower lip (p = 0.18), and the upper lip (p = 0.11).
Different letters represent statistically significant differences (p < 0.05); n is the number of irradiated sites.
Discussion
LLLT was effective in reducing symptoms caused by BMS, decreasing 80.4% of the burning sensation with three laser sessions. During the 6-week follow-up period, a partial return of the symptoms was observed only on the tongue. Despite this fact, the mean burning intensity was reduced in all treated sites by the laser therapy.
One of the possible mechanisms associated with the reduction in symptoms could be the analgesia induced by serotonin 14 and β-endorphin production 16 following LLLT. However, it is not expected that these biological events would last for a long period. 19 Moreover, had the effect been promoted by neural conduction blockage after irradiation, the relief of symptoms would be estimated to last just 24 h. 17 The maintenance of the results observed at the 6-week follow-up suggests a different or an additional mechanism of action for the laser therapy in BMS. In fact, the lack of information on the etiopathogenesis of this disease 20 limits the comprehension of the possible mechanisms involved in the observed effects.
The improvement in symptoms observed in this pilot study showed an irregular pattern among subjects and treated sites. Six weeks after the treatment, three treated sites deteriorated, while 16 showed a percentage improvement to 63.4%. Assuming the neurological etiology in BMS pathogenesis, these observations could be related to the involvement of different systems, mainly the peripheral and central nervous systems.
Interestingly, the tongue was the only site that did not maintain the improvement achieved at the end of the treatment, even though a 45.5% relief in symptoms was obtained during the follow-up period. Taking into account the sensorial innervations of the regions treated in the present study, the tongue has a more complex neural structure than the other sites due to the presence of the taste buds. In addition, the anterior portion of the tongue is innervated by two cranial nerves: the trigeminal nerve and the facial nerve. This neural complexity could be hypothesized as the reason for the different effects observed between the tongue and the other sites treated with the laser. Besides, a peripheral sensory neuropathy caused by diffuse degeneration of nerve fibers was described in the tongue of patients affected by BMS. 7 If this neural alteration was present, the laser could have caused a delay in the process of degeneration 21 and a slow return of the symptoms might be expected. Therefore, the increase in the number of laser applications could result in a lasting effect. Also, long-term follow-up studies might show if the other sites were more susceptible to the laser therapy.
A similar decrease in tongue pain was observed after irradiation of the stellate ganglion in patients with BMS. 13 In contrast to distant neural irradiation, in the present study, the light was applied on the affected site. Nevertheless, the increase in blood flow observed after the ganglion irradiation could also be achieved on the site of the laser application. 22 However, it is not known if this blood-flow alteration caused by the laser could be responsible for the maintenance of the effects for 6 weeks.
Comparing LLLT to other treatments reported, positive results were also obtained with systemic and topical drugs. However, side effects, especially in long-term use, 23 –25 represent a significant disadvantage for these pharmacological therapies.
This study is pioneering in reporting the effectiveness of LLLT in the reduction of BMS symptoms and the maintenance of the improvement achieved for 6 weeks in most of the affected sites. It is worth noting that the results obtained in this study were not based on a randomized controlled clinical trial, but the design was necessary for a study with such characteristics, particularly taking into account the positive results achieved.
Conclusion
Laser treatment was effective and well accepted by the patients, who did not report any adverse effects. The partial return of symptom intensity during the 6-week follow-up occurred on the tongue, and further studies are necessary to elucidate this issue. Meantime, LLLT may be a helpful approach in the treatment of patients with BMS.
Footnotes
Acknowledgments
We would like to thank FAPESP (Fundação de Amparo à Pesquisa do Estado de São Paulo – Proc. No. 06/55860-0) and CNPq-Brazil (Conselho Nacional de Pesquisa e Desenvolvimento) for their financial support.
Author Disclosure Statement
No competing financial interests exist.