
Abstract
Introduction
An alternative to traditional treatment modalities for diabetic ulcers is low-level laser therapy (LLLT). Among the various non-invasive treatments used in wound healing, LLLT has steadily increased in its applications to include a wide variety of medical and surgical specialties. 7 A number of published studies demonstrate the beneficial effects of LLLT, 8 although several other studies also exist which indicate results to the contrary. 9,10 Currently, there is no accepted theory to explain the mechanism of low-level laser biostimulation, and this lack of knowledge complicates the evaluation of conflicting reports in the literature. Lasers have been shown to be both stimulatory and inhibitory. These differences in the literature can be explained by the different treatment parameters used, such as wavelength, fluence, output power, and treatment regimens. 11 Patient status, as well as size and type of wound also play important roles. On the other hand, few articles provide all of the relevant laser parameters, making it difficult to reproduce the work.
In previous studies, 670 nm and 810 nm diode lasers have been individually studied. 12 –15 It has been shown that 810 nm diode laser prevents oxidative cellular damage and increases the reperfusion rate in ischemic conditions. On the other hand, this laser type is a genetically safe one, since it does not damage DNA, even in high fluences. 12,13 Previously, 670 nm diode laser has also been applied to treat the diabetic ulcer. It seems that this diode laser exerts its effects through genetic regulation of the cells to increase their proliferation and viability rate. 14,15
In the present study, we evaluated the effects of a combination of 670 nm and 810 nm diode lasers on diabetic wound healing parameters in rats.
Materials and Methods
Animals
Healthy adult male Swiss Albino rats (Wistar rats) [6-9 weeks of age, with average body weight of 245-300 g] were used in this study.
Blocked randomization of the samples
One hundred male Wistar rats were selected and divided randomly into four blocks of 25 rats. Five rats from each block (in total, 20 rats) were selected and placed together in a large cage. These rats were assigned randomly to four groups denoted as A, B, C, and D, and each rat was labeled with a code fixed to the tail.
Matching of the groups
After the rats were assigned to their groups, we measured their weight and frequently matched the groups based on the rats' mean weights. The age of all rats ranged from 4 to 6 weeks, and four groups were matched for their mean age. One rat among 20 was randomly excluded from the samples because of technical limitations of the study.
The sample included 19 animals divided into two groups: one diabetic (Group A) and the other (control) non-diabetic (Group B). In Group A, diabetes was induced. Then, each group was subdivided into two subgroups as follows:
Group A-laser: received laser as the intervention in the selected parameters (n = 5)
Group A-control: this group did not receive any intervention (n = 4)
Group B-laser: received laser as the intervention in the selected parameters (n = 5)
Group B-control: this group did not receive any intervention (n = 5)
Control groups did not undergo any therapeutic interference and were observed only. The study groups were of statistically equal body weights (P = 0.956; Kruskal-Wallis test).
Acclimatization
Each rat was placed separately in an experimental metabolic cage with the specified maintenance environment of a 12 hour day-night light cycle, a temperature of 25°C, and 65% humidity. Ten days of acclimatization were allowed so that the rats could habituate to the laboratory environment.
Induction of diabetes
Diabetes was induced in the animals of Group A by an intra-peritoneal injection of the pancreatic β-cell toxin streptozotocin (STZ; Sigma Chemical Co, St. Louis, Mo; freshly dissolved in sterile saline, 0.9%) at a dose of 65 mg/kg body weight. Using an Accu-Check Advantage Glucometer (Boehringer Mannheim Corp., Indianapolis, IN), blood glucose levels were monitored one week after the STZ treatment and throughout the duration of the study to determine the hyperglycemic state of the animals. Animals that failed to develop average blood glucose concentrations greater than 300 mg/dl within 9 days after the first injection were excluded from the study.
Developing the wounds on the rats
We made ulcers on the dorsal region of all animals according the following determined protocol.
Anesthetics preparation
A mixture of ketamine/ xylazine solutions with the ratio of 2/3 was utilized to anesthetize the rats. This anesthetic solution was administered intramuscularly to the great thigh muscle of the rats at the dose of 1 mg/kg body weight of the rats.
Preparation of the wound size ingot
A circle-shaped ingot with a diameter of 12 mm was prepared from a silastic plate in order to create wounds of almost equal area. Their circular shape also allows more convenient area measurement.
Preparation of the rats for wounding
Once anesthetized, we fixed the rats on a laboratory surgical board and shaved their whole dorsal region from their skull base to the proximity of the tail. We first cut long hairs and then the remaining short hair was shaved completely using a shaving blade after sterilization and wetting of the complete dorsal region with an alcoholic (ethanol 70%) solution. Afterwards, the wound region was determined, in the middle dorsum of each rat. An appropriate distance of the wounded area from the eyes of each rat was considered, for the least adverse effects of the laser irradiation on their eyes.
The prepared wound ingot was then placed on the determined region and the wound environment was lined by a methylene blue-saturated sterile swab stick.
Creating the ulcers
After preparation of the samples through the above-mentioned process, we cut the skin through the drawn line of the wound template using a 1.5 gauged surgical scalpel. Epidermis, dermis, and panniculus carnosus, up to the superficial layer of the deep fascia of the skin, was excised.
De-anesthetization
After completion of each session, we placed the rats in a warm environment, until they were withdrawn of the anesthetic effects. This prevented central hypothermia and any resulting cardiovascular effects stemming from the anesthetization.
Infection prevention
Intramuscular (IM) injection of gentamicin (5 mg/kg body weight of every rat) to their great thigh muscle administered prevented infection at the first session after surgical operation. In the subsequent sessions, IM gentamicin was repeated in the cases if purulent excretions were seen around the wound.
Therapeutic intervention
Once prepared, the rats in the laser groups underwent the therapeutic intervention. This included irradiation of the wounds with a combination of two low-level lasers according to the following laser protocol:
Laser dosage and protocol
Low level diode red-light laser (Gallium-Aluminum-Indium-Phosphate; GaAlInP laser) [Physiolaser Olympic, ©REIMERS & JANSSEN GmbH Medical Technology, Germany] with a wavelength of 670 nm using a contact hand-held probe (Handylaser Sprint-670) (power: 500 mW, energy: 10 J, time: 48 s) was irradiated to the wound bed area (energy density: 10 J/cm2).
Low level diode infra-red laser (Gallium-Aluminum-Arsenide; GaAlAs laser) [Physiolaser Olympic, ©REIMERS & JANSSEN GmbH Medical Technology, Germany] with a wavelength of 810 nm using a non-contact hand-held probe (Handylaser Sprint-810) (power: 250 mW, energy: 12 J, time: 50 s) was irradiated through a 2 cm distance to the wound. The probe contained a lens to diverge the laser beam to irradiate the wound margins (estimated energy density: 1.33 J/cm2).
There was a series of previously defined protocols regarding laser irradiation and frequencies on the laser device. The laser protocol used was a defined, fixed on-device protocol of ©REIMERS & JANSSEN GmbH Medical Technology Company for the treatment of acute wounds. This protocol included 5-second intervals of continuous Nogier A’ (292 Hz), Nogier B’ (584 Hz), and Nogier C’ (1168 Hz) frequencies, which were repeated during the treatment period for both laser types.
Therapeutic sessions
The low-level laser therapy sessions were performed every third day. In this method, a total of seven therapeutic sessions were done. These sessions were on the 3rd, 6th, 9th, 12th, 15th, 20th and 24th days after wound creation, which was defined as the day-zero study session.
Outcome measurements:
Wound healing promotion was evaluated through serial digital photography and wound area measurement in the successive sessions. Photography of the wounds was performed during each therapeutic session. In addition, we did a primary evaluation of the wounds the day after completion of the therapeutic intervention. In control rats, following the anesthesia, we performed the photography alone.
Photography of the wounds
Photography of the wounds was done using a high-quality digital microscope (AM313 Dino-Lite digital microscope; Dino-Lite, The Netherlands) connected to a laptop personal computer on which the required software for application of the microscope was installed. The digital microscope was fixed on a square metal-based stand holder (MS35B Digital Microscope holder, Dino-Lite, The Netherlands) and the magnification level was adjusted at each photography session to acquire the maximum size and sharpness of the captured wound area in the taken photographs. Also, a standard millimeter-graded metal ruler with a label including the rat code and session number was placed adjacent to the wound while taking the photographs, for the sake of calibration of the software in order to calculate the wound area.
Wound area measurement
Measurement of the wound area in the prepared photographs was accomplished using specialized graphical software (Adobe Photoshop CS4 extended, version 11.0 × 20071101 [20071101.m. 190 2007/11/01:02:00:00 cutoff; m branc] © 1990-2007 Adobe Systems Inc., U.S.A.) (Fig. 1). The entire process of area measurement was done by a single person who was blinded to the group of the rat and the session for each wound being measured. This avoided measurement biases by multiple measurers.

Distinct wound area was measured using powerful graphical software. (Color image can be found at
Finally, the outcomes were reported as successive measured wound areas, percentage of open wound area (%OWA), and wound healing rate for each evaluation session.
Percentage of open wound area for each session was calculated as the measured wound area in that session divided by the measured wound area on day 0, multiplied by 100.
Wound healing rate (RWH) was calculated as the difference in wound area from that of the immediately previous session, divided by the number of days between the two sessions.
Daily urine volume measurement
Urinary excretions for each animal were collected through the urine collecting system placed beneath the metabolic cages. This system allowed us to collect the urinary fluid into a sterile graded bottle. During a 24-h period, the urine bottles were emptied after registering the urine volume according to the grading of the bottles.
Euthanasia of the rats
Finally, after termination of the study period, the rats were killed with a 10 ml intra-peritoneal injection of Potassium Chloride (KCl) 20% solution after anesthetization.
Consideration of research ethics
Our study was accepted by the Laboratory Animal Committee of the Iran University of Medical Sciences (LACIUMS).
Data analysis
Repeated Measures Analysis using the Multivariate Analysis of Variance (MANOVA) with Bonferroni and Huynh-Feldt corrections for the degrees of freedom for the main therapeutic effect was used to analyze the repeated measurements in multiple groups. Tukey's honestly significant difference test and the Ryan, Eniot, Gabriel, and Welsch (R-E-G-W) F test were also applied as GLM Post-hoc comparison tests. In the case of skewed or abnormal distribution of the data, the non-parametric Kruskal-Wallis test was used to assess the difference in repeated measures between the study groups.
All analyses were performed using the Statistical Package for Social Studies (SPSS) version 17.0 (SPSS Statistics 17.0, Release 17.0.0); and the type one error level was assumed to be 0.05 for all analyses.
Results
We included 19 rats in four groups in the study. The mean weight for the samples was 272.37 g (95% confidence interval: 252.04–292.70 g).
On the third session of the study, the rat labeled as L2 died and was replaced immediately with a new one to prevent the study from more data loss. Another rat, labeled as LD1, died on the 9th day (session 4) of the study, and could not be replaced because of bias production. Therefore, the study continued with 18 rats altogether from day 10 of the study. The average area of the developed wounds in the first session (day 0) of the study was 414.69 mm2 (95% CI: 380.18–449.19 mm2); and there was no statistically significant difference between the mean wound areas of four groups in at this session (P = 0.545, One-way ANOVA).
Our results did not show any statistically significant differences in the wound area, percentage of open wound area, or wound healing rate changes throughout the repeated measurements in the study time period. Significant differences were found neither between the two diabetic (P = 0.334, P = 0.122, P = 0.480, respectively; [Fig. 2], nor the two non-diabetic groups (P = 0.302, P = 0.604, and P = 0.364, accordingly; (Fig. 3).

The difference between mean wound area

The difference between mean wound area
Although we could not complete the analysis of repeated urine volume measures because of excessive data loss (37 successive days of measurement), after 7 days of low level laser therapy, the urine excretion volume raised evidently in the laser-irradiated, non-diabetic rats in comparison with the non-irradiated control group, who did not receive the laser irradiation. However, we did not see a similar change in the urine excretion in their diabetic counterparts (Fig. 4).
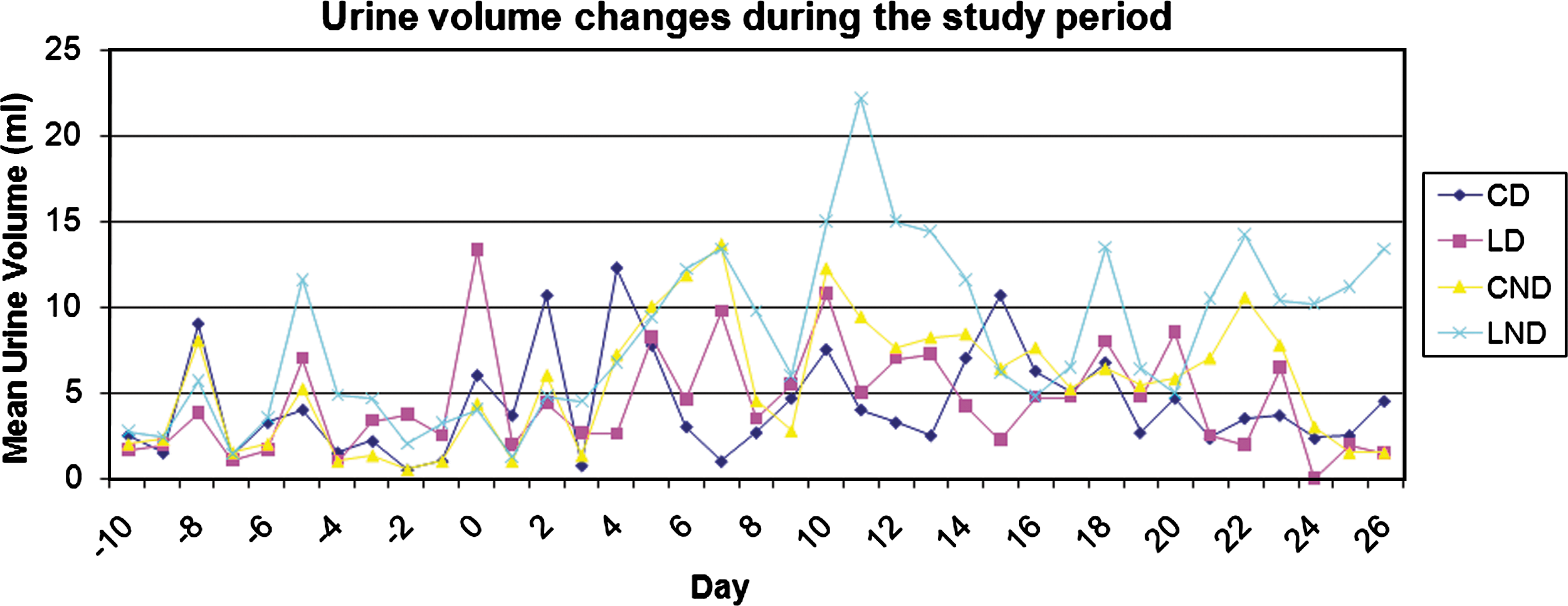
Urine volume changes during 37 days of the study period. Mean urine volume was significantly increased in the laser-treated non-diabetic group after 10 days (3 sessions) of laser therapy. (Color image can be found at
Discussion
Overall, according to our study, low-level laser therapy using a combination of 670 nm and 810 nm wavelengths did not improve the physical wound healing parameters examined, including wound area, percentage of open wound area, and wound healing rate.
There is a series of controversial studies about the efficacy of low level laser therapy in diabetic wound healing. Avni et al. 12 studied the effect of laser irradiation (GaAs, 810 nm) on ischemic reperfusion (I-R) injury in the gastrocnemius muscle of the rat brought about by complete occlusion of the blood supply for 3 h. The study found that the laser irradiation markedly protects skeletal muscles from degeneration following acute I-R injury. The study also found that the level of antioxidants was elevated following laser irradiation, which may reduce cytotoxic reactive oxygen species such as superoxide, which together with blood reperfusion aggravates the hypoxia during ischemic injury 12 . In another study, Kujawa and colleagues 13 found no considerable light-induced DNA damage after irradiating B14 cells with a wavelength of 810 nm at a fluence ranging from 3.75 to 15 J/cm2. Whelan and colleagues irradiated wounded mice with a light emitting diode laser with a 670 nm wavelength and 4 J/cm2 dose. They noticed that genes associated with cell death were down-regulated and proliferation and regulatory genes were up-regulated 14 . Schindl et al. also presented a case study of low-level radiation treatment of a diabetic ulcer. The ulcer had been present for 6 weeks and was accompanied by osteomyelitis. After 16 treatments over 4 weeks using a 670 nm diode laser, the ulcer was completely healed 15 . Kawalec et al. 16 , in a review of lasers in healing diabetic ulcers concluded that lasers appear to have a beneficial effect on enhancing wound healing in diabetic patients. They concluded that the 980 nm diode laser seems to have a considerable effect in healing diabetic ulcers, and noticed a number of effects resulting from photostimulation of the wounds. These effects included increased cell function/ activity through an increase in cellular respiratory mechanisms, ATP synthesis, DNA and RNA synthesis, cell proliferation, collagen synthesis, fibroblast proliferation, and stimulation of ascorbic acid utilization by the cells 16 . Although not statistically significant, in diabetic rats, the applied profile of low level laser therapy served to prevent normal wound healing, to some extent. In light of this finding, some of the inhibitory effects on wound healing parameters in the diabetic rats seen in our study could have resulted from excessive laser fluencies, especially those of the 670 nm diode laser applied in our profile. It seems that the application of two different low level lasers with an energy density of 10 J/cm2 in our profile may have exposed the diabetic wound cells to genetic damage and increased their apoptosis rate. This could have been confirmed through a histologic examination of the wounds following LLLT. However, because of insufficient sample size, we could not set up a design to histologically examine the treated wounds. Since the 810 nm diode laser has shown genetic safety in fluencies up to 15 J/cm2 in previous studies 13 , the 670 nm diode laser is implicated here as the source of such an effect. Al-watban 17 performed a recent study to determine the optimal laser dosimetric parameters in comparison with polychromatic light-emitting diodes (LEDs) that have been shown to speed up healing in four animal models. He used 532-, 633-, 810-, 980-, and ten 600-nm lasers (visible to far infrared) and polychromatic LED clusters (510–872 nm, visible to infrared) as photon sources. Finally, he recommended 633 nm laser therapies given three times per week at 4.71 J/cm2 per dose for diabetic burn healing, and three times per week at 2.35 J/cm2 per dose for diabetic wound healing, as actual doses for future human clinical trials 17 . Our results in a certain sense corroborate Al-watban's findings about the optimal protocol for laser intervention for diabetic wounds; our combination of irradiations did not improve physical wound healing parameters in diabetic or non-diabetic rats. Diabetic wounds and ulcers are observed with more frequency in patients with disease of long evolution and they are habitually chronic and complicated. Our study was done with a model of recently induced diabetes and acute, uncomplicated wounds.
We did not compare the measurements of diabetic and non-diabetic groups. Because the basic wound healing mechanisms could be very different in the two settings, such a comparison may convey a bias. However, using the control (non-diabetic) group helped us to see generally if low-level laser therapy changes physical parameters of wound healing in diabetic and non-diabetic groups with different patterns. In our study, laser irradiation failed to change the wound healing course in both diabetic and non-diabetic rats. This shows us that although the basic wound healing mechanisms are different in the two settings, our applied LLLT protocol did act similarly in the two groups; the cellular effects of LLLT obey similar rules in diabetic and non-diabetic conditions.
The slightly increased daily urine volume in the laser non-diabetic group in comparison with other groups was an incidental observation in our study. We could not find any previous report of this type of observation in the literature. However, this could have arisen as a result of systemic effects of our high-energy low-level laser in the non-diabetic rats. A variety of mechanisms, from central stimulation of the thirst sensation to an increase in renal function or triggering of renal wash-out mechanisms, could be responsible for the LLLT-induced urine volume increase in the non-diabetic rats. Further investigations are warranted to clarify the basic mechanisms underlying this observation.
Conclusion
Low level laser therapy with the applied combination of 670 nm and 810 nm diode lasers did not improve the wound healing parameters in a model of diabetic rats in this study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.