
Abstract
Introduction
Diabetes mellitus is a chronic disease characterized by partial or total deficiency of insulin production or a resistance to its action. 5 Metabolic disturbances such as diabetes may further compromise the clinical status of patients with burns due to delayed healing and increased risks of infections. 6 Diabetes causes delayed healing through several pathways: reduced chemotaxis of leukocytes; changes in oxygen diffusion, reduced nutrient transport, decreased number and activity of fibroblasts, impaired capacity of collagen synthesis and delayed maturation and instability of the collagen, and increased number of plasmocytes. 5,7 –10 Additionally, patients with uncontrolled diabetes may show impaired vision, 11 diabetic angiopathy, arteriosclerosis, impaired leukocyte activity ROS activity, as well as decreased production of IL-2. 12
Impaired wound healing in patients with diabetes is well documented in the literature as are the therapeutic approaches used to quicken the repair process in these patients. However, studies on the repair of burns in patients with diabetes are scarce, especially for the use of phototherapies. 13
Previous reports have shown positive effects of the Bioptron® lamp with 95% polarization on promoting faster wound repair and healing. 14 –16 The incoherent polarized light from this lamp can induce biostimulative effects in living cells similar to low-level lasers. Because the Bioptron lamp combines visible light at λ480–700 nm and infrared light at λ700–2000 nm, it is a low-intensity light source, like a low-level laser, but it is polychromatic and incoherent. 17
Several mechanisms are responsible for the photobiostimulating effects of both parts of the electromagnetic spectrum present in this polychromatic light source. Both types of light lead to the same final photoresponse, but the cascade of metabolic events starts at different cellular levels for each. One of the main effects of the absorption of visible light is the stimulation of the mitochondria, which results in increased cell energy and activation of nucleic acid synthesis, essential for wound repair. The use of infrared light has the same end results, but the process is initiated by a response at the membrane level. Biomodulation is influenced by common characteristics of polarization for both types of light. 16
There are several factors that are important for the outcome of treatments involving light sources. Most of the proposed protocols use different parameters, which results in conflicting results. The selection of appropriately defined parameters, including wavelength, power density, energy, and application time and frequency, is essential for achieving desired treatment results. 18,19
The present study aimed to assess the effects of a polarized light source on the healing process of third-degree burns on diabetic Wistar rats.
Materials and Methods
Following approval by the Animal Experimentation Ethics Committee of the School of Dentistry of the Federal University of Bahia, 45 young adult male Wistar rats weighing 200–230 g were obtained from the animal breeding facility of the College of Veterinary Medicine of the Federal University of Bahia, and were kept at the Animal Experimentation Laboratory of the School of Dentistry of the Federal University of Bahia. The animals were kept in individual plastic cages lined with wood chips and were maintained at 22°C in a 12/12 h day/night light cycle. The animals were fed a standard laboratory diet and had water available ad libidum. After a regular quarantine period, the animals were randomly distributed into three groups of 15 animals each as follows: G1: control (no treatment); G2: polarized light (λ = 400–2000 nm, 20 J/cm2); and G3: polarized light (λ = 400–2000 nm, 40 J/cm2). Each group was then divided into three subgroups of five animals each according to the planned time of death. Food was withheld from the animals for 12 h, after which they were injected with streptozotocin (Sigma Aldrich) diluted in citrate buffer (0.1 M, pH 4.5, 60 mg/kg). 20 Forty-eight hours after injection, the blood sugar level was measured and only animals with blood sugar levels of 350 mg/100 mL or higher were included in the study. 20 Under intraperitoneal general anesthesia (0.10 mL/100 g of ketamine and 0.25 mL/100 mg of xylazine) the animals had their dorsum shaved and cleaned. Next, a specially designed instrument measuring 1.5 by 1.5 cm was heated until red and incandescent and then applied to the skin of the anesthetized animals for 20 sec to induce a third-degree burn. Phototherapy was performed on groups G2 and G3 (Bioptron, λ400–2000 nm, 40 mW/cm2, 2.4 J/cm2 per min, 5.5-cm beam diameter, 23.7-cm2 beam area, 3.7 W).
Phototherapy started immediately post-burning and was repeated daily until the day before death. The energy was applied transcutaneously observing a distance of 10 cm as recommended by the manufacturer. The dose was 20 or 40 J/cm2 (255 or 510 sec). The total number of sessions of phototherapy varied based on the time of death: 7, 14, or 21 d.
At 7, 14, or 21 d post-burning, and following macroscopic examination, animals were killed by an overdose of general anesthetic. Tissue specimens were taken and kept in 10% formalin for 24 h. They were then routinely embedded in paraffin, sectioned, stained with HE or Sirius red or immunomarked with CK AE1/AE3 (Dako Cytomation® +streptoavidinbiotin peroxidase, 1:200) antibody. An experienced pathologist, blinded to the protocols, completed qualitative and semiquantitative histological analyses of the coded specimens under light microscopy. Three slides were made from each specimen and the whole area was analyzed. The variables used for this analysis are shown in Table 1. 13 These variables were used previously 13,21 and included inflammatory reaction, re-epithelialization, number of fibroblasts, and amount of collagen deposition and neoangiogenesis. The scoring system was based upon the number of samples with the observed grading. Statistical analysis was carried out by the Fisher's test due to the small sample size, and the significance level was set at 5%.
Results
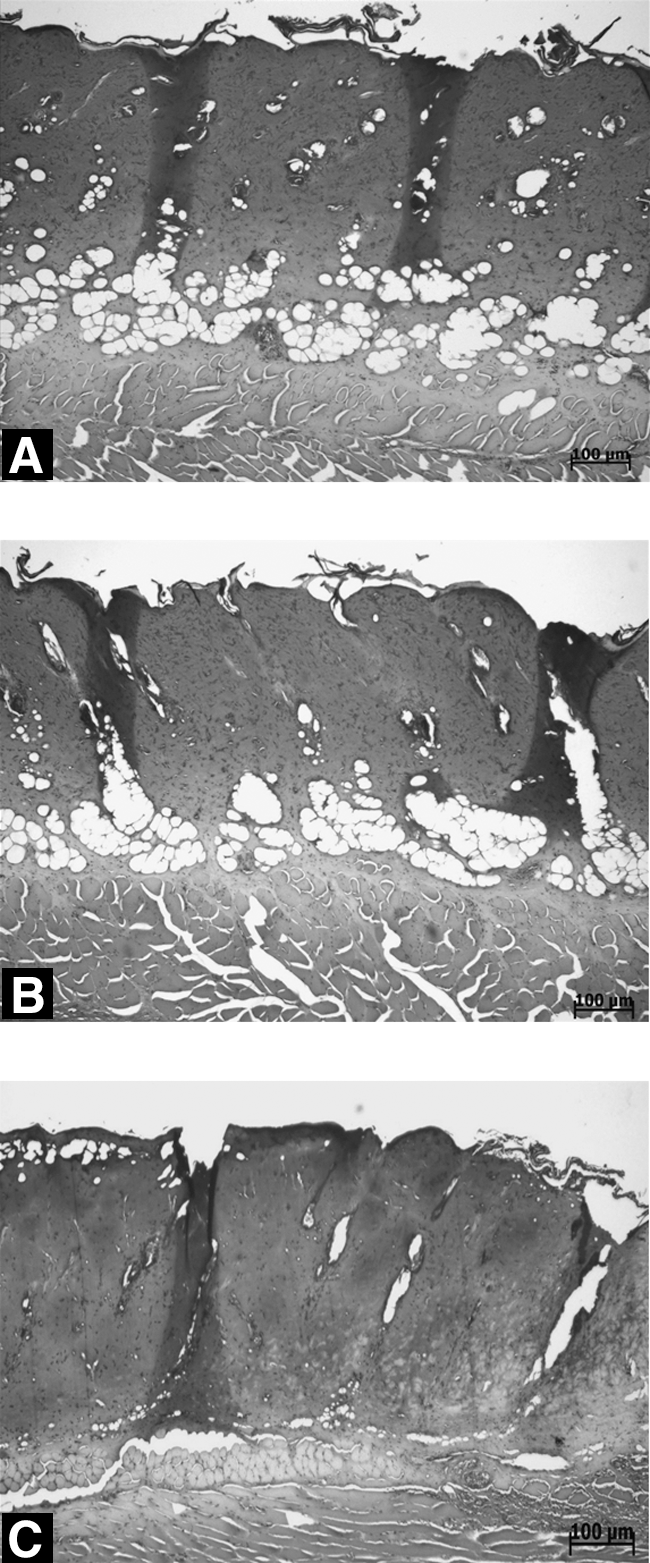
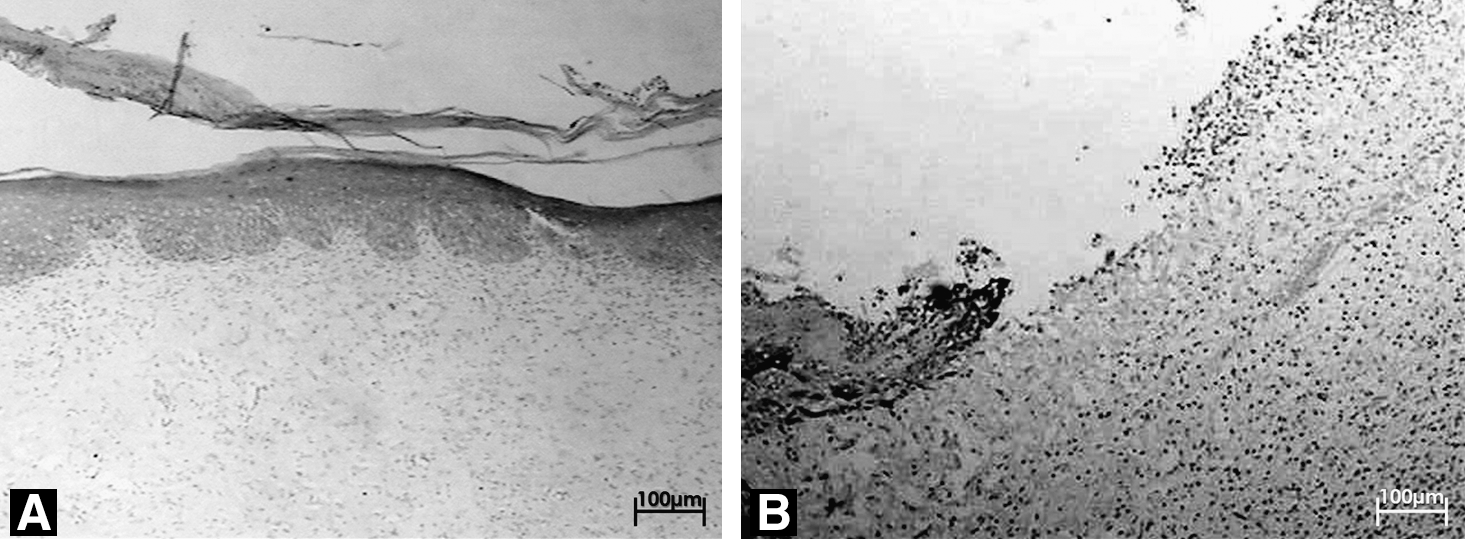
On day 7, all specimens showed the presence of necrotic skin fragments extending down to the muscle (Fig. 1). Most G1 (80%) and G3 (60%; 40 J/cm2) animals showed chronic inflammation at this time (Fig. 2). G2 subjects showed variable inflammatory infiltrate: acute (20%), chronic (40%), or mixed (40%). Angiogenesis and fibroblast number were significantly lower in G3 subjects when compared to either G1 or G2 animals (Fisher's test, p = 0.02 and p = 0.03). G1 and G2 specimens were most similar with regard to re-epithelialization, which was mostly discrete (Fig. 3). G3 subjects did not show evidence of re-epithelialization in most cases.
Photomicrograph of
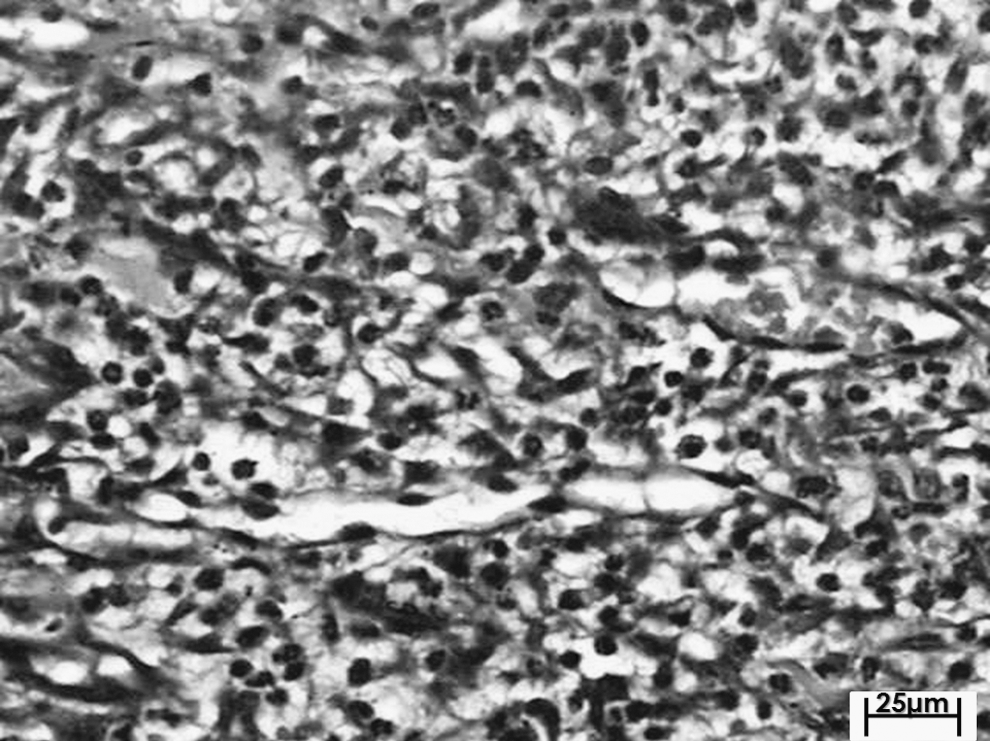
Photomicrograph of a control specimen at day 7 post-burn, showing moderate chronic inflammation, predominantly lymphoplasmocitary cells (HE, 25 μm).

Photomicrograph of
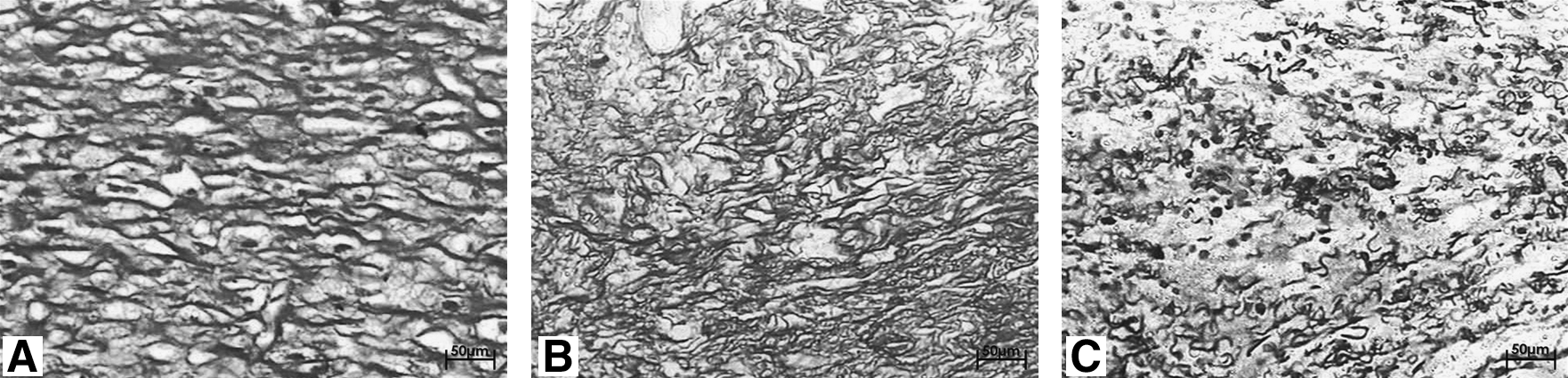
Fourteen days after burning, 60% of G1 specimens showed evidence of a mixed moderate inflammatory infiltrate. Illumination (20 J/cm2) again demonstrated wide variation in the inflammatory reaction: acute (20%), chronic (40%), or mixed (40%). G3 specimens showed a moderate or intense chronic inflammatory reaction in 80% of the cases. These specimens also showed significantly less crusting than the controls (Fisher's test, p = 0.03). Both illuminated groups had a significant increase in angiogenesis when compared to controls (Fisher's test, p = 0.03, Fig. 4). G3 specimens showed a significant increase in the number of fibroblasts when compared to both G1 and G2 samples (Fisher's test, p = 0.01). Re-epithelialization was more evident in G1 specimens than those from G2 subjects (Fisher's test, p = 0.03). Collagen deposition was significantly higher (increased density) in both G1 and G2 specimens when compared to G3 (Fisher's test, p = 0.03, Fig. 5).
Photomicrograph of
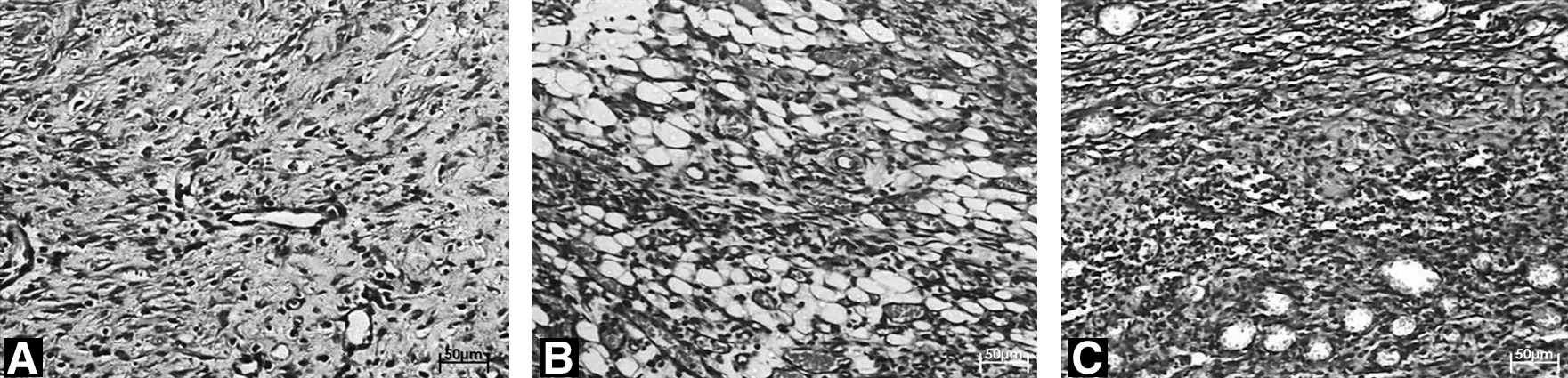
At the final observation time (21 d), abcess and edema were observed in two G3 subjects. G1 subjects showed intense mixed inflammatory reaction in 60% of the animals (Fig. 6). Illuminated subjects showed a predominantly lymphoplasmocitary inflammatory infiltrate, which was observed in 60% of the G2 animals and 80% of the G3 animals (Fig. 7). Sixty percent of G1 specimens showed a discrete number of fibroblasts at this stage. In 60% of the G3 subjects, there was a moderate number of these cells, and in 60% of the G2 specimens, the number of fibroblasts was marked and these cells were parallel to the surface. G3 specimens showed significantly higher levels of angiogenesis and collagen deposition when compared to their controls (p = 0.01). Most of the G2 subjects (60%) showed complete epithelial pavementing, while only one G3 subject showed complete pavementing (Fig. 8). A summary of the results is presented in Table 2.

Photomicrograph of a control specimen at day 21 post-burn, showing intense mixed inflammatory reaction (HE, 50 μm).

Photomicrograph of a 40 J/cm2 specimen at day 21 post-burn, showing moderate lymphoplasmocitary inflammatory infiltrate (HE, 50 μm).
G1, control; G2, 20 J/cm2; G3, 40 J/cm2.
Discussion
Despite therapeutic advances and growing awareness of the mechanisms of burn repair that have greatly improved treatment outcome over the past few years, these lesions still show both high morbidity and mortality rates. These rates are increased with the simultaneous occurrence of other diseases, such as uncontrolled diabetes, that may severely impair the repair process. 13 Long-term treatment and its disabling effects greatly impede patients' return to their daily activities, and the development of new therapeutic approaches to hasten recovery is greatly desired.
Several reports have shown the efficacy of polarized light sources on speeding wound repair, 22 –24 but there are not many reports on the use of this method for burn healing complicated by a debilitating metabolic disease such as diabetes mellitus. This situation prompted the present study, and the adopted protocol has been used by our group in other studies. The use of different doses in the present investigation is justified by the lack of previous studies using a similar model.
Our results showed that subjects illuminated with 20 J/cm2 (G2) had more positive responses for the majority of the criteria assessed, including increased angiogenesis at early stages of the repair process as well as increased re-epithelialization at the end of the experimental time, when the burned site showed clinical signs of tissue normality. These findings aligned with those from previous reports, 17,22,24 which used the same light source and a similar dose of 20 J/cm2 and found quicker repair and improved scar tissue quality when compared with nonilluminated subjects or to subjects illuminated with different doses.
Although subjects illuminated with 40 J/cm2 (G3) showed positive effects in both fibroblast proliferation and angiogenesis, this dose inhibited re-epithelialization. This may further confirm the existence of a therapeutic window as previously reported 25 and also supports data from Saudi Arabia in which λ670 nm laser light used with low doses (1–5 J/cm2) showed beneficial effects on burns, while higher doses (38 J/cm2) inhibited the process. 26
The use of phototherapies to quicken the repair of burns in a model similar to ours has been reported in the literature. In a previous study using polychromatic light-emitting diodes (272 mW, 13.6 mW/cm2, 5 J/cm2, 10 J/cm2, 20 J/cm2, and 30 J/cm2), Al-Watban and Andres 27 showed that the effects of the light were more evident when there was a metabolic deficit (diabetes). 16,27 Another study from our group 13 used λ660 and λ780 nm laser light (35 mW, Φ = 2 mm, and 20 J/cm2), which were also found to have positive effects on burns. We found increased deposition of collagen fibers, larger amounts of granulation tissue, less edema, a more vigorous inflammatory reaction, and increased revascularization on all laser-treated animals.
Our results suggest that the use of polarized light at a dose of 20 J/cm2 is effective on improving the healing of third-degree burns in diabetic animals at both early (angiogenesis) and late stages (re-epithelialization) of repair.
Footnotes
Author Disclosure Statement
No competing financial interests exist.