
Abstract
Introduction
Preventing and/or postponing muscle fatigue through light therapy is relatively new in the area of exercise physiology, and the optimal parameters in the use of this technique with such a purpose have not yet been determined. A pioneer study showed that low-level laser therapy (LLLT) can delay the inevitable decline in maximal tension during repeated electrically induced tetanic contractions in an animal model. 7 Also, specific doses of LLLT reduced muscle damage when compared with that in non-irradiated groups. 7 Subsequent human model studies showed that professional male volleyball athletes subjected to repeated voluntary movements of elbow flexion–extension using free weights produced a significant higher number of repetitions when previously irradiated with red (655-nm) LLLT, 8 and infrared (830-nm) LLLT. 9 In both trials, no difference on blood lactate levels after exercise between LLLT and placebo treatment was observed.
A possible limitation of these experimental studies 8,9 is related to the single laser probes used to administer LLLT. This kind of probe allows the irradiation of a small muscle area per irradiation, leading to an increased irradiation time to reach the entire muscle. Therefore, when one seeks to reduce or postpone fatigue by using light therapy, a larger irradiation area would be more effective, as was shown in another study using volleyball athletes that had positive results in exercise performance, blood lactate concentration, and muscle damage with a multidiode cluster probe. 10 This apparatus, which has been available on the market for two decades, typically has several visible red and infrared light-emitting diodes (LEDs). LEDs are cheaper to manufacture and have larger spot sizes than laser diodes. Also, it appears that therapeutic effects ascribed to monochromatic light relate more to wavelength and dose than to the light source. 11
Although this experimental protocol was designed to evaluate the athletes' muscle fatigue, the angular velocity was not controlled during the elbow flexion–extensions. The angular velocity (or the muscle-shortening velocity) is an important variable affecting muscle force production, as described by the force–velocity relation, 12 affecting muscle fatigue. For this reason, isokinetic dynamometers are considered the gold-standard equipment to measure muscle performance and consequently muscle fatigue. 13 Commonly, the mechanical quantification of fatigue is determined by comparing the maximal isometric voluntary contractions (MVCs) performed before and after a given exercise test in these dynamometers. 4 To the best of our knowledge, only one pilot study used an isokinetic dynamometer to evaluate the LLLT effects on quadriceps muscle fatigue induced by electrical stimulation in five healthy volunteers. These preliminary results showed no differences in knee-extensor torque production between LLLT and control situations, 14 suggesting that LLLT is unable to decrease muscle fatigue.
Therefore, the purpose of this study was to evaluate the effects of LEDT on muscle fatigue by using an LED multidiode cluster probe before an isokinetic concentric knee flexion–extension fatigue protocol.
Materials and Methods
Ethical aspects
The study was approved by the Ethics Committee of the Federal University of Rio Grande do Sul. All subjects signed an informed-consent form before participating in the study.
Sample
Sample size was determined based on the following aspects: similar sample size to the one used in studies with a similar isokinetic fatigue protocol (e.g., Pincivero et al., 15 who demonstrated high intraclass correlation coefficients between test and retest in 21 subjects); and based on the fact that most experiments conducted with humans involving light therapy and fatigue have used samples with five to 12 participants. 8 –10,14 Therefore, a total of 20 subjects was initially determined. These subjects were included according to the following criteria: (a) male volunteers between 18 and 35 years old; (b) healthy and physically active subjects (exercising at least 3 times per week); (c) without any lower-limb musculoskeletal injury within a period of 30 days before the tests; and (d) able to perform the fatigue test in such a way that they reach maximal peak torque by the fifth repetition with progressive decrease in peak torque with subsequent repetitions.
Experimental design
The study was designed as a crossover, randomized, double-blind, and placebo-controlled trial. Before data acquisition volunteers were randomized by using a simple drawing of lots (A and B). For participants in the lot A, LEDT was given at the first session, and placebo treatment was given at the second session. The inverse order was used for participants in lot B. All participants were crossed over during the experiment, to compare the outcomes after LEDT and placebo treatments, respectively.
The group allocation code from the drawing of lots was performed by a technician who set the control unit accordingly to either an LEDT or a placebo mode. This technician was instructed not to communicate the type of treatment given to either the participants or the researchers responsible for the dynamometer data collection. The volunteers used opaque goggles during the therapy to protect their eyes from the treatment and to help in the blindness of the study. For the same reason, researchers were not present in the dynamometer room during LEDT or placebo treatments. Thus, the treatment allocation was concealed from participants and researchers.
The experiment followed a 2-day protocol with a minimum of a 72-h interval between testing sessions. The volunteers were submitted to the same evaluation protocol in these two sessions.
Protocol
Information regarding procedures and exercise tests was given, and any questions were answered before the testing protocol. All subjects performed a warm up on a cycle ergometer for 5 min (mean cadence of 80 rpm and load established by the volunteer). After the warm up, the subject was properly positioned with the dominant lower limb on the Isokinetic Dinamometer Biodex System 3 Pro (Biodex Medical System, Shirley, NY), following the recommendations of the manufacturer for evaluations of knee flexion–extension movement.
In the first part of the protocol, the knee-extensor maximal peak torque was determined. Three knee-extensor maximal isometric voluntary contractions (MVCs) were performed at the knee-joint angle of 60 degrees (0 degrees = total knee extension). Each MVC lasted 5 sec, and 2-min intervals were observed between consecutive contractions. Subjects were verbally encouraged during MVCs to obtain maximal effort. The highest isometric peak torque value obtained among the three MVCs was considered the maximal isometric voluntary knee-extensor contraction before exercise (PRE-MVC).
PRE-MVC was followed by a resting period of 60 sec, after which volunteers performed a familiarization isokinetic protocol. This protocol consisted of five submaximal voluntary repetitions of knee flexion–extension in concentric mode at an angular velocity of 180 degrees per second, with a 90-degree total range of motion (ROM). After familiarization, subjects rested for 5 min before the fatigue protocol. During this period, LEDT or placebo treatment was conducted (see LEDT application and parameters).
Two minutes after LEDT or placebo application, the fatigue protocol started. This protocol consisted of 30 maximal isokinetic concentric repetitions of knee flexion–extension performed at an angular velocity of 180 degrees per second with a 90-degree ROM. 15 All participants were instructed to perform the exercise with the highest intensity possible from the first repetition, and verbal encouragement was given to the subjects throughout the fatigue protocol.
After completion of the fatigue protocol, the dynamometer automatically positioned the lower limb at a knee-joint angle of 60 degrees, and a new 5-sec knee-extensor MVC was performed, approximately 10 sec after exercise finish. The peak torque value was considered the maximal isometric voluntary knee-extensors contraction after exercise (POST-MVC).
An experimental protocol flow chart is presented in Fig. 1.
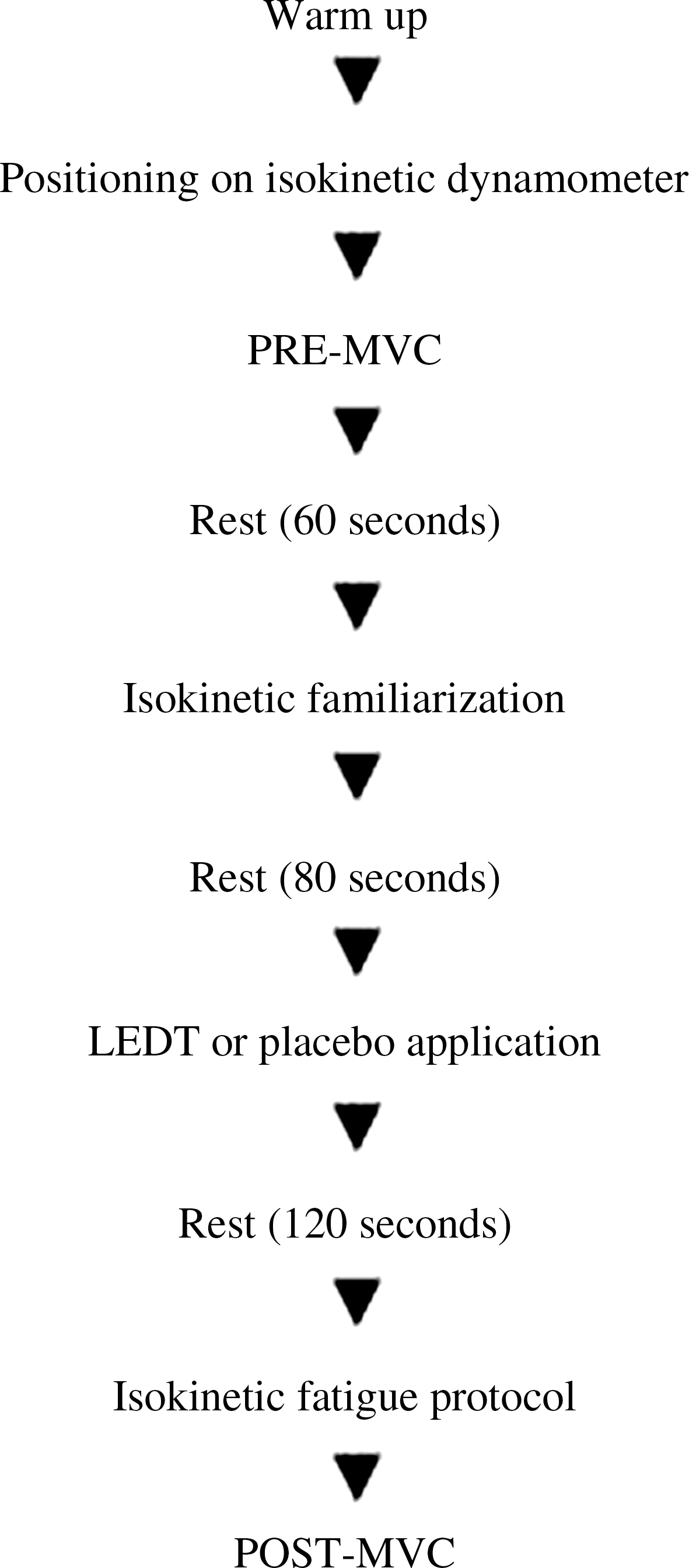
Flow chart illustrating subjects' progression through the protocol.
LEDT application and parameters
During all trials, participants received a single treatment (LEDT or placebo, according to the results of the randomization procedure) through a Thor DD2 Control Unit (Thor®; London, England) with a LED multidiode cluster probe (with 34 diodes of 660 nm and 35 diodes of 850 nm) of the same manufacturer.
LEDT parameters were similar to those used by Leal Junior et al. 16 : 30 sec per point, except that three application points were used instead of two, with the aim of irradiating a larger quadriceps area. The central belly of the rectus femoris, as well as the most prominent point of the vastus medialis and vastus lateralis muscles, was defined by palpation and marked for LEDT or placebo irradiation. The application started 80 sec after the end of the familiarization protocol and finished 120 sec before the fatigue protocol, with a total irradiation time of 30 sec per point. Between each application point, a 5-sec period was necessary to correct the cluster-probe position. The placebo application was exactly the same as the LEDT, but with the device turned off. Fig. 2 shows the LEDT or placebo application points, and Table 1 presents the parameters used during LEDT treatment.

Application points (black circles) used for LEDT or placebo treatment.
Statistical analysis
From the isokinetic fatigue protocol, the following parameters were obtained for analysis: Peak Torque, defined as the maximal knee-extensor torque value obtained during the fatigue test, always reached between first and fifth repetition (expressed in Newton-meters); Average Peak Torque, the mean value calculated by the peak torque reached in each repetition of the fatigue test (in Newton-meters); Average Power, the mean value calculated by the power reached in each repetition of fatigue test (in Watts); Total Work, the sum of work performed in each repetition of fatigue test (in Joules); and Work Fatigue Index, defined as a percentage decline in work performed and calculated by the division of the work performed during the last one third of the fatigue test (last 10 repetitions) by the work performed during the first one third (first 10 repetitions). Comparison between LEDT and placebo conditions was analyzed by using a paired two-sided Student's t test.
The absolute torque values obtained in the MVCs were compared by using a two-way ANOVA followed by a Holm-Sidak post hoc test to determine differences between PRE-MVC and POST-MVC after LEDT and placebo treatments. All statistical comparisons were performed by using a significance level set at 5%.
Results
After data collection, three volunteers had to be excluded from the sample: one subject could not perform the second session because of a musculoskeletal injury (inclusion criterion c), and two subjects did not have a satisfactory performance during the isokinetic fatigue protocol in any of the two testing sessions (inclusion criterion d). Therefore, the final sample was composed of 17 volunteers (26.29 ± 4.33 years; 75.24 ± 6.34 kg; and 1.78 ± 0.05 m).
No differences were observed for all performance variables of the knee-extensor muscles in the isokinetic fatigue protocol between LEDT and placebo treatments (Table 2). No difference was found (p = 0.675) in PRE-MVC torque values between LEDT (284.81 ± 54.52 Nm) and placebo (282.65 ± 53.64 Nm) treatments. The isokinetic fatigue protocol led to a decrease (p < 0.001) in maximal isometric torque after both LEDT and placebo treatments. However, higher torque values (p = 0.034) were observed in POST-MVC for LEDT (237.68 ± 48.82 Nm) compared with placebo (225.68 ± 44.14 Nm) treatment (Fig. 3).
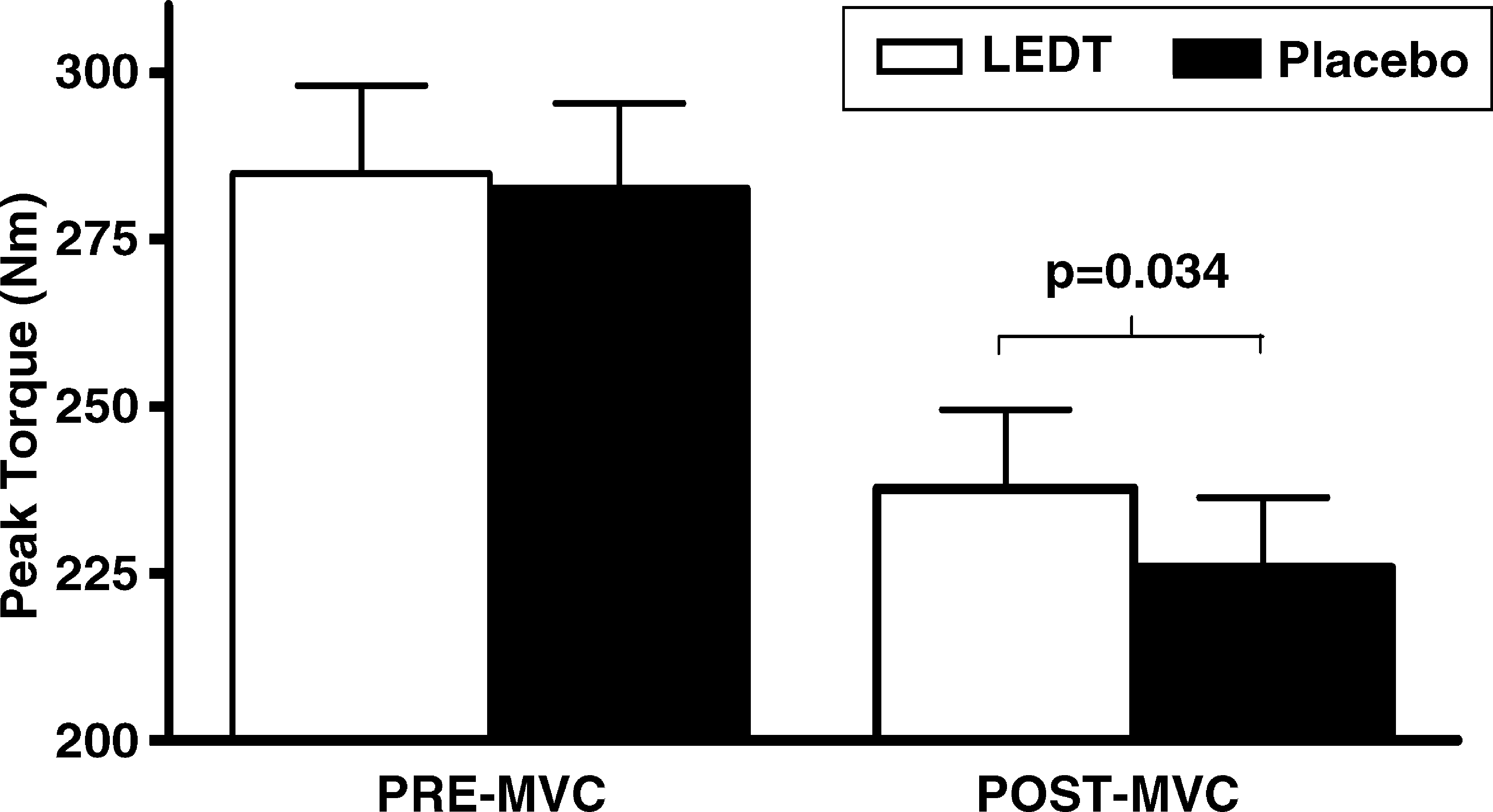
PRE-MVC and POST-MVC knee-extensor maximal isometric torques for LEDT and placebo treatments (mean ± SEM). The bracket indicates differences in POST-MVC between LEDT and placebo (p value above the bracket).
Discussion
The similarity in the isokinetic results of knee extensors during the two sessions of the fatigue protocol (Table 2) demonstrated that the volunteers' performance was very similar between tests (i.e., the crossover design was justified and worked to reduce any effect of bias or learning that may have occurred between the first and second sessions). Also, the similarity in maximal isometric torque between LEDT and placebo conditions during PRE-MVC (Fig. 3) demonstrated that subjects had the same capacity for force production at the initial moment of both testing sessions. In other words, subjects came for the two sessions with similar maximal isometric torque capacities and performed both tests with similar intensity. Therefore, any differences found in POST-MVC values cannot be attributed to possible preexistent differences in the two experimental conditions.
The difference in POST-MVC values between placebo and LEDT treatments shows that an effect of LEDT treatment was present on maximal isometric knee-extensor torque. More specifically, the fact that POST-MVC in the placebo condition was smaller than in the LEDT is evidence of preservation of the maximal capacity for torque generation by LEDT irradiation. Whereas in the LEDT condition, the ability to generate isometric torque decreased on average by ∼16%, in the placebo condition, it decreased ∼20%. This further demonstrates that the application of LEDT before the isokinetic fatigue protocol improves the isometric performance after exercise. These results are in agreement with previous studies that tried to prevent fatigue by using LLLT 7 –9 and LEDT. 10
The use of light therapy to prevent muscle fatigue was first reported by Lopes-Martins et al. 7 These authors performed electrically elicited repetitive tetanic contractions in the tibialis anterior muscle of rats previously irradiated with different doses of LLLT (0.5 J/cm2, 1.0 J/cm2, 2.5 J/cm2, and control) by using a visible red laser (655 nm) and a continuous power output of 2.5 mW. This study demonstrated that LLLT could delay the inevitable decline in maximal peak force due to fatigue during repeated contractions. In addition, specific doses of LLLT reduced muscle damage, measured by creatine kinase levels.
By using the same visible red laser (655 nm) of the previously mentioned animal study, Leal Junior et al. 8 applied 5 J in each of four points along the ventral side of the biceps humeri muscle belly (50 mW of power output; 20 J of total energy delivered) of 12 male professional volleyball players, subjected to repetitive voluntary elbow flexion–extension movements by using free weights. A significant increase was observed in the total number of repetitions performed after LLLT treatment, despite the fact that the increase of blood lactate levels did not differ from the control situation. In a subsequent experiment, 9 authors found similar results by using the same fatigue protocol to measure the effects of an infrared laser (830 nm, 100 mW, and 5 J, delivered at four points on the muscle belly, also 20 J of total energy) delivered on the biceps muscle.
Recently, this experimental model was used in a third experiment, 10 now using the same multidiode cluster probe of the present study (660/850 nm; 10/30 mW; 41.7 J of total energy irradiated). The results demonstrated again the positive effects on performance, as well as a minor increment in blood lactate concentration and a protective effect of LEDT on muscle damage (measured by creatine kinase levels), similar to that shown in another study involving high-intensity cycle-ergometer exercise. 16 These findings corroborate an idea defended by Enwemeka 11 that therapeutic effects of monochromatic light relate more to wavelength (range of 600–1,000 nm) and doses than to the source of light (laser or LED, for example).
To the best of our knowledge, only one published pilot study involved light-therapy application using an isokinetic dynamometer to evaluate fatigue. 14 Five volunteers had fatigue induced in their quadriceps muscles by repeated electrical stimulation. The authors opted to use a scanner laser (808 nm, 500 mW) that irradiated the quadriceps muscle during 5 and 10 min, applying the respective dosages of 3 J and 7 J. Their results showed no differences in peak torque decrement between LLLT and control situations. Their absence of laser effects on electrically elicited torques might be related to the laser parameters used. More specifically, their delivered dosage was considerably lower than that used in the present study. Also, the scanner application method leads to a possible insufficient interaction time between laser and skeletal muscle tissue. The noncontact between skin and apparatus may have promoted a higher reflection of the irradiated energy, and consequently, less laser penetrated into the skin and muscle.
The likely mechanism that explains the prevention of muscle fatigue after light therapy is in the light–tissue interaction properties and the phenomena generate by this interaction, especially on blood circulation and cellular mitochondria.
It is well known that laser promotes arteriolar vasodilation and improves the peripheral microcirculation. 17,18 Consequently, an increase occurs in the muscle's blood supply, thereby increasing the oxygen supply to the tissue. Probably it provides better conditions to perform activities using the aerobic system and reduces the blood lactate accumulation, as observed by Leal Junior et al. 10 by using the same LEDT apparatus of the present study, although other studies 8,9 observed no effect of laser therapy in blood lactate accumulation after exercise.
The interaction between laser and mitochondria has been the focus of many studies, which observed a stimulatory effect that promotes an increment in mitochondrial capacity to generate adenosine triphosphate (ATP). 19 –21 Manteifel et al. 22 observed, through three-dimensional analysis of human lymphocytes, the presence of giant mitochondria after laser irradiation, able to produce higher levels of ATP concentration. Studies in animal models also have shown laser effectiveness on oxidative stress to decrease. 23,24 This phenomenon consists of serial damage to the organism caused by imbalance between prooxidant and antioxidant agents, which may be due to an increase in the production of reactive oxygen species (ROS) or a decrease of cellular antioxidant capacity 25 that is closely related to a reduction in muscle performance. 26,27 In an experiment involving electrical stimulation of rat muscle cells in culture, Xu et al. 28 verified that laser treatment significantly decreased ROS production and restored the mitochondrial function. These authors suggested that light therapy is an innovative and noninvasive treatment in prevention of exercise-induced muscle fatigue, muscle damage, and other processes where mitochondrial function has a key role. This evidence supports the hypothesis that the key point to explain muscle-fatigue prevention by light therapy is at the mitochondrial level, especially related to an increase in the ATP synthesis and to a decrease in ROS production.
Although our results show evidence of a reduction in knee-extensor fatigue after LEDT, caution should be taken about the generalization of these findings. An interesting observation is that three of 17 participants did not show an increment in performance with LEDT treatment. It is possible that external factors, not related to LEDT or placebo administration, contributed to these results. An individual response to this type of therapy cannot be ignored. The monitoring of some biochemical markers of muscle function, such as blood lactate and creatine kinase levels, might help future studies to determine better the effects of LEDT in human muscle function. A more rigorous control of the volunteers' physical activities between sessions and a preliminary familiarization session on a separate day to train the subjects with the isokinetic fatigue protocol are some of the aspects that should be controlled in future studies.
In summary, LEDT was able to promote a smaller decrease in isometric torque after an isokinetic high-intensity concentric fatigue protocol. These findings reinforce the effectiveness of light therapies on muscle-fatigue prevention. Our results are novel in the area of light therapy and performance because they demonstrated for the first time the preventive effects of LEDT on muscle fatigue by using the most reliable apparatus to evaluate muscle function in humans.
Footnotes
Acknowledgment
Professor Ernesto Cesar Pinto Leal Junior would like to thank Fundo de Apoio a Pesquisa–FAP/UNINOVE for financial support.
Author Disclosure Statement
No competing financial interests exist.