
Abstract
Introduction
Some studies have demonstrated that the increase in movement speed can be achieved by local injection of prostaglandins, 10 1.25 (OH)2.3 (active form of vitamin D), 11 or osteocalcin, 12 which is a protein exclusively produced by odontoclasts during the process of bone-matrix synthesis. 13 Although those cited injectable substances increase the speed of tooth movement, they also promote collateral effects in the patients, such as pain and discomfort. 13,14
Recently, Goulart 15 observed in dogs that high doses of LLL reduce the speed of tooth movement, whereas the opposite is observed with lower doses of LLL. Only two articles in the literature evaluated the influence of LLL on the speed of orthodontic tooth movement by means of clinical trials, 13,14 in which the results are divergent and the laser dosage different. With this background, there is still a necessity of more studies to verify the efficacy and to determine protocols of laser therapy used to increase the speed of orthodontic tooth movement. The purpose of this study was to compare the quantity of tooth movement of human canines, irradiated with diode laser or not, as well as to verify the tissue-integrity preservation after the use of laser for orthodontic movement.
Material and Methods
Ten patients of both genders (six female and four male patients), with a mean age of 13.1 years (range, 10.5–20.2 years) were selected for this study. The inclusion criteria were as follows: the need for extraction of first premolars due to biprotrusion or dental crowding; the presence of permanent dentition; the absence of any kind of systemic disease; no use any medication; and no previous orthodontic treatment. This protocol was approved by the local Research Ethics Committee at the São Paulo Methodist University, SBC, Brazil.
Twenty-six mandibular or maxillary canines or both were evaluated, 13 laser irradiated and 13 nonirradiated (placebo). Five maxillary and eight mandibular arches were evaluated. In three patients, both arches were included in the research. Only one side of the arch was laser irradiated, representing the Laser Group (LG), whereas the other side was not irradiated and then was considered the Control Group (CG). The initial retraction of the canines started after a period of 3 months of the premolar extractions, and it was further evaluated for a period of 4 months.
Metallic brackets, Andrews prescription, 0.022 × 0.028-inch slot (Ormco Corp., Orange, CA), were placed on canines and second premolars, whereas the first molars were properly banded. Bilaterally segmented arches made of stainless steel, 0.016, were adapted in conjunction with a closed Ni-Ti coil spring (12 mm in length; Morelli Ltda., Sorocaba, Brazil), delivering a force of 150 g/side for the initial retraction of the canines. This force was measured with a dynamometer (commercial brand, Morelli). The springs were reactivated (150 g/side) after 30 (T2) and 60 days (T3). The impressions were performed at initial (T1), after 30 (T2), 60 (T3), and 90 days (T4). Besides those steps, periapical radiographs of the canines and first molars were taken at the T1 and T4 phases, by using the bisecting-angle technique.
The equipment was Twin Laser (MMOptics Ltda, São Carlos, São Paulo, Brazil), which is a semiconductor diode low-level aluminum-gallium-arsenide (AsGaAl) laser. It presents wavelengths at the infrared spectrum (λ = 780 nm) and emits continuous waves with an irradiated area of about 0.04 cm2.
The laser application was performed by one operator (M.V.S.S.), at the predetermined point areas in only one of the canines randomly chosen. The used output was 20 mW, with an energy density of 5 J/cm2, and it was used for 10 sec per point, resulting in 0.2 J of energy per point. As 10 points per tooth (five bucally and five lingually) 14 received irradiation, the total energy (TE) surrounding canine roots was 2 J per treatment time. The laser application was performed after the closed NiTi coil spring was installed or activated (day 0), 3 and 7 days after the first application, resulting in 6 J/month of energy. The application protocol was as follows: point area application, light beam perpendicular to and in direct contact with the mucosa, clean and dry surface, and application under cotton-roll isolation. The point areas for application are illustrated on Fig. 1.
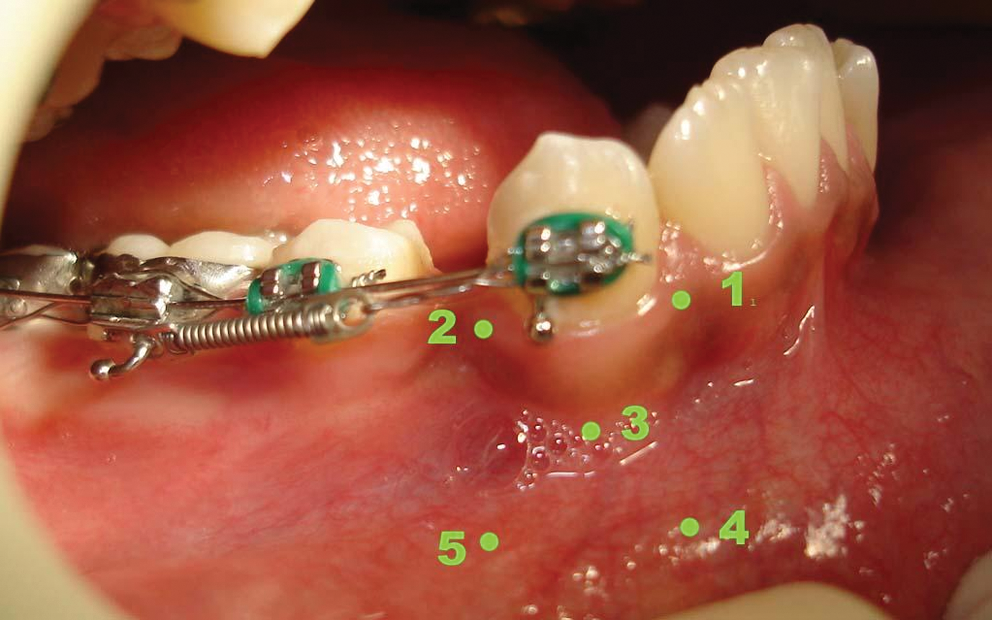
Points for laser application at the buccal surface: (1) mesiobuccal gingival ridge; (2) distal buccal gingival ridge; (3) buccal central point, central in relation to the other points; (4) bottom of oral vestibule, at the same vertical direction as point 1, and at the level of the root apex; and (5) bottom of oral vestibule, in the same vertical direction as point 2, and at the level of the root apex. The same points were selected for lingual application, totaling 10 points.
The laser irradiation was performed right after the spring activation (T1) and reactivations (T2 and T3), totaling nine applications.
Measurement of casts and radiographs
The casts obtained in the four different evaluation phases (T1, T2, T3, and T4) were 3D scanned with 3 Shape, model D-250 (3Shape's D-250; Denmark). The measurements were performed with the Geomagic Studio 5 software (Raindrop Geomagic, Inc.). For the measurements, the tips of canines of both sides, as well as the most cervical area of the papilla between the central incisors in both maxillary and mandibular arches, were references to determine the linear distance between the papilla and the canines, irradiated (PiCD) or not (PCD). Canine retraction was measured monthly by the difference of PiCD or PCD obtained the previous month (T2−T1, T3−T2, T4−T3) (Fig. 2).
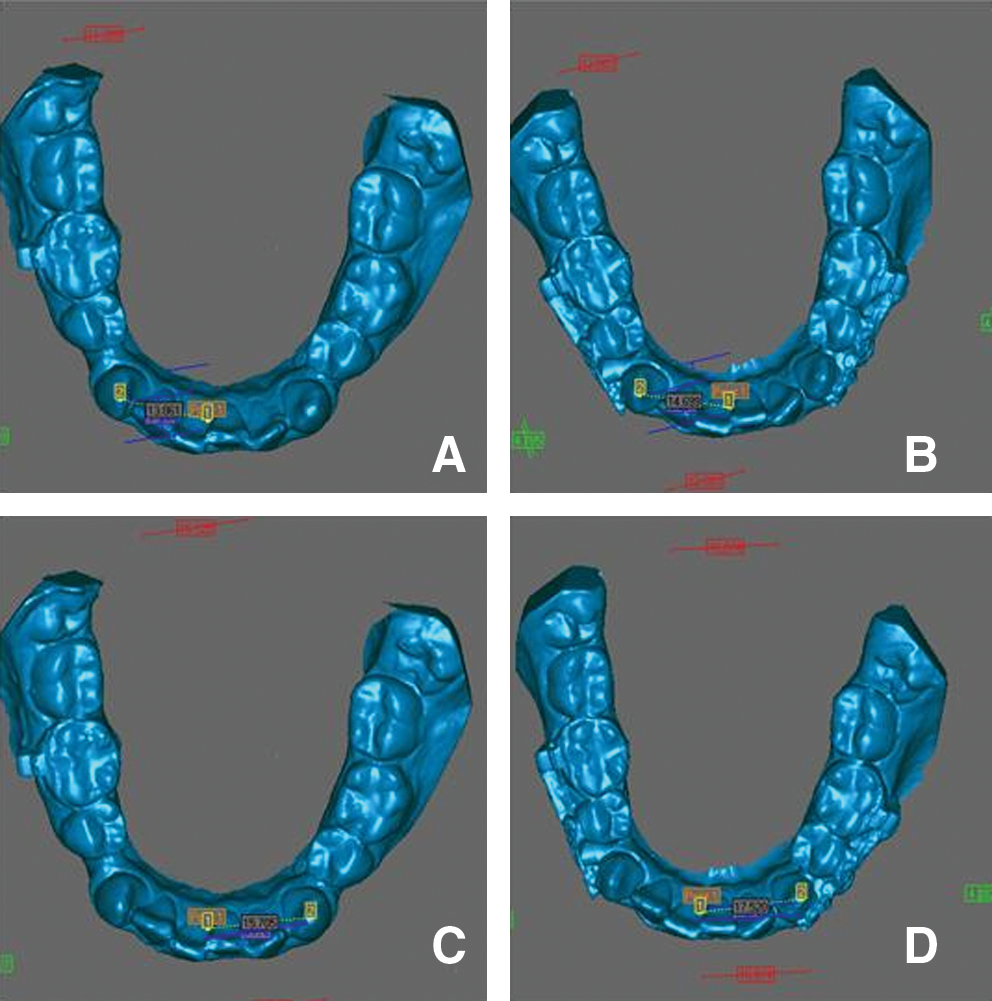
3D image of inferior casts with the reference points and the performed measurements in the same patient. (
The distance between the alveolar bone ridge (AR) and the cemento-enamel junction (CEJ), obtained parallel to the tooth long axis and on both distal and mesial aspects of the canines, irradiated or not, and first permanent molars, was measured on the initial and final (T1 and T4) periapical radiographs. 16 The obtained difference (T4−T1) was converted to scores, as showed in Fig. 3. These scores were obtained to evaluate the quantity of bone resorption of the alveolar ridge. Any possible root resorptions of the retracted canines were also evaluated by using the previously mentioned radiographs and following the root-resorption levels proposed by Levander and Malmgreen. 17 For both evaluations (bone ridge and root resorption), the alterations of irradiated and nonirradiated canines were compared.

Measurement of alveolar bone ridge, AR-CEJ distance. The scores were obtained from the difference between the initial and final (T4−T1) measurements of the AR-CEJ distance. Score 1, >0 and ≤1 mm; Score 2, >1 and ≤2 mm; and Score 3, >2 mm. Scores 1 and 2 were classified as healthy periodontal status, but score 3 as having periodontal damage.
27,28
(
Method error
To control the errors, the measurements of casts and radiographs were repeated in five randomly selected patients, after a period of at least 15 days.
Statistical analysis
To measure the error, we used the paired t test and the Dahlberg 18 formula for the cast measurements. The method error for the radiographs was evaluated by means of a kappa test. 19
Analysis of variance followed by Tukey multiple comparison tests was used to compare the movement of laser-irradiated canines with nonirradiated ones. The Wilcoxon test was used for the comparison of root resorption and alveolar bone ridge resorption between the laser-irradiated and non–laser-irradiated sides.
For all tests, the significance level was 5% (p < 0.05). The software Statistica for Windows, volume 5.1 (StatSoft Inc.) was used.
Results
No statistically significant systematic error was found in all evaluated casts. The casual error for the cast measurements was considered clinically not relevant (Dalhberg error = 0.01). On the radiographs, the error was also considered not relevant, with kappa values greater than 0.7 and concordance greater than 90%.
The analysis of variance results showed no statistically significant difference between the movement of either maxillary or mandibular canines (Table 1), allowing pooling the maxillary and mandibular teeth for the multiple comparison by using the Tukey test (Table 2). The movement of laser-irradiated canines was statistically greater than that in the nonirradiated group, in all evaluated periods (Table 2).
Statistically significant (p < 0.05).
Statistically significant for p < 0.05.
No statistically significant difference was found in the resorption of either root or alveolar bone ridge, between the laser-irradiated and nonirradiated groups (Table 3). Regarding the first molars, no statistical difference in the resorption of the alveolar bone ridge was noted (Table 4).
No values were statistically significant.
No values were statistically significant.
Discussion
Study design
Few laboratory studies have evaluated the influence of laser on orthodontic movement in animals, but all of them proved that bone tissue that underwent LLL therapy showed an accelerated repair process, increasing bone neoformation and consequently increasing the speed of orthodontic tooth movement. 4,15 Only one clinical study was done in humans, 14 in which it was stated that the LLL therapy (λ = 780 nm/5 J/cm2/10 sec, 0.2 J by point, totaling 8 J/month) statistically increased the speed of orthodontic movement. In this present study, the obtained results were similar, but a lower dose of laser was used, totaling 6 J per month per tooth. Practically, this information is relevant once laser-therapy appointments can be reduced, resulting in less chair time and fewer returns needed, and also to determine the really necessary laser dose to obtain faster orthodontic movement.
In the present study, canine retraction was evaluated in segmented arches, different from that in Cruz et al., 14 avoiding interference of the contralateral side. The measurements were performed monthly by using digitized casts; measurement performed directly in the mouth (in loco) cannot be reproduced (no method error), 14 and its accuracy is low.
In our study, the laser was applied by a single operator (MVSS), and patients did not know which side was irradiated, resulting in a prospective and blind study. Patients were their own controls, reducing the variability and allowing a smaller number of patients in the sample. 13,14 As no difference in tooth movement was observed between the maxillary and mandibular arches through the analysis of variance (Table 1), both arches from some patients were included in the analysis, totaling 26 teeth, 13 laser irradiated and 13 not irradiated, similar to the studies of Cruz et al. 14 (22 teeth) and Limpanichkul 13 (24 teeth).
Three-dimensional casts were used to analyze tooth movement, as this technique allows a better visualization and consequently greater precision to determine the target point in a tridimensional sense. 20,21 This precision was confirmed, as no statistically significant error of the method was observed, showing the reproducibility of the measurements.
Possible alveolar bone-ridge resorption, at the mesial and distal aspects of retracted canines and first molars, and possible root resorption of the retracted canines, were evaluated through periapical radiographs obtained at the beginning (T1) and at the end of the study (T4, 90 days). As both the patient and the evaluator (at the time of the evaluation) were not informed which tooth was irradiated, this study is characterized as double-blinded. The radiograph analyses were essential to determine possible injuries to periodontal tissues or root resorptions as a result of retraction forces and laser application.
Effects of laser application on orthodontic movement
In this study, a statistically significant greater orthodontic movement was observed in the group irradiated with laser, in comparison with the nonirradiated one (Table 2). These results are not in agreement with the results obtained by Limpanichkul et al., 13 in which no effect of LLL on orthodontic movement was reported. That study used higher doses of laser (25 J/cm2/2.3 J per point/18.4 J per tooth); and this dose might have no effect on the speed of tooth movement. According to Goulart et al., 15 higher doses of LLL could present inhibitory effects on tooth movement.
In this study, which used the same protocol as described by Cruz et al. 14 (5 J/cm2/0.2 J per point/2.0 J per tooth/8 J monthly), where an increase in speed of tooth movement in the irradiated group was observed, the results were similar; although the total acccumulated energy was lower, 6 J per month (one application was skipped). With this information, in future studies, the use of one or two monthly LLL applications might be enough to achieve the same results as this study, regarding orthodontic movement.
The exact mechanism of biostimulation promoted by LLL is still unknown, but according to some reports, 4,6,9 the LLL promotes the appearance of singlet oxygen, which increases the formation of adenosine triphosphate (ATP) in the irradiated spot, 9 and cell metabolism is accelerated. Moreover, more Ca2+ ions will be found in the cytoplasm, due to LLL action (with wavelength at the infrared level) on the sodium-potassium pump of the cell membrane. This promotes greater protein synthesis 9 and accelerates DNA duplication and RNA replication, 22 accelerating cell metabolism.
When evaluating the total difference of canine movement between the initial and the final phases (T4−T1; Table 2), we can observe that the irradiated side had almost double the movement of the nonirradiated side. However, when evaluating the difference between the following recall periods, T2−T1, T3−T2, and T4−T3 (Table 2), it can be observed that as time goes by, this difference decreases, although still being statistically greater for the irradiated canines in relation to the nonirradiated ones. This probably occurred because of a systemic effect of the laser. The laser irradiation would promote an increase in phagocytosis of leukocytes present at the irradiated area, being transferred to other nonirradiated areas by humoral substances. 6
Clinical considerations
The use of LLL to accelerate tooth movement presents advantages in relation to other resources like injectable drugs 10 –12,23 and electrical stimulation, 24 as these other resources may promote painful sensitivity for the patients. Among the advantages of LLL, the simple application method is painless and does not have collateral effects, 13,14 besides having very few contraindications.
For clinical implications, faster tooth movement can significantly reduce treatment time, an advantage especially for adults; longer treatment times can imply greater chances of alveolar bone loss and caries recurrence. 25,26 A decrease of sensitivity due to orthodontic movement can also be obtained with LLL 1,2 ; however, this is true with higher doses than those used in this study. The ideal for future studies should be to find a specific dose of LLL that could promote faster orthodontic movement, as well as reduce sensitivity.
LLL might also work to stimulate and facilitate tooth movement in difficult clinical situations, as with nonerupted teeth that will undergo orthodontic traction or in molar distalization or anterior teeth retraction mechanisms. Laser application with stimulation levels, especially on those teeth previously mentioned, would probably facilitate tooth movement and consequently would reduce the treatment time.
Conclusions
Low-level laser therapy statistically speeded the orthodontic movement of canines during the initial retraction period. No alveolar bone ridge resorption of the support teeth or canine root resorption was observed.
The LLL therapy represents an excellent adjuvant therapeutic resource for orthodontic treatment; it can probably reduce the treatment time. However, more studies in this area are necessary.
Footnotes
Acknowledgments
This report was based on research by Dr. Marinês Vieira da Silva Sousa in partial fulfillment of the requirements for the Master's degree in Orthodontics at São Paulo Methodist University, São Bernardo do Campo, São Paulo, Brazil.
Author Disclosure Statement
No competing financial interests exist.