
Abstract
Introduction
Patients and Methods
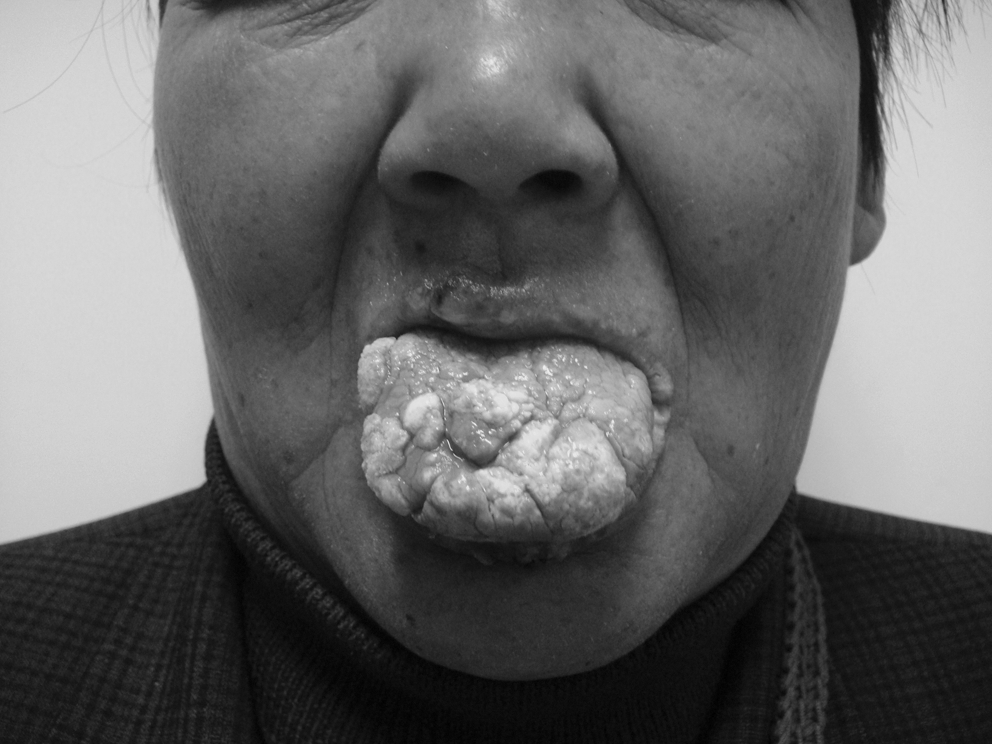
A 59-year-old woman was admitted to our hospital with widespread asymptomatic papillomatous lesions in the oral cavity (Fig. 1). It was very hard for her to swallow, eat, or speak. The lesions appeared 7 years ago on the buccal mucosa and the lower lip, and gradually increased in numbers and expanded to the gingivae and the tongue. She had been treated with interferon, excision, and electrocauterization during last 4 years. Yet again, new papillomatous lesions recurred on the affected area several weeks after each treatment. For suggestive verrucous carcinoma, she had accepted superior gingivectomy and alveolectomy. However, the lesions relapsed 2 months later and progressed as before. She was diagnosed with OFP with lesion biopsy.

Numerous papillomatous lesions on the mucosal surface of the lip, tongue, and gingivae.
The study was approved by the hospital ethics committee and given a fully informed consent by the patient. She had no serious systemic diseases and had not taken an oral retinoid within the past 6 months. A gastric tube was fixed before treatment.
The patient was first subjected to a skin allergy test. After a negative result, she was intravenously injected with 5 mg/kg PsD-007(provided by the Shanghai Institute of Red-Green Photosensitizers, Shanghai, China) in a shaded room. Three hours later, each lesion area was exposed for 10 min to a continuous laser beam of 635 nm wavelength radiated by a diode laser type XD-635AB (manufactured by Xingda Photoelectricity Medical Equipment Corporation, Guilin, China) with laser intensity of 177 mW/cm2 and energy density of 106.2 J/cm2. The fluorescence was visualized by exposure to 532-nm light. The light direction was adjusted to keep a constant distance from lesions and a 3 cm2 light spot on each lesion. She was prescribed 30 mg/d of the antiinflammatory drug prednisone acetate for 3 days after light illumination. She was told to stay strictly in the dark for 1–2 weeks and then gradually to return outdoor activities 2 weeks later with dark glasses for at least a month. She returned 1 month after the treatment for clinical evaluation. Later, she experienced another two periods of treatment every another month. No dyspnea was found during the therapy.
Results
The patient was able to eat and drink normally 3 days after the first treatment. After two courses, the lesion volumes markedly decreased (Fig. 2). The small lesions completely disappeared, and the diameters of the larger papillomatoses were reduced by ≥80%. She was satisfied and did not come back for further treatment. After each treatment, evident edema occurred on the face, with discharge of yellowish serum-like liquid in the mouth. It generally needed 2–3 days to subside. Distending pain was obvious after each treatment, but always faded within 2 days. The pain lessened, and the duration shortened with more treatments. No other side effects were found.
Patient received two courses of treatment at a drug dose of 5 mg/kg and a light dose of 106.2 J/cm2. Clinical appearance of the tongue and lip 1 month after the second session. The small lesions completely disappeared, and the diameters of the larger papillomatoses were reduced remarkably.
Discussion
OFP is a rare disease characterized by multiple papillomatous lesions in the oral cavity. Infection with human papillomavirus (HPV) subtypes 13, 32, 6, 16, or 11 could be the cause of the disease. 7–8 The therapeutic effects of ALA-mediated PDT were evaluated in HPV-related diseases such as cervical intraepithelial neoplasia 9 and condyloma acuminatum. 10 In this case, we chose systemic application of a photosensitizer but not topical administration of ALA into OFP lesions, because the widespread, irregular, and large lesions suffusing the mouth cavity were difficult to cover with ALA gel, whereas systemic administration was able to distribute PsD-007 into each lesion. In tumor cells, accumulation of protoporphyrin IX(PpIX) could result from decreased conversion of PpIX to heme because of decreased ferrochelatase activity 11 after a period of metabolism.
To eliminate side effects, we chose 3 h as application time, because the PsD-007 has pharmacokinetic parameters of t1/2π = 0.26 ± 0.5 h and t1/2α = 4.52 ± 1.04 h. 6 After 3 h, only a limited amount of photosensitizer is left in the normal epidermis and other tissues. When PpIX is illuminated with light of an appropriate wavelength, the excited molecule then emits energy to produce singlet oxygen, a highly reactive and cytotoxic species, resulting in cell death. The combination of photosensitizer distributed in malignant tissues and selected light delivery provides an effective therapy with efficient cytotoxicity to the tumor and limited damage to the surrounding normal tissue. 12 Therefore, the patient recovered rapidly and could swallow normally after PDT.
The depth of tissue necrosis induced by ALA-PDT ranges from 0.1 to 1.3 mm in oral lesions, and complete epithelial necrosis is present in all cases. 13 Because the depth of tissue necrosis induced by PDT depends on the wavelength of the light source, we speculate that the depth induced by administration of PsD-007 is similar to that by ALA-mediated PDT. Other studies have shown that the targeted tumors ≤2 mm in thickness are completely ablated 14 with systemic PDT.
After three courses, the lesions regressed rather than healed. Because thicker keratin layers can reduce light intensity and prevent sufficient light from reaching the underlying lesions, insufficient light dosage causes only partial photochemical reactions and limited tissue necrosis. Therefore, we observed the complete disappearance of small lesions and only reduced volumes of larger lesions. Using a more powerful light source may result in a better outcome.
The prolonged photosensitivity definitely limits the wide application of the new treatment modality in the clinic. Although more remarkable remission of papillomatosis could be obtained, the patient would not receive further treatment because of the required 2 weeks of complete darkness protection after PDT. The combination of systemic PDT and topical PDT may increase treatment compliance. Hence, a more powerful laser system and a new photosensitizer with shorter period of light avoidance are urgent to reduce the distress of patients.
Conclusions
In summary, this study provided a new method of systemic PDT for OFP treatment and achieved relatively good short-term clinical efficacy. Although the long-term outcome must be further studied, we believe that systemic PDT should be an effective and satisfactory treatment in refractory epidermis tumors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.