
Abstract
Introduction
Failure to heal generally arises during the initial stages of tissue repair when a marked reduction occurs in angiogenesis, collagen synthesis, and in the migration and activation of leukocytes, macrophages, and fibroblasts, and there is an increased risk of infection. 6 –8 There is evidence that various therapeutic strategies are capable of modulating the events involved in all the phases of the healing process of skin wounds. Low-level laser therapy (LLLT) has been widely used in biomedicine for the treatment of wounds resulting from trauma or vascular injuries in view of its positive photobiomodulation effect on tissue repair. 4,9 –11
Although LLLT has been widely investigated over the past 30 yr, parameters such as the type of laser, the number of applications, the time of application, the duration of treatment, and the type and source of light emission remain the focus of investigation in a search for more effective methodologies for the management of different clinical and experimental situations. 4,11 A important point of controversy concerns the wavelength and the appropriate energy density for the treatment of skin lesions. Previous studies have shown that the gallium-aluminum-arsenide diode laser (GaAsA1 λ 830 nm), when used with energy densities between 1 J/cm2 and 20 J/cm2, is capable of stimulating the healing of skin lesions in humans and laboratory animals. 9,12,13 Nevertheless, with respect to this type of laser, data on the effect of energy densities greater than 20 J/cm2 on the healing response, as well as the dose–response effect of this stimulation, are sparse and conflicting. These limitations hamper the reproduction and use of protocols that have been described in specific clinical and experimental situations.
In addition to LLLT, healing oils containing a combination of medium chain triglycerides and essential fatty acids have been frequently used to stimulate cell nutrition, tissue regeneration, and the healing speed of wounds. 5,14 –16 Although this therapy is common in clinical practice, to the best of our knowledge no studies have been carried out to compare these substances with LLLT. Therefore, it is important to investigate the effect of higher energy densities on aspects related to the healing process of wounds. In addition, comparing the effects of LLLT with the effect on wounds of oils containing a combination of medium chain triglycerides and essential fatty acids may contribute toward the development of broader and more effective therapeutic strategies for the treatment of skin ailments. Thus the objective of the present study was to compare the effect of GaAsA1 laser (λ 830 nm) at the densities of 30 J/cm2 and 60 J/cm2, and healing oil, on the quantity of fibroblasts, blood vessels, and collagen maturation in skin wounds in Wistar rats.
Materials and Methods
Twenty-four male Wistar rats (Rattus norvegicus), 10 wk old and weighing 325 ± 27 g, obtained from the central animal laboratory of the Biological Sciences Center, Federal University of Viçosa, Minas Gerais, Brazil, were used in the present study. During the experiment, the animals were maintained in a controlled environment (temperature 22°C; 12 h light/dark cycles) in individual cages that were cleaned daily. Water and standard rat chow were provided ad libitum. The experiment was approved by the Internal Review Board of the Institute for the Care and Use of Laboratory Animals (protocol 005/2008). Before the surgical wounds were made, the animals were first anesthetized using an intraperitoneal application of ketamine (60 mg/kg bw) and xylazine (10 mg/kg bw). Next, a trichotomy was performed on the dorsolateral region of all the animals, and the area was thoroughly defatted using ethyl ether (Merck®, Rio de Janeiro, Brazil) followed by the use of 10% povidone-iodine for antisepsis (Johnson Diversey®, Rio de Janeiro, Brazil). Five circular secondary intention wounds 12 mm in diameter were made in the dorsolateral region of the animals by performing a surgical incision in the skin and subcutaneous cell tissue using a scalpel. The area of the wounds was previously marked using crystal violet and checked using an analogical pachymeter (Mitutoyo Sul Americana Ltda®, São Paulo, Brazil). The depth of the surgical incision was controlled by removing the epithelial tissue until the dorsal muscular fascia was exposed. 17 After the wounds had been made, the animals were randomly divided into four groups of six animals each: the Control Group in which wounds were cleaned using a 0.9% saline solution; the L30 Group in which wounds were treated using the GaAsAl laser (λ 830nm, 30 J/cm2); the L60 Group in which wounds were treated with the GaAsAl laser (λ 830nm, 60 J/cm2); and the Oil Group in which wounds were treated with 0.1 g of oil consisting of medium chain triglycerides (caprylic acid, capric acid, caproic acid, and lauric acid) and essential fatty acid (linoleic acid) in a proportion of 1:1 (Saniplan Essential Products®, Rio de Janeiro, Brazil). A GaAsA1 diode laser with a wavelength of 830 nm, an output of 9 mW, collimated beam, and a punctual area of irradiation of 0.035 mm2 (Quasar®, Dentoflex, São Paulo, Brazil) was used in this study, having been previously calibrated by the manufacturer. Radiation was performed using a probe from the device, guided in a scan technique perpendicular to the surface of the wounds. The time of application was automatically adjusted by the device in accordance with the energy dose selected. The wounds were cleaned daily with 0.9% saline solution immediately prior to application of the laser treatment or healing oil. All therapies were initiated 6 h after surgery and repeated daily for the 20 d of the experiment. For the histological analysis, fragments of tissue were collected from the different wounds every 4 d. Each fragment contained tissue removed from the center of the wound, as well as part of the uninjured tissue removed from a region adjacent to the border of the wound that had not received radiation from the laser. The fragments of tissue from the wounds were fixed in a solution of 10% formaldehyde in 0.1M sodium phosphate buffer, pH 7.2, dehydrated in ethanol, cleared in xylol, and embedded in paraffin. Next, 4-μm thick histological sections were cut in a Leica Multicut 2045® rotary microtome (Reichert-Jung Products, Germany). The sections were mounted on histology slides and stained with hematoxylin-eosin for the analysis of fibroblasts and blood vessels 17,18 or stained using the modified Sirius red technique for the analysis of collagen maturation. 19,20 To avoid repeat analysis of cells, sections were evaluated in semi-series, using 1 in every 10 sections. The slides were visualized and the images captured using a BX-60® light microscope (Olympus, Tóquio, Japan) connected to a QColor-3® digital camera (Olympus). Four slides were made for each wound, each slide containing six histological sections. For each section, 15 images were randomly captured using a resolution of 2048 × 1536 pixels with an objective of 20 × . Using the digitalized images, fibroblasts and blood vessels were counted using a grid of 216 intersections associated with the image analysis software program Image Pro-Plus 4.5® (Media Cybernetcs, Silver Spring, MD). The collagen maturation index (CMI) was calculated using the ratio % of type I collagen:% of type III collagen, with indexes close to or over 1 (CMI ≥1) indicating a higher proportion of type I collagen and a greater level of maturation of the collagen fibers. 17 Differentiation of type I and type III collagen fibers was made using the Quantum® software program (Department of Soil Science, Federal University of Viçosa, Viçosa, Brazil). Statistical analysis was performed using the SPSS statistical software program (V11.0; SPSS Inc., Chicago, IL). Data were presented as measures of central tendency, means, and standard deviations (SD). Normal distribution of data was verified using the Kolmogorov–Smirnov test. Based on this test, intergroup comparison of the mean values of collagen fibers, number of fibroblasts, and blood vessels was performed using the Kruskal–Wallis test. A significance level of 5% was defined throughout the statistical analysis.
Results
Observation of the skin wounds over the 20 d of the experiment showed the characteristic signs of a normal, infection-free healing process. Statistical analysis of the histomorphometric data from the histological sections obtained from the uninjured tissue on day 1 of the experiment confirmed that there were no statistically significant differences in the number of fibroblasts or blood vessels between the animals in the different treatment groups (Tables 1 and 2). The representative distribution of fibroblasts and blood vessels in the scar tissue of the different groups is shown in Fig. 1.
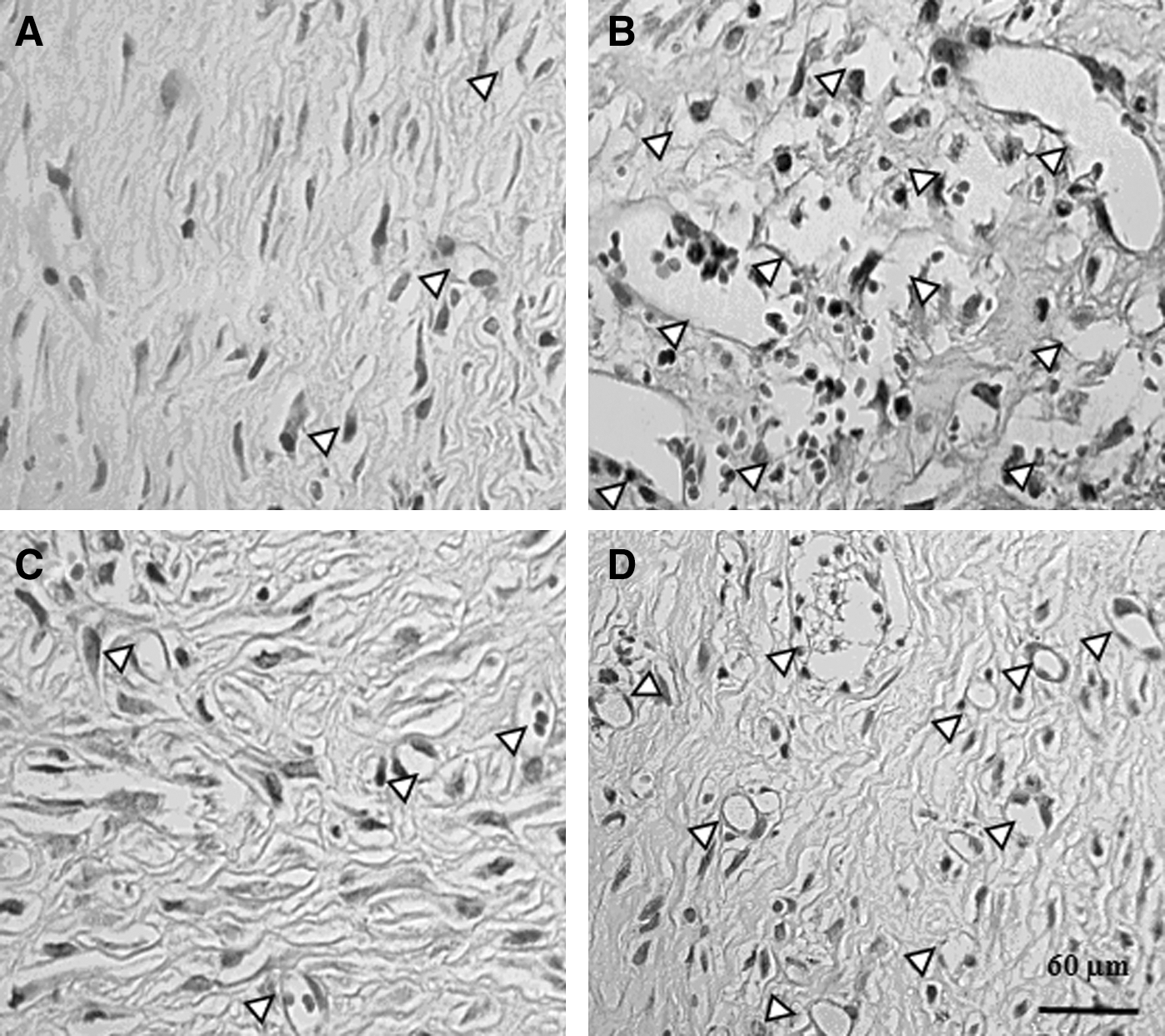
Representative photomicrographs of histological sections of skin of rats on day 20 of experiment stained with hematoxylin and eosin and observed under the light microscope. The animals received: A, saline 0.9%; B, healing oil; C, Laser GaAsAl 30 J/cm2; D, Laser GaAsAl 60 J/cm2. Arrowheads indicate blood vessels. Magnification 200×.
Different letters in columns indicate statistically significant differences between groups (p < 0.05), Kruskal–Wallis test. Groups: L30, laser 30 J/cm2; L60, laser 60 J/cm2; Oil, healing oil; Control, saline 0.9%.
Different letters in columns indicate statistically significant differences between groups (p < 0.05), Kruskal–Wallis test. Groups: L30, laser 30 J/cm2; L60, laser 60 J/cm2; Oil, healing oil; Control, saline 0.9%.
On day 4 of the experiment, a greater quantity of fibroblasts and blood vessels was found in the granulation tissue of the wounds treated with the oil, the 30 J/cm2 laser, and the 60 J/cm2 laser compared to the control group, although this difference was only significant in the case of fibroblasts (p < 0.05; Tables 1 and 2).
On day 8, there was a significantly greater quantity of fibroblasts in the group treated with the healing oil compared to the L30 and L60 laser groups (p < 0.05). The quantity of blood vessels was significantly greater in both laser-treatment groups in comparison with the control group and with the group treated with oil, the most significant result being in the L60 group (p < 0.05; Tables 1 and 2).
On day 12 of the experiment, no statistically significant difference was found between the groups with respect to fibroblasts or blood vessels (Tables 1 and 2). On the day 16, there was no statistically significant difference between the groups with respect to the number of fibroblasts; however, the quantity of blood vessels in the wounds of the animals in the L60 group was significantly greater compared to those of the L30 or healing oil groups (p < 0.05; Table 2). At the end of the experiment, on day 20, there was no statistically significant difference in the quantity of fibroblasts or blood vessels between the groups investigated (Table 1 and 2).
The collagen maturation index calculated for all the wounds showed that, at all time points, collagen maturation was greater in the group treated with the 60 J/cm2 laser compared to the other groups. Collagen maturation was significantly greater on days 4 and 20 of the experiment in the L30 group compared to the control and healing oil groups. Moreover, on day 16, the collagen maturation index was significantly higher in the groups treated with the 30 J/cm2 laser and oil compared to the control group (Fig. 2).
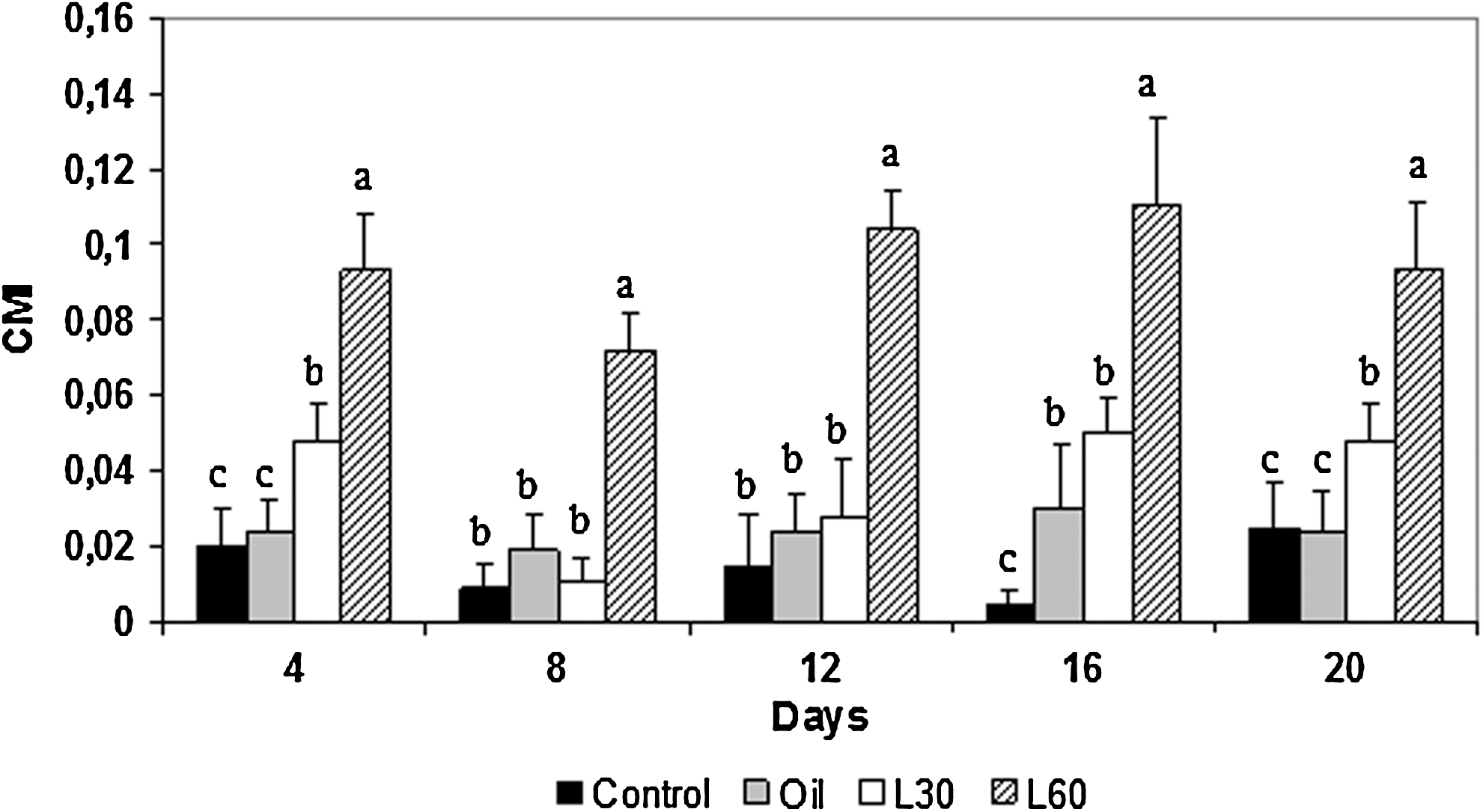
Collagen maturation index (CMI) of skin wounds of Wistar rats during 20 d of treatment with: L30, laser 30 J/cm2; L60, laser 60 J/cm2; Oil, healing oil; Control, saline 0.9%. a,b,cDifferent letters in columns indicate statistically significant differences between groups (p < 0.05), Kruskal–Wallis test.
Discussion
There are various reports in the literature on the benefits of laser treatment in the different phases of the healing process. This therapy has been shown to have a positive effect on angiogenesis, collagen deposit, and fibroblast proliferation. 2,3,6,7,21 Nonetheless, data on the most appropriate wavelength and energy density to assure optimal results are conflicting. 6,22,23 Other studies have shown the benefit of the use of oils consisting of a combination of medium chain triglycerides and essential fatty acids in stimulating the healing process of skin wounds. 5,14,16 Although the use of these oils is common in clinical practice, it remains unclear which aspects related to the healing process are most stimulated by this therapy. In the present study, LLLT, at the doses of 30 J/cm2 and 60 J/cm2, and healing oils were used on second-intention skin wounds characterized by a large loss of tissue and a marked production of granulation tissue. 4,5
Various studies have shown that the selection of parameters such as the wavelength and the energy dose of laser light are capable of stimulating different aspects of the healing process such as cell and vascular proliferation and collagen synthesis. 3,6,21 There is evidence that collagen concentration is a determining factor in the quality of healing. 1,4,8,9 In addition, collagen production has been reported to be affected by an inversely proportional correlation between wavelength and energy density. 3,6,21 Although this correlation has been reported in some studies, it remains to be fully clarified. In the present study, LLLT with a high wavelength and an energy dose of 60 J/cm2 was more effective in stimulating the production of type I collagen, which characterizes greater collagen maturation (Fig. 2). Better collagen maturation of scar tissue has important implications in the increase of the mechanical resistance of the newly formed tissue. The first collagen to be formed in the healing process is type III collagen that serves as support for the deposit of type I collagen, which is thicker and renders the scar more resistant to traction. 24,25 The increased resistance of scar tissue occurs throughout the collagen remodeling process due to the gradual substitution of collagen type III fibers for type I and by the increase in hydrogen bridges between its molecules. 1,4,11 According to Meirelles et al., 3 marked maturation of granulation tissue is found on day 21 of treatment using the 20 J/cm2 laser. In addition, Mendez et al. 6 showed that the GaAsA1 (λ 830 nm) laser, administered at higher energy doses (50 J/cm2), was able to promote intense collagen deposit and maturation in skin wounds in rats.
In the present study, the quantity of fibroblasts on day 4 of the experiment was greater in all the wounds treated with the laser or oil compared to the controls. However, on day 8, the oil proved to be more effective in increasing these cells in the scar tissue. Studies have shown that essential fatty acids and medium chain triglycerides contribute positively to the healing process of skin wounds by increasing cell nutrition and producing growth factors that stimulate cell proliferation. 5,14 These lipid compounds promote hydration of the scar tissue, contributing toward autolytic debridement and re-epithelization. 5 Moreover, there were fewer fibroblasts in the group treated with the 30 J/cm2 laser. It is interesting to note that collagen maturation indexes were higher in the L30 group compared to the oil and control groups; nevertheless, no similar effect was found on the quantity of fibroblasts. Therefore, it is evident that further studies need to be carried out to investigate the ultrastructural and metabolic modifications caused by the different doses of LLLT energy in the cells and to examine which mechanisms stimulate collagen production, since studies evaluating the effects of LLLT at cell level are sparse. 26,27 In an extensive literature review, Reddy 8 reported that the positive photobiomodulation effect of the laser on fibroblastic proliferation occurs only at low energy doses such as 2 and 4 J/cm2. According to this author, higher doses may suppress the mitosis rate of these cells, which may partially explain the findings of the present study.
With respect to tissue vascularization, a greater quantity of blood vessels was found on day 8 in the group treated with the 60 J/cm2 laser compared to the other groups, a situation that was also found on day 16. Some studies have shown that the formation of a larger vascular network in granulation tissue contributes toward a faster and better healing process due to the greater influx of nutrients and efflux of metabolites from the area of the wound. 28,29 Corazza et al. 10 showed that on day 21 of their experiment, an energy dose of 20 J/cm2 effectively promoted angiogenesis in skin wounds induced in rats. There are reports that laser photobiomodulation is associated with a reduction in the inflammatory process 12 and with stimulation of the production of angiogenic growth factors by macrophages, T lymphocytes, fibroblasts, and keratinocytes. 30,31 Moreover, there is evidence that LLLT is capable of inhibiting nitric oxide production at the site of the lesion, thereby reducing the formation of reactive oxygen species and favoring neovascularization. 28,29
Conclusion
The present study analyzed the effect of LLLT and healing oil on different parameters of the healing process such as fibroblasts, blood vessels, and also on collagen maturation, indicating that these therapeutic modalities may interact effectively with different elements in scar tissue. Results show that the 60 J/cm2 laser was more effective in stimulating angiogenesis. In addition, the 60 J/cm2 and the 30 J/cm2 laser were both more effective in promoting collagen maturation in the scar tissue of rats, respectively. In addition, the healing oil was the most effective method for the stimulation of fibroblast proliferation. In view of the effect of LLLT and of the combination of healing oil consisting of essential fatty acids and medium chain triglycerides on different aspects related to wound healing, additional studies should be carried out to investigate combinations of these resources with the objective of developing a more effective therapeutic strategy for the treatment of skin wounds.
Footnotes
Author Disclosure Statement
No competing financial interests exist.