
Abstract
Introduction
Surgical excision is often the first option for treating PCACC. 3 –5 However, the tumor tends to have a high potential for recurrence after local excision. 1,4 –7 It has been reported that the recurrence rate can reach 50% or even 70%. 6,7 Although surgical treatment with extensive resection margins is recommended, it is not appropriate for patients with facial lesions.
Case Report
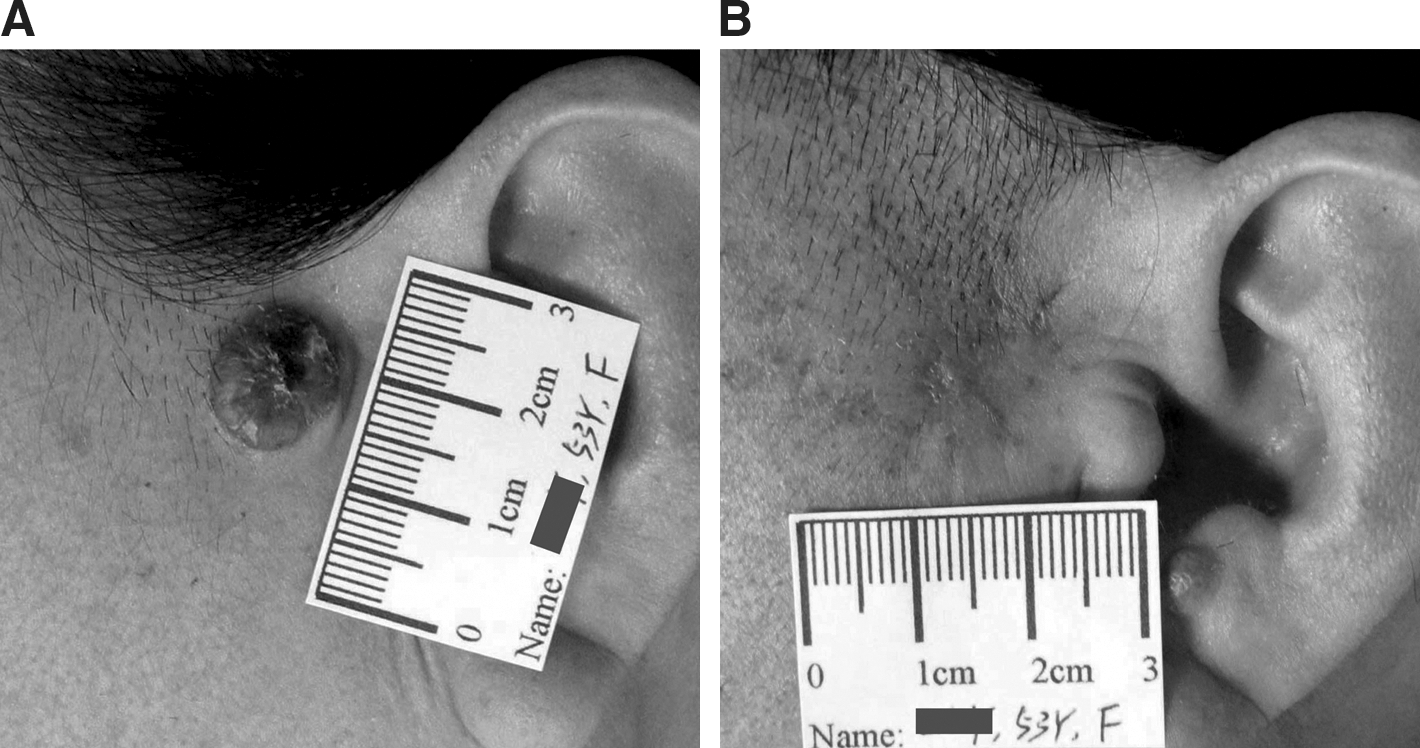
A 53-year-old Chinese woman presented to our clinic with symptoms of PCACC in the preauricular region. She complained of a small, brown, pinkish papule appearing about 3 years ago, which had gradually increased in size over time. Occasionally she experienced slight pain around the papule, but neither surgical procedures, including laser surgery, nor pharmacological therapies had been attempted. A physical examination conducted at our center revealed a single, soft papulonodular eruption with the scales affecting her left cheek (Fig. 1A). The tumor was round, with a diameter of 1.3 cm. No other similar lesions were found on her body. The salivary glands, bronchi, and other organs were also examined, and no signs of neoplasm were found. In addition, superficial lymphadenopathy did not exist. It was decided to resect the tumor surgically, with the scope of the removal including the whole lesion and the surrounding skin tissue with a margin of 0.5 cm beyond the borderline.
Furthermore, the metastasis to intracranial tissue and the lungs was first excluded by computer tomography examination (CT scan), and the sera carcinoembryonic antigen (CEA) was determined normal by laboratory tests. However, the lesion specimen showed large cell masses with a tubular or cribriform pattern histopathologically (Fig. 2A), plus many small solid epithelial islands were shown without overlying epidermal connections (Fig. 2B). All the analyses matched previously reported PCACC, 8 including three types of cystic spaces, the pseudocysts with abundant basophilic mucin (Fig. 2C), true glandular lumens, and intercellular spaces. In addition, there was no significant perineural invasion in this specimen. Immunohistochemical analysis also indicated positive results for epithelial membrane antigen (EMA), α-smooth muscule actin (SMA), cytokeratin AE1/AE3, and S-100 stainings, though it was almost negative with CEA. There was no apparent tumor mass found in the immediate proximity to the operation ridges.

One week after the surgery, the wounds had healed completely. With informed consent, the patient began a series of the treatments of 5-aminolevulinic acid (ALA)-based photodynamic therapy (PDT). 9 A total of 20% ALA (Shanghai Fudan-Zhangjiang Bio-Pharmaceutical Co., China) cream was applied in each treatment to the lesion location, with a margin of about 2.0 cm beyond the visible excision border. The whole lesion area was then covered with black gauze, which protected it from the light for 3 h before the laser irradiation. A non-heating He–Ne laser with a specific wavelength of 632.8 nm (Guilin Xingda Co., China) was used for the therapy. Thirty minutes of irradiation with the fluence of 80 J/cm2 for each PDT was applied to the ALA-treated area. This treatment was given once a week and repeated five times. A control histopathological examination performed 1 wk after the final PDT treatment revealed that no tumor cells were shown in the specimen.
The patient was then followed up for 40 mo after the therapy. During this period, no evidence of recurrence or metastasis was found. The eruption had disappeared, with a slight hyperpigmentation at month 10 (Fig. 1B). Workup for recurrence or metastasis, including a chest X-ray, head and neck CT scan, and ultrasonic screening, all showed normal skin structures and visceral nodules in the previous lesion area. By the end of the follow-up period, the local hyperpigmentation had disappeared completely. Only the inconspicuous post-operative scar remained.
Discussion
Compared to an adenoid cystic pattern of basal cell carcinoma, in which focal neoplastic aggregations are usually found, PCACC shows the entire neoplasm to be composed nearly of cribriforms, with the pattern relatively uniform in size and shape. 10 To make a definite diagnosis, immunohistochemical analysis was needed to obtain supportive results. Besides adenoid basal cell carcinoma, PCACC requires other differential diagnosis, including cylindroma, mucinous apocrine carcinoma, and apocrine mixed tumor in the skin. 1,2
Frequent local recurrence after surgical excision is an important feature of PCACC. 1,2,6,7 The interval between surgery and recurrence can range from 4 mo to 20 yr, 7 and recurrence has been found in 37% of reported PCACC patients during the first 3 yr of follow-up. 2 Perineural invasion might be associated with an increased rate of recurrence, but this is not absolutely certain. 2 Adenoid cystic carcinomas can be classified into three different histological variants: tubular, solid, and cribriform, with the solid variant having a worse prognosis than the other two variants. 2
PDT combines the selective accumulation of a photosensitizer in tumor tissue with visible light to produce reactive oxygen species. 11 It results in selected cellular phototoxicity and the ablation of the tumor lesion, and also keeps the surrounding normal tissue undamaged. It has been proven that PDT could reduce the number of new lesions developing in patients at high risk of skin cancer, and it has a role as a preventive therapy. 12 ALA could be absorbed by the residual malignant cells, which might be the cause of recurrence. Giving this fact, ALA has been widely chosen as a photosensitizer in some anti-tumor PDT treatments, as it can be absorbed by the recurrent prophylaxis of superficial tumors.
Although dozens of PCACC cases have been reported before, our patient was the first case found in China, and she was also the first PCACC patient treated with PDT. In our case, the tumor did not show prominent perineural invasion but clear histological typing for the mixture of tubular, solid, or cribriform stuctures. The lesion was located in the facial region, which restricted more aggressive therapy after the original excision. Because the visible lesion had been removed, ALA-PDT was chosen as the consolidation treatment because it is widely used to treat superficial non-melanoma skin cancers. 13
The patient seemed to have superior cosmetic outcomes compared with the use of simple excision, which might imply that PDT therapy actually inhibits collagen secretion of fibroblasts. 14,15 The follow-up may still not be enough to conclude the final effect of ALA-PDT on PCACC, although a second histological check revealed no malignant cells in the original location after PDT, and a thorough examination found no evidence of any relapse. ALA-PDT can be a safe and effective alternative therapy that can reduce recurrence and obtain good cosmetic results.
Footnotes
Author Disclosure Statement
No competing financial interests exist.