
Abstract
Introduction
On the basis of its analgesic and wound-healing effects, laser phototherapy (LPT) has been used to prevent and treat oral lesions. 4 –6 Its efficacy is based on its capacity to modulate various metabolic processes through the cellular effects of its radiation energy. 7 It also has proven to be simple to apply, atraumatic, and well tolerated by the patients. 4
The oral lesions of SJS often make it difficult for patients to open their mouths to eat, drink, or speak. No current interventional technique is completely successful at preventing or treating these lesions. A treatment that can promote healing of the ulcerative lesions and decrease the pain and other symptoms of SJS, thus improving the basic oral functions and reducing the risk of secondary infections in patients with the condition, is therefore essential. In this context, we report LPT as a potentially new adjuvant treatment modality for SJS.
Clinical Case Report
A 7-year-old boy was admitted to the Intensive Care Unit (ICU) of the Hospital Universitário of the Univesidade de São Paulo (USP, Sao Paulo, Brazil). He was first seen with fever, respiratory distress, and lesions (blisters developed on widespread purpuric macules) on his extremities, trunk, face, and neck, as well as on his conjunctivae and on the mucosa of his genitalia. He also had swollen, bleeding, and crusted lips, and the clinical examination revealed diffuse ulcerative intraoral lesions (Fig. 1A). He was unable to speak or open his mouth, and reported severe and constant oral pain that rendered him unable to eat any solid food and required a feeding tube for his nutrition. His cutaneous and intraoral lesions and symptoms had developed after treatment with phenobarbital for a seizure disorder for approximately 30 days. It was the first time that the patient had these clinical manifestations. The diagnosis of SJS was decided after clinical examination of the body lesions in association with the patient's medical history. After that, he was transferred to ICU. In an attempt to prevent and minimize secondary infections, gastric problems, pain, and other complications, the patient was given medicines such as clindamycin, ranitidine, dipyrone, diphenhydramine (Benadryl) drops, and morphine. In addition, he was instructed to use bicarbonate solution and ketoconazole (Xylogel) in the oral cavity, none of which seemed to provide any benefit. On the fifth day after his admission, he underwent a dental examination, and because of the lack of progress of the patient, laser phototherapy (LPT) was indicated.
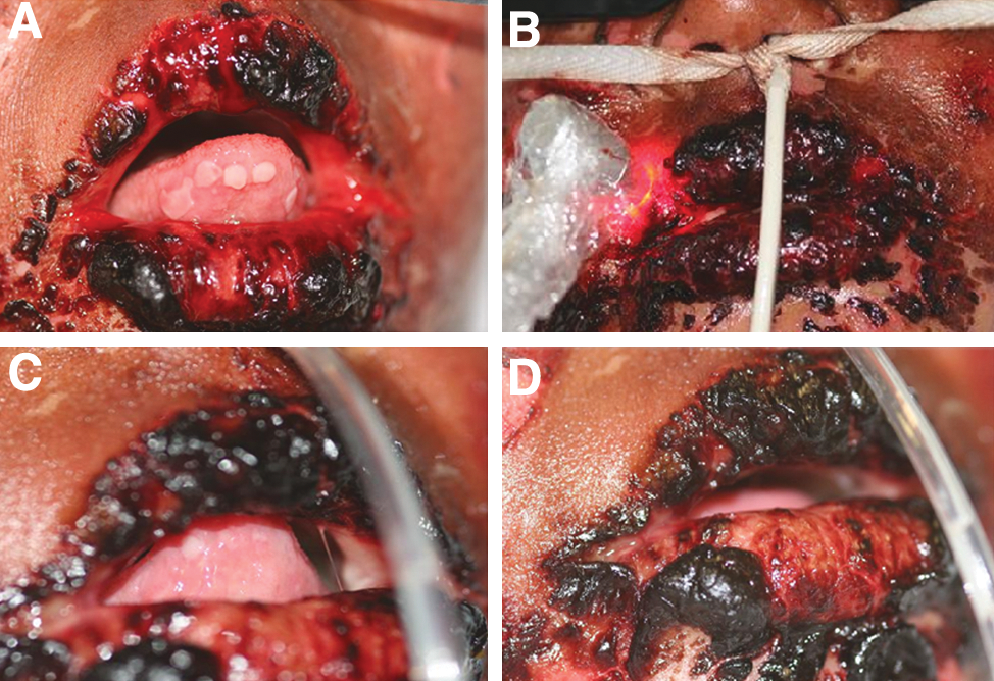
Clinical appearance of patient's lesions before first (
The patient underwent both extra- and intraoral LPT. The extraoral therapy was delivered with a 660-nm InGaAlP laser (Twin Laser; MMOptics Ltd., São Carlos, SP, Brazil). The irradiation was delivered with the laser tip in direct contact with and perpendicular to the patient's oral mucosa and lips, and lesions on the patient's perioral skin were treated in the same way (Figs. 1B and 2A). The laser settings were 15 mW and 3.8 J/cm2, at an energy of 0.15 J per treatment point and a laser-beam spot size of 0.04 cm2 for 10 s per treatment point. The irradiance was 0.375W/cm2. For intraoral LPT (Photon Laser DMC, São Carlos, São Paulo, Brazil), because of the patient's difficulty in opening his mouth, a smaller spot size, 0.028 cm2 per treatment point, was used for his oral lesions, at 100 mW and 7.1 J/cm2, and with an irradiation time of 2 s per treatment point. The irradiance was 3.571W/cm2. Lesions on the patient's tongue were treated with direct application of the laser tip, and areas of ulceration on the patient's oral mucosa were treated with the laser in the defocused mode (Fig. 2B).

Extra- (
Results
A few minutes after the first session of LPT, the patient was able to eat gelatin delivered through a syringe. Healing of his lesions became evident on the following day, with a decreased severity, which was marked mainly by a reduction in the size of the lesions on the patient's tongue and the appearance of drier crusts of his lips (Fig. 1B–D).
Debridement of the patient's dermal lesions was done on the fifth day after his initial session of LPT, when both the number and severity of his oral lesions had decreased. It is important to highlight that the oral lesions were always more severe than most of the skin lesions, and that, after the debridement, the dermal lesions showed a great improvement. It is also important to remember that laser phototherapy was applied by a dentist, and therefore, only the face and mouth lesions received the irradiation.
On the fifth day, the patient was able to open his mouth easily, to talk, laugh, and eat gelatin and porridge. He reported feeling better and was also able to engage in easy activities, such as playing cards. On the sixth day after his initial laser treatment, he was able to eat solid food without assistance; his feeding tube was removed; and he left the ICU (Fig. 3A–C). Although few of the oral lesions remained, he reported them being painless (Fig. 3B and C).
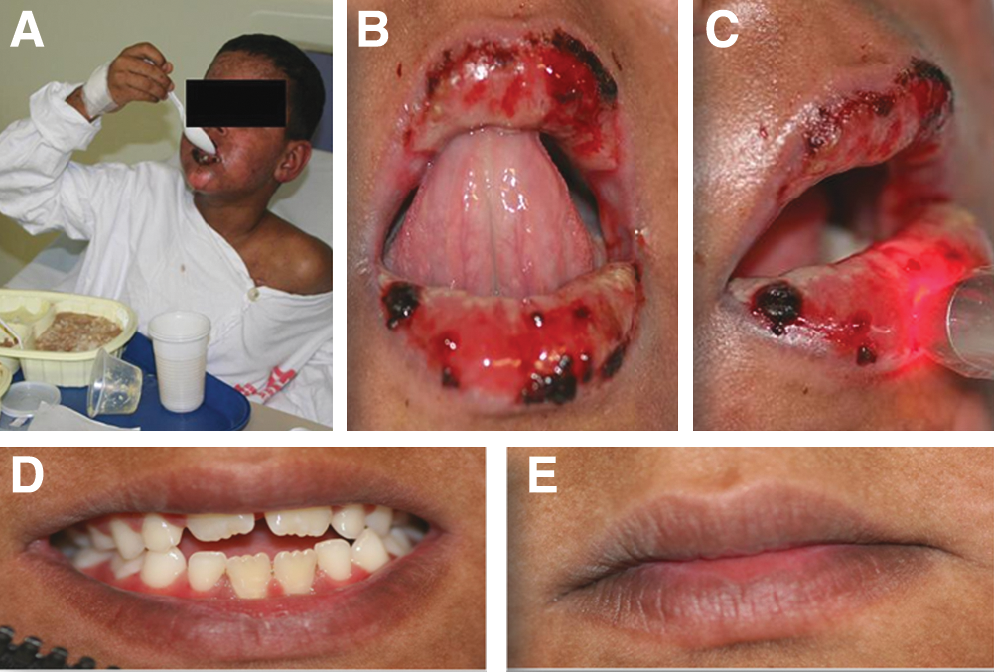
Clinical appearance of patient's oral lesions on the sixth day after initial application of LPT (
The patient was discharged from the hospital after 10 sessions of LPT, after which he underwent three further sessions at the Special Laboratory of Lasers in Dentistry at the University of São Paulo. At this time, the complete healing of his oral lesions was observed (Fig. 3D and E).
Discussion
In this case, LPT was effective at healing the oral lesions of an SJS patient and relieving the pain associated with this manifestation. These results accord with other clinical findings regarding the efficacy of LPT in treating ulcerative oral lesions, 4 –6 but seem noteworthy in terms of rapidity of lesion remissions; as in the present case, the healing of the lesions on the patient's tongue was observed after a single laser treatment. The results of LPT in this case also accord with those of other studies in showing that LPT can improve quality of life by relieving pain and facilitating such basic oral functions as drinking, eating, and speaking. 4 –6,8 The healing effected by LPT in the case described also decreased the patient's risk for secondary infection.
Laser radiation in the visible spectrum is absorbed by chromophores in the mitochondrial respiratory chain, with a consequent increase in production of adenosine triphosphate (ATP), which in turn increases cell proliferation and protein synthesis, aiding in tissue repair. 7 Our research group has shown that LPT can upregulate cell proliferation, modify cytokine production, increase mast cell degranulation, 9 –11 and may thus have beneficial effects in SJS, because all of these processes are physiologically related to inflammation and wound healing.
LPT can be advantageous because the window of its therapeutic antiinflammatory effect overlaps that of its ability to enhance tissue repair and to alleviate pain. The reason for the analgesic effect of LPT is still not fully clear; some investigators attribute it to the stabilization of the neuronal cell membrane through promotion of a more-stable conformation of the membrane lipid bilayer and of the proteins integrally associated with the neuronal membrane. 12 The laser-induced enhancement in production of ATP also was shown to restore the integrity of the neuronal membrane and to decrease the transmission of nociceptive impulses. 13 Additionally, LPT can enhance the production of endogenous opioids 14 and decrease serum levels of prostaglandin E2, a known mediator of inflammation. 15
Last but equally important is the widely established use of LPT as an adjuvant to traditional treatment measures. The case described here extends the benefits of LPT as a new adjuvant modality for SJS complications. In addition, more studies should be conducted analyzing the effect of LPT on dermal lesions of SJS patients.
Footnotes
Acknowledgments
We express our gratitude to the Laboratório Especial de Laser em Odontologia of the Universidade de São Paulo, the Fundação de Apoio à Pesquisa do Estado de São Paulo (FAPESP #2005/57578-8), and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq #305574/2008-6). We also thank Mariana Aparecida Brozoski and Professor Antonio Carlos de Campos of the Hospital Universitário of the Universidade de São Paulo.
Author Disclosure Statement
The authors have no competitive financial interests in this work.