
Abstract
Introduction
Periodontal tissue begins healing by the adhesion of a blood clot to the root surface, stabilized by a network of fibrin. It is through this network that undifferentiated cells from the periodontal ligament migrate toward the root surface to begin formation of collagen fibers. This prevents apical migration of junctional epithelium allowing regeneration of cementum, periodontal ligament, and alveolar bone. 2,3
Scaling and root planing with manual curettes is the most recognized treatment for periodontal disease. However, studies disclose limitations for promoting a root surface compatible with regeneration, because a manual curette does not completely remove the microorganisms and their products embedded in cementum or dentin. 4,5 After scaling and root planing, a smear layer forms, which hinders migration of undifferentiated mesenchymal cells to the root surface. 6
Some treatments have been proposed to make root surfaces more compatible with regenerative processes, such as use of biomodification chemical agents 7,8 and more recently laser therapy 2 to remove the smear layer and expose the organic collagen matrix allowing the clot to bind better to the root surface.
The Er,Cr:YSGG (Erbium, Chromium: doped Yttrium, Scandium, Gallium, Garnet) laser, first indicated for removal of caries and preparation of cavities, was approved by the FDA in 2002 for bone cutting and resection. The laser wavelength of 2.78 μm provides a high degree of absorption by water, thus acting on mineralized surfaces by vaporizing water from mineralized tissues. This reduces thermal effects, especially when used together with cooling water that may damage dental pulp. The Er,Cr:YSGG laser used on the surface of root canal walls promoted removal of the smear layer and opened dentinal tubules, 9 also substituting scaling and root planing with manual instruments 10 or an ultrasound system. 11 However, no research was found in literature that evaluated the effect on adhesion of blood components to root surfaces after Er,Cr:YSGG laser irradiation.
The aim of this in vitro study was to evaluate the effects of Er,Cr:YSGG laser irradiation on root surfaces for the adhesion of blood components and surface morphology.
Material and Methods
Fifteen uniradicular or multiradicular teeth, extracted from patients with severe periodontal disease and attachment loss of more than one third of the root, were prepared for study. Four patients, three male and one female, with chronic generalized periodontitis aged between 40–65 years were selected. Exclusion criteria were: (1) periodontal treatment within the last 12 months; (2) systemic disease that could influence the outcome of periodontal therapy; (3) use of antibiotics and/or mouthwash within the last 6 months; (4) use of anti-inflammatory drugs within the last 3 months; and (5) a smoking habit. This study was approved by the Ethical Committee of the Araraquara Dental School, UNESP (CEP-FO/Car. no. 32/08).
Specimen preparation
Tooth specimens were cleaned in distilled water after extraction to remove blood and residues before being stored in a phosphate buffer solution (PBS) pH 7.0 at room temperature to maintain hydration prior to use.
The mesial and distal cervical third of the roots of these teeth were bordered by two parallel grooves made with a carbide multiblade drill. The first groove was made at the cementum–enamel junction, whereas the second was 5 mm distant on the root surface in the apical direction from the first groove. Then, a slowly rotating diamond-coated disk was used to section the teeth. The roots were crosscut in the first groove, separating them from the crown. The roots were cut lengthwise in the buccal–lingual orientation, and then in the mesio–distal orientation until the second grove was reached apically. The samples were crosscut and separated in two samples of about 2 × 2 mm in the mesio and distal surfaces to examine adhesion of blood components and root surface morphology on the same root face, totaling four specimens per tooth and therefore 60 specimens, which were divided into three groups of 20 specimens for each group.
Treatments groups
All the specimens were randomly assigned to one of the following groups of 20 each:
Group 1 (G1) specimens were treated by scaling and root planing (SRP), which was done by 50 traction movements in the cervical–occlusal direction with a manual curette (Gracey curette, no. 5–6; Hu-Friedy, Chicago, IL), carried out by only one trained operator.
Group 2 (G2) was irradiated by Er,Cr:YSGG laser (Waterlase YSGG; BIOLASE Technology) with a wavelength of 2.78 μm with a sapphire tip (G4; size 600 μm; length 4 mm; transmission factor 100%), with a power of 1.0 W and a frequency of 20 Hz (140–150 μs), irrigated with 10% air and 15% water for 30 s (29.99 J/cm2/pulse). The root was scanned in non-contact mode, with 45° angulations to the surface, by only one trained operator.
Group 3 (G3) specimens were treated by scaling and root planing (SRP), which was done by 50 traction movements in the cervical–occlusal direction with a manual curette (Gracey curette, no. 5–6; Hu-Friedy) combined with irradiation by Er,Cr:YSGG laser (Waterlase YSGG; BIOLASE Technology) with a wavelength of 2.78 μm with a sapphire tip (G4; size 600 μm; length 4 mm; transmission factor 100%), with a power of 1.0 W and a frequency of 20 Hz (140–150 μs), irrigated with 10% air and 15% water for 30 s (29.99 J/cm2/pulse). The root was scanned in non-contact mode, with 45° angulations to the surface, by only one trained operator.
After this, 10 specimens from each group were submitted to deposition of blood, whereas the remaining 10 from each group were morphologically evaluated. All specimens were microphotographed with a scanning electron microscope (SEM).
Preparation for adhesion of blood components
The methodology used for the preparation for adhesion of the blood components was according Theodoro et al. 2 Ten milliliters of blood were obtained by a syringe and needle from the peripheral circulation of a non-smoking adult (one male, aged 25 years) without systemic disease and use of antibiotics or/and anti-inflammatory drugs within the last 3 months. This was done in the School of Pharmaceutical Sciences at Araraquara, after agreement and signature of the Term of Free and Informed Consent no. 32/08.
In all the experimental groups, blood was deposited with a syringe and needle on the specimens, which were then maintained in a humidifier chamber for 20 min. Next, they were washed three times for 5 min each time with a PBS pH 7.0 in a shaker. Following this, specimens were identified and fixed in 1% formaldehyde and PBS for 15 min. After washing three times for 5 min each time with PBS, they were incubated for 10 min in 0.02M glycine and PBS, and washed again. They were then fixed in 2.5% glutaraldehyde and PBS for 30 min, and washed again. The specimens were dehydrated in solutions of increasing ethyl alcohol concentrations of 25%, 50%, 75%, and 95% for 10 min in each concentration prior to washing three times for 10 min each time in absolute ethyl alcohol. After drying, using a carbon dioxide critical point apparatus, specimens were fixed on metal stubs and placed in a vacuum desiccator for 48 h.
Preparation for root surface morphology
These specimens were dehydrated in solutions of increasing ethyl alcohol concentrations of 25%, 50%, 75%, 95%, and 100% for 1 h in each solution. Specimens were then placed in wells on an acrylic plate for application of hexamethyldisilazane (HMDS). First, each well received 0.8 μL of HMDS + 0.8 μL of absolute alcohol, measured by an automatic pipette (Boeco, Hamburg, Germany), where the specimens remained for 30 min. The solution was then removed, and the wells were filled with 1 mL of pure HMDS, and the specimens remained there for 10 min. The specimens were dried at ambient temperature for 20 min. After drying, using a carbon dioxide critical point apparatus, specimens were fixed on metal stubs and placed in a vacuum desiccator for 48 h.
SEM analysis
All specimens were metalized by sputtering in a Balt-Tec SCD-050 device for 120 s. Analysis was made with a SEM (JSM-330; Jeol, Tokyo, Japan) at 20 kV, and microphotographs were taken with a Fuji Neopan SS120 film at magnifications of 1000 ×, 1500 ×, and 2000 ×. Microphotographs were analyzed by one blinded single operator, previously trained, who described adhesion to the surfaces using the index of blood component adhesion 2 and morphology of the root surfaces with the modified index for analysis of morphology. 2
Index of blood component adhesion:
(0) absence of a fibrin network and blood cells
(1) scarce fibrin network and/or blood cells
(2) moderate fibrin network and moderate quantity of blood cells
(3) dense fibrin network and trapped blood cells.
The blood cells observed were platelets, erythrocytes, and leucocytes.
Modified index for analysis of morphology:
(1) rougher surface—presence of grooves, irregular aspect with microroughness similar to squamous and presence of dentinal tubules
(2) smooth surface: absence of grooves and craters, presence of smear layer and without exposure of dentinal tubules.
Statistical analysis
The computer program Bioestat 5.0 (Belém, PA, Brazil) was used for statistical analysis. Statistical differences between groups for adhesion of blood components and root morphology were evaluated by the Kruskal–Wallis nonparametric test (p < 0.05). The Mann–Whitney nonparametric test (p < 0.05) was used to identify the statistically significant differences between groups. The level of significance was set at 5%, and 95% confidence intervals (CI) were calculated.
Results
Analysis of blood component adhesion
In group 1 (SRP), six (60%) of these photomicrographed specimens had a score of 3 for adhesion, which describes a dense fibrin network with extensive interlacing and entrapped blood cells with presence of platelets (Fig. 1). The remainder had scores of 1 and 2, with two specimens (20%) in each group, indicating adhesion of a scarce fibrin network and/or blood cells and a moderate quantity of blood cells and a weak fibrin network with little interlacing respectively. No specimens were found with a score of 0 in this group.
Group 1 (SRP/Adhesion of blood components). Root surface showed dense fibrin network with presence of blood cells (platelets adhered in fibrin network ↑) (score 3) (bar = 10 μm; original magnification 2000 ×).
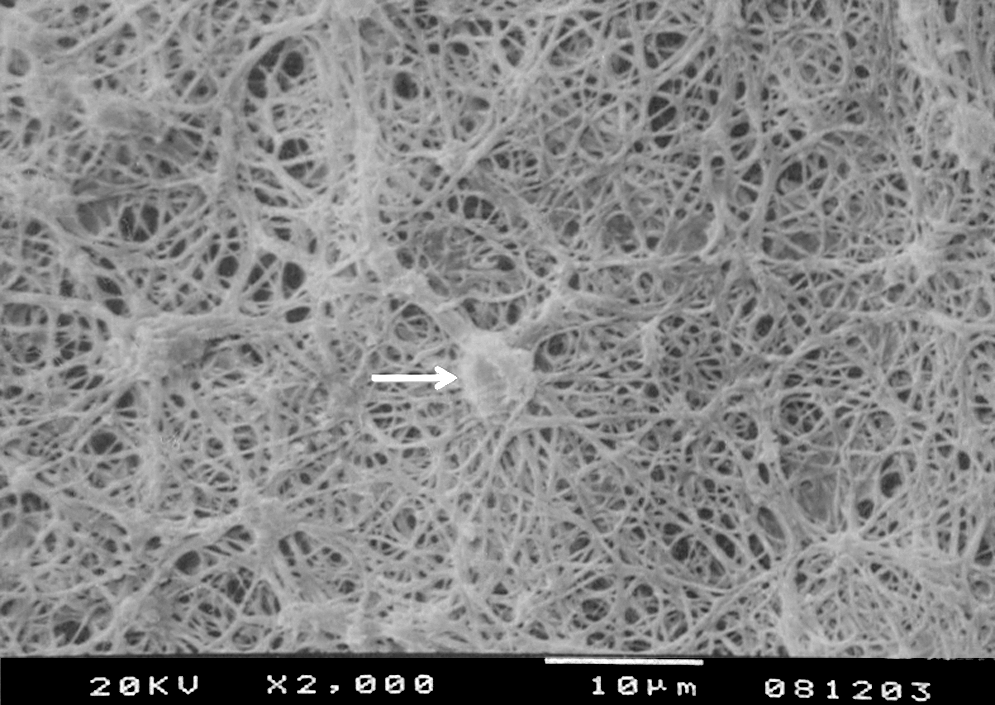
Group 2 (Er,Cr:YSGG laser) had a higher frequency (eight specimens, 80%) with a score of 3, disclosing a dense network of fibrin with extensive interlacing and entrapped blood cells: leucocytes (Fig. 2). Two specimens (20%) showed different scores, one specimen with adhesion of a scarce fibrin network and/or blood cells (score 1) and the other with no fibrin or blood cells (score 0).
Group 2 (Er,Cr:YSGG Laser/Adhesion of blood components). Root surface disclosed a dense fibrin network of with presence of blood cells entrapped (leucocytes ↑) (score 3) (bar = 10 μm; original magnification 2000 ×).
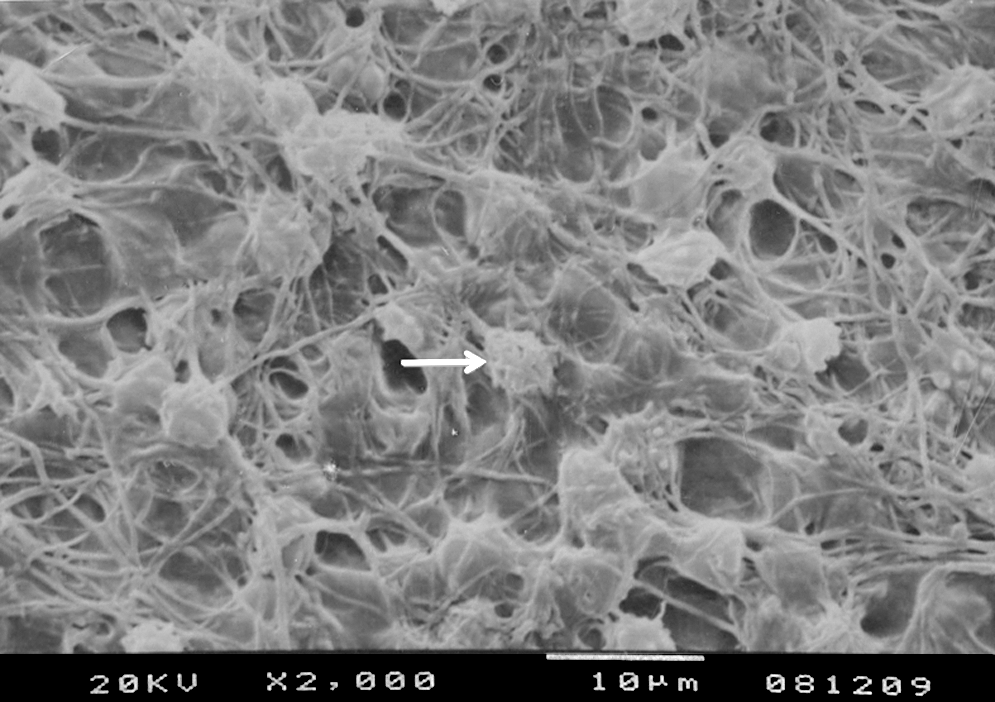
Group 3 (SRP + Er,Cr:YSGG Laser) showed a higher frequency with a score of 3 for adhesion of blood components, with five specimens (50%) found in this group, indicating extensive adhesion of a dense fibrin network and extensive interlacing and trapped blood cells: leucocytes (Fig. 3). Three specimens (30%) had a score of 0, with no adhesion of blood components, one specimen (10%) a score of 1, and another specimen (10%) a score of 2, describing, respectively, scarce adhesion with a fibrin network and/or blood cells and moderate quantity of blood cells and a weak fibrin network with little interlacing.

Group 3 (SRP + Er,Cr:YSGG laser/adhesion of blood components). Presence of blood cells (leucocytes ↑) entrapped in a dense network of fibrin on root surface (score 3) (bar = 10 μm; original magnification 2000 ×).
Analysis of root surface morphology
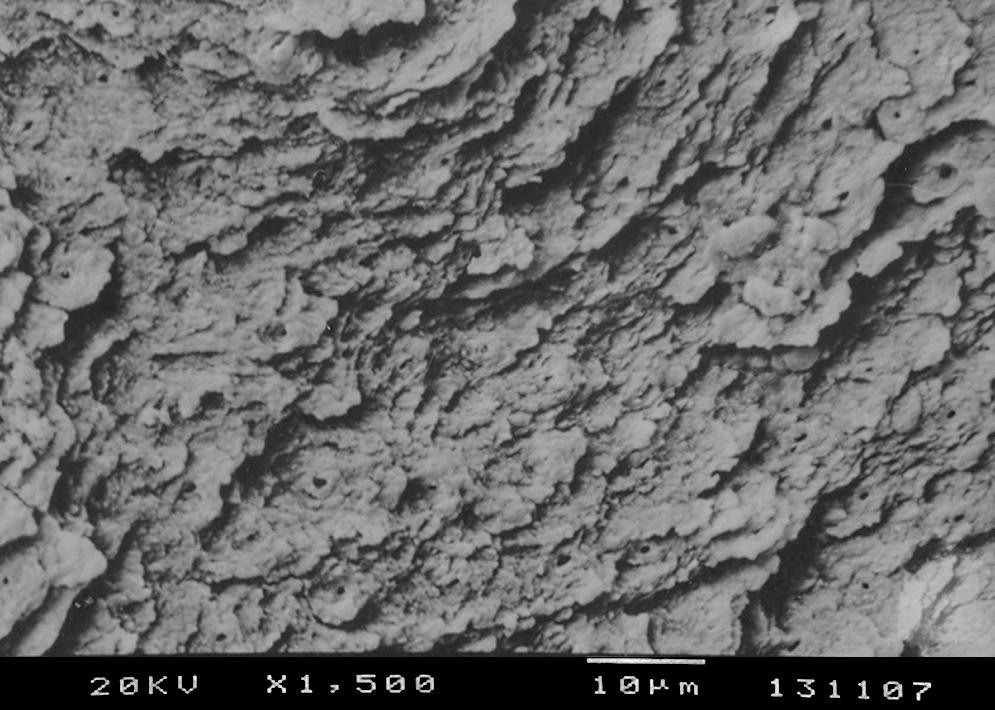
In group 1 (SRP), the photomicrographs were, in the majority, smooth, (nine specimens, 90%); only one specimen (10%) had a very rough surface (Fig. 4). All specimens had a smear layer and scratches without exposure of dentinal tubules.

Group 1 (SRP/morphological analysis). Root surface smooth and regular, with occluded dentinal tubules and presence of smear layer (score 2) (bar = 10 μm; original magnification 1500 ×).
In groups 2 (Er,Cr:YSGG Laser) and 3 (SRP + Er,Cr:YSGG Laser), the photomicrographs revealed that all (100%) specimens were very rough (Figs. 5 and 6), without the presence of a smear layer.
Group 2 (Er,Cr:YSGG laser/morphological analysis). Root surface irregular with microrugosity, partial occluded dentinal tubules and without smear layer (score 1) (bar = 10 μm; original magnification 1500 ×).

Group 3 (SRP + Er,Cr:YSGG laser/morphological analysis). Root surface irregular with microrugosity, open dentinal tubules and without smear layer (score 1) (bar = 10 μm; original magnification 1500 ×).
Statistical analysis
The nonparametric Kruskal–Wallis test (p < 0.05) evaluated the statistical differences between groups for adhesion of blood components. No statistically significant differences between groups (p = 0.3592) were found.
This test (p < 0.05) was also used for morphological analysis, disclosing significant differences between groups (p < 0.001). The Mann–Whitney test (p < 0.05) indicated that root surfaces irradiated by Er,Cr:YSGG laser were rougher than those only hand scraped (G1–G2: p = 0.0003, G3–G1: p = 0.0003).
Discussion
The objective of this in vitro study was to evaluate the effects of Er,Cr:YSGG laser irradiation on root surfaces for morphology and the adhesion of blood components, which represents the initial step of the insertion of the periodontium.
Specimens treated by Er,Cr:YSGG laser in this study presented a statistically rougher surface than those only scraped by manual instruments. This morphological pattern was found in other studies using Er,Cr:YSGG 11 –13 and Er:YAG lasers. 2,14 –16 Justification of this roughness is related to laser interaction with dental tissues. Er,Cr:YSGG and Er:YAG lasers have wavelengths that are well absorbed by water. This results in greater absorption of radiated energy from these lasers by water molecules in tissues. In dental tissue, a molecule of superheated water evaporates quickly, and energy released causes microexplosions in a process of thermo mechanical ablation. 13 The results of the dentin roughness caused by an Er,Cr:YSGG laser could be explicated because the dentin has three different types of tissue—intertubular, peritubular, and tubular—which contain different amounts of water. 9
Our morphological findings also showed an absence of carbonization, cracks, or condensation on root surfaces irradiated with an Er,Cr:YSGG laser. These results can be explained by the laser power level and irrigation water used during treatment. The power level of our laser was 1.0 W, used together with water, corroborating the results of Ting et al., 12 who observed no deleterious effects on root surfaces at this power level. Another study evaluated the effect of an Er,Cr:YSGG laser on human dentin, and disclosed cracks and condensation in dentin tissue. However, the lowest power level used in that study was 3.0 W, which explains the morphological advantages found in our study. 13 Yamazaki et al. 17 reported the presence of cracks in the dentin tissue after Er,Cr:YSGG laser irradiation. However, this was only found in groups without irrigation. Irrigation is important to avoid overheating during irradiation. However, increasing the amount of water has been associated with greater tissue ablation. 18 This could not be verified in our study because ablation is not effected by the water volume at an irradiation power of less than 1.5 W. 12
Although the effectiveness of calculus removal was not part of our study, calculus was not found on any the specimens, indicating the efficiency of this laser in removing these deposits. This was also considered beneficial in another study, where a root surface free of calculus was obtained using an Er,Cr:YSGG laser with 1.0 W power. 11 Moreover, specimens irradiated with an Er,Cr:YSGG laser showed evident dentin tubules and no smear layer. These effects may have influenced adhesion of blood components in G2 and G3 groups.
Analyzing the results on adhesion, G2 and G3 treated with Er,Cr:YSGG laser irradiation did not promote significantly greater adhesion of blood components than the G1 treated with hand instrumentation. Although no statistical differences were detected, it may be noted that G2 and G3 showed specimens without adhesion of blood components. This did not occur in G1 treated only with scaling and root planing. Theodoro et al. 2 demonstrated the same results when using a Er:YAG laser on dental roots. Studies evaluating the adhesion of fibroblasts found biocompatibility on roots affected by periodontal disease that were irradiated with an Er:YAG laser. 19,20 Although Maruyama et al. 21 reported less adhesion of fibroblasts on roots irradiated with the Er:YAG laser than for untreated roots, the difference in relation to our study is that the untreated roots had not been affected by periodontal disease. The literature surveyed did not disclose studies evaluating adhesion of fibroblasts on roots irradiated with an Er,Cr:YSGG laser.
The roughness produced on the root surfaces irradiated with laser may influence periodontal regeneration. 22,23 Some authors reported that smooth surfaces are not important for effective periodontal treatment, 24,25 although surface roughness may facilitate accumulation of bacterial biofilms. 16,20 However, the effect of quicker formation of biofilm is more important supragingivally than subgingivally. 15,26 Probably surfaces irradiated with an Er,Cr:YSGG laser had adhesion of blood components facilitated by physical retention due to root morphology. Eriksson et al. 27 demonstrated that neutrophil polymorphonuclear cells adhere preferably to rough surfaces in comparison to smooth surfaces. This may explain results of G2 and G3 treated with Er,Cr:YSGG laser in our study. Moreover, the absence of a smear layer and antimicrobial effects of an Er,Cr:YSGG laser may have influenced adhesion of these blood components.
Studies in vivo would be necessary to analyze the healing processes in tissues surrounding root surfaces irradiated by Er,Cr:YSGG laser. It should be noted that the healing process is very complex and that adhesion of the clot is only the initial event of the healing process.
Conclusion
Based on our results, it is concluded that Er,Cr:YSGG laser irradiation produced rougher root surfaces when compared to treatment by scaling and root planing. However, this did not affect adhesion of blood components to root surfaces.
Footnotes
Acknowledgments
This study had the financial support of the Coordination for the Improvement of Higher Educated Personnel (CAPES, Brasilia, DF, Brazil).
Author Disclosure Statement
No competing financial interests exist.