
Abstract
Introduction
Matrix metalloproteases (MMPs) are a family of zinc- and calcium-dependent endopeptidases that can degrade almost all molecules in the cutaneous extracellular matrix (ECM), such as structural molecules of collagen and elastic fibers. 4 –7 Tissue inhibitor of metalloproteinase 1 (TIMP-1) is one of the endogenous inhibiters that binds to activated interstitial collagenase and gelatinase. 8 UV radiation has been recognized as a modulator of MMPs both in vitro and in vivo, and there is extensive evidence linking skin photoaging with the effects of MMPs. 1,9,10
Intense pulsed light (IPL) is one of the nonablative approaches to treating photoaging. The lower risk of postinflammatory hyperpigmentation and the limited postoperative downtime have made IPL a popular choice. Histological studies revealed accumulation of procollagen I and procollagen III after IPL treatment. 11,12 Recent studies demonstrated decreased MMP expression levels following IPL irradiation, suggesting that IPL irradiation may reduce the destructive aspects through down-regulation of MMPs and result in ECM accumulation. 13,14 Increased MMP-1 and TIMP-1 protein levels have been reported in IPL-irradiated rat skin. 15,16 However, the real expression pattern of MMPs/TIMP-1 and their role in IPL irradiation remain unknown.
This study focused on the effects of IPL on the expression of MMP-1, -3, -9, and -12; TIMP-1; and ECM. The MMPs/TIMP-1 and ECM expression patterns between IPL- and UVA-irradiated skin were compared and the role of MMP in IPL photorejuvenation was investigated.
Materials and Methods
Research volunteers
The work protocol was granted by human experimentation committee of the hospital in accordance with the Helsinki Declaration. Before the experiments, informed consent was obtained in writing from all subjects. Eleven healthy female volunteers with Fitzpatrick skin phototype III participated in this study (mean age 39 ± 5 y). The subjects had no history of previous skin disease, were taking no photosensitizing drugs, and had never exposed buttock skin to direct sunlight. Buttock skin was examined to confirm the absence of any skin lesions that could interfere with the investigation.
UVA and IPL irradiation
Skin samples were divided into three groups: IPL-irradiated skin, UVA-exposed skin (to induce a skin photoaging model), and normal control skin. Multiport solar simulators GS-2004 (Aohua Co.) were used in the construction of skin photoaging model. The solar simulator consisted of a 450-W xenon lamp and a dichroic mirror. Radiation was filtered to deliver a continuous UV spectrum from 320 to 400 nm (UVAII/UVAI = 8–20%) by a WG 320, 1-mm-thick, short cut-off filter plus a UG 11, 1-mm-thick, long cutoff filter (Schott). The irradiances at skin level were monitored with a calibrated SUN5 digital spectroradiometer (National Institute of Measuring). Before experiments, the minimal erythema dose was determined on one side of the buttock. The skin was irradiated by UVA three times per week (Monday, Wednesday, and Friday) for 13 weeks. The initial UVA dose was 8.3 J/cm2 and increased each week with 20% progression. Thus a total dose of 1070 J/cm2 was implemented in the irradiation, which can produce histological changes of skin aging. 17 Three days after the last exposure, 4-mm punch biopsies were obtained from the irradiated and control sites. Specimens were frozen (−70°C) for real-time quantitative polymerase chain reaction (qRT-PCR) and fixed by formalin for immunochemistry.
To emulate the clinical IPL photorejuvenation process, skin was smeared with cooled ultrasonic gel and then irradiated by IPL (Lovely II, Alma) with the following specifications: wavelength 570–950 nm, spot size 8 × 35 mm, pulse duration 12 msec, pulse delay 30 msec, fluence 15 J/cm2, two pulses. Each individual was given four irradiations at 2-week intervals. Two weeks after the last IPL irradiation, the skin specimens were taken.
Routine histology
The specimens were 4 mm in width, embedded in paraffin wax, and sectioned on a rotary microtome (Leica) at 6 μm; four sequential sections for each paraffin block were taken. Elastic fibers were stained by Weigert's Resorcin Fuchsin method (26370-Series, Electron Microscopy Sciences) according to the instructions. Elastic fibers were stained dark blue and collagen fibers were stained red pink.
Immunohistochemical staining for expression of MMPs, TIMP-1
Immunohistochemical staining was performed using the primary antibodies MMP-1 (dilution 1:50, RB-1536; NeoMarkers), MMP-3 (dilution 1:50, RB-10488, NeoMarkers), MMP-9 (dilution 1:50, RB-9234, NeoMarkers), MMP-12 (dilution 1:50, EP1261Y 1906-1, Epitomics), TIMP-1 (dilution 1:100, ZA-0429, ZYMED), collagen I (dilution 1:400, AB-3391, Chemicon), and collagen III (dilution, 1:50, ZM-0465, ZYMED). MMPs/TIMP-1 antigen retrieval was carried out by treating tissue sections with boiled citrate acid. Collagen I and collagen III antigens were retrieved by pepsin. Negative controls were treated by substitution of the primary antibody with rabbit preimmune serum (for rabbit polyclonal) and mouse immunoglobulin (for mouse monoclonal). Tissues of breast cancer or placenta known to express MMPs/TIMP-1 were used as positive controls. 3-Amino-9-ethylcarbozole was used as the chromogenic agent, and hematoxylin was used to counterstain the nucleus.
Image analysis
Image Pro Plus 6.0 image analysis software (Media Cybernetics) was used to measure the integral optical density of MMPs/TIMP-1 and area density of collagen/elastic fibers. Image analysis was done by two pathologists with no knowledge of the treatments. In this study, three serial tissue sections for each antibody were taken and five fields of view per section were analyzed. Epidermis and epidermal appendages were excluded from the fields for area density measurement. To analyze the integral optical density, sections were divided into epidermis and dermis.
RNA analysis
Total RNA was harvested with High Pure tissue RNA Isolation Kit (Biomed) and quantified by measurement of optical density of an aliquot at 260 and 280 nm, using a DU-65 spectrophotometer (Beckman Instruments). Contaminating genomic DNA was removed by incubation with DNAase I Amplification Grade (Invitrogen). Two micrograms total RNA was used for cDNA synthesis using Superscript™ III First-Strand synthesis system (Invitrogen). Amplification of cDNA was made using SYBR Green PCR Master Mix in an Applied Biosystems 7500 Real-time PCR System under standard conditions. To control for variations in the reactions, all polymerase chain reactions (PCRs) were normalized against glyceraldehyde-3-phosphate dehydrogenase (GAPDH) expression and analyzed in duplicate. The standard curve was calculated by plotting the threshold cycle (Ct). A linear regression was performed, and the slope-relating Ct to log RNA was calculated. The average Ct for each sample was then used to determine the corresponding log nanogram of standard RNA using the slope of the standard curve. Primers were all synthesized by Shanghai Invitrogen Biotechnology. Sequences of primers and PCR cycling conditions are showed in Table 1. The PCR program consisted of pre-denaturation at 95°C for 3 min and denaturation at 95°C for 10 sec for MMP-1, -3, -9, and -12 and TIMP-1, denaturation at 94°C for 1 min for collagens I and III, and at 94°C for 20 sec for elastin. The PCRs were performed in 40 cycles for MMP-1, -3, -9, and -12 and TIMP-1, 35 cycles for collagens I and III, and 25 cycles for elastin. Baseline mRNA levels of control skin were assigned a value of 1, and fold change above baseline was measured and expressed as mean ± standard deviation.
MMP, matrix metalloprotease; TIMP-1, tissue inhibitor of metalloproteinase 1; GAPDH, glyceraldehyde-3-phosphate dehydrogenase; COLL, collagen.
Statistical analysis
Protein/mRNA levels of MMPs/TIMP-1 and collagen/elastic fibers were analyzed by SPSS 15.0 software (SPSS). One-way analysis of variance (ANOVA) was used to compare the quantitative data (when a normal distribution was found) and Kruskal–Wallis one-way ANOVA on ranks was used if distributions were not normal. The differences were considered statistically significant at p < 0.05 among the groups: IPL-irradiated skin, UVA-exposed skin, and control skin.
Results
Effect of IPL irradiation on epidermis and dermal matrix proteins
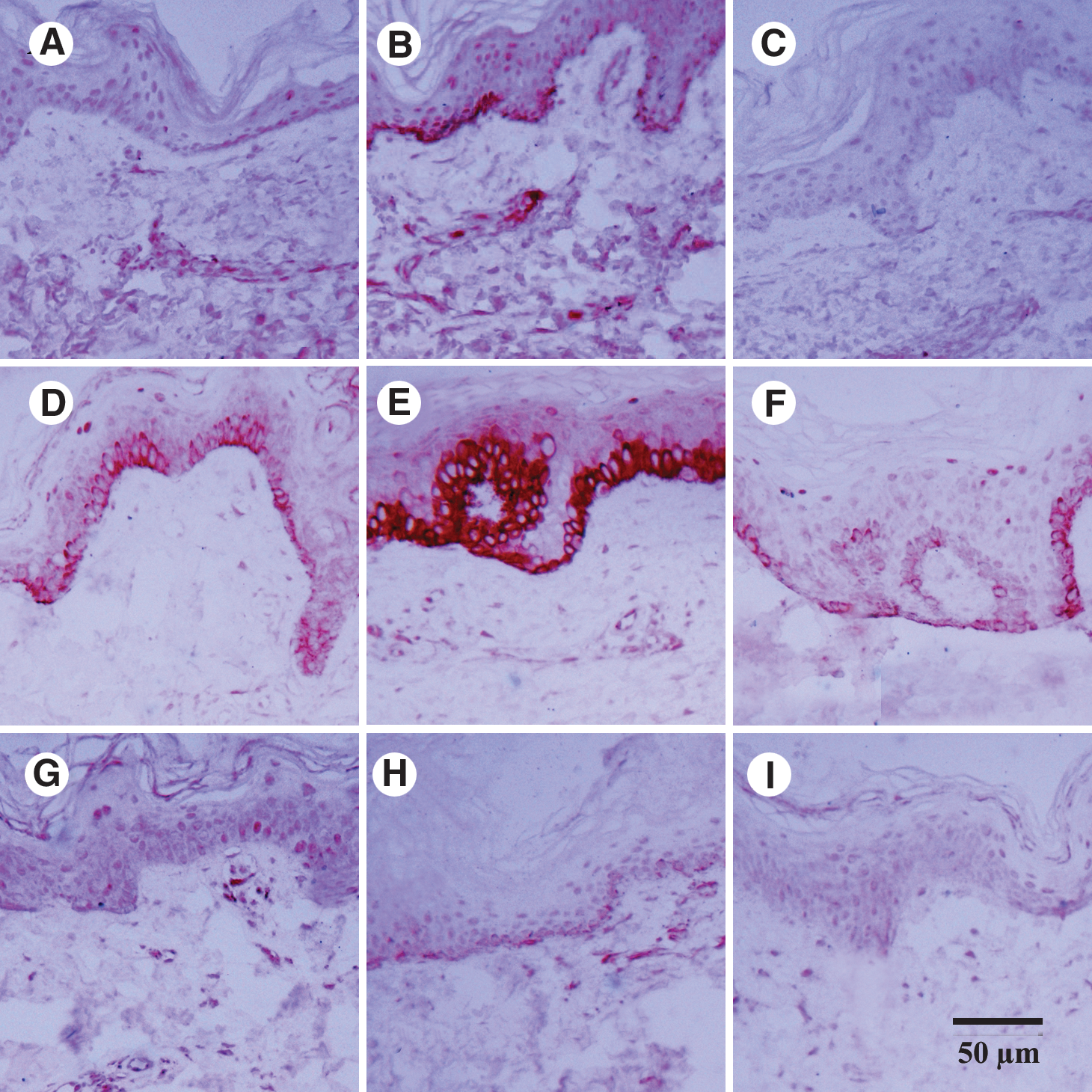
Both IPL and UVA irradiation caused an increase in the thickness of epidermis and stratum corneum, particularly the thickness of stratum corneum (data not shown). By Weigert's staining, no morphological change of elastic fibers was found in IPL-irradiated skin (Fig. 1A). However, fragments of elastic fibers were detected in dermal papilla in UVA-exposed skin (Fig. 1B), which confirmed the establishment of a skin photoaging model. There was no significant difference in the area density of elastic fibers between IPL- and UVA-irradiated skin and the control (0.11 ± 0.02, 0.13 ± 0.04, 0.12 ± 0.03; p > 0.05, p > 0.05; Table 2).

Photomicrographs of samples stained with Weigert's solution (A–C), collagen I antibodies (D–F), and collagen III antibodies (G–I).
IOD, integral optical density; AD, area density. AD was calculated by measurement of the ratio between area of collagen/elastic fibers and area of dermis, using Image Pro Plus 6.0.
Immunohistochemistry showed more compactly arranged collagen I fibers and smaller interspaces in IPL-treated skin (Fig. 1D) than the control (Fig. 1F). There was a significant increase in the area density of collagen I fibers in IPL-irradiated skin (0.86 ± 0.15) as compared with the control (0.79 ± 0.09; p < 0.05; Table 2). On the contrary, UVA caused a decrease in the area density of collagen I fibers (0.70 ± 0.13; p < 0.05). Collagen III staining revealed similar arrangement of collagen III fibers in IPL- and UVA-irradiated skin (Fig. 1G and H) as compared with the control (Fig. 1I). There was no significant difference in area density of collagen III fibers between IPL- and UVA-irradiated skin and the control (0.82 ± 0.10, 0.81 ± 0.12, 0.83 ± 0.06, respectively; p > 0.05, p > 0.05, Table 2).
Effects of IPL and UVA on protein expression of MMPs/TIMP-1
Immunohistochemical staining showed increased MMP-1, -3, and -9 protein levels in IPL-irradiated (Fig. 2A, D, and G) and UVA-irradiated skin (Fig. 2B, E, and H), as compared with the normal control (Fig. 2C, F, and I). Image analysis software was used to quantify the dermal and epidermal MMPs/TIMP-1 expression by measuring their integral optical density. Compared with dermal MMP-1, -3, -12, and MMP-9 levels in the control skin (7.34 ± 1.21, 4.53 ± 0.68, 4.66 ± 0.51, 11.50 ± 1.78, respectively), IPL irradiation induced significantly higher levels of MMP-1, -3, and -12 (39.25 ± 4.24, 7.21 ± 0.97, 8.60 ± 0.9) and MMP-9 (25.36 ± 3.06) (p < 0.01, p < 0.01, p < 0.01, p < 0.01) in the dermis. While, UVA induced much higher levels of dermal MMP-1, -3, and -12 (58.31 ± 7.39, 14.03 ± 0.76, 67.05 ± 8.63) and lower level of MMP-9 (19.58 ± 2.22) than IPL (p < 0.01, p < 0.01, p < 0.01, p < 0.05). There was a significant difference in the dermal MMP-9 protein levels between IPL- and UVA-irradiated skin (25.36 ± 3.06, 19.58 ± 2.22, respectively; p < 0.05). These findings indicated that IPL may have a more powerful effect on MMP-9 expression. Compared with the normal control (6.50 ± 0.57), the elevation of the dermal TIMP-1 level in IPL-irradiated (19.58 ± 3.05) and UVA-irradiated skin (17.70 ± 2.24) was statistically significant (p < 0.05), whereas there was no significant difference in the TIMP-1 levels between IPL- and UVA-irradiated skin (p > 0.05).
Photomicrographs of samples stained with MMP-1 (A–C), MMP-3 (D–F), and MMP-9 antibodies (G–I).
IPL and UVA also increased the epidermal MMPs/TIMP-1 protein expression. As compared with the control (18.22 ± 3.01, 62.86 ± 5.23, 61.35 ± 8.41, 12.44 ± 2.17, 7.40 ± 0.89), there were significantly higher levels of epidermal MMP-1, -3, -9, and -12 and TIMP-1 in IPL-irradiated (22.40 ± 8.16, 79.34 ± 10.25, 95.24 ± 11.09, 18.50 ± 2.35, 25.90 ± 4.37) and UVA-irradiated skin (166.31 ± 14.35, 188.39 ± 20.77, 76.29 ± 9.53, 102.09 ± 15.11, 27.80 ± 3.26) (p < 0.01, p < 0.01, p < 0.01, p < 0.01, p < 0.01) (Table 2).
Effect of IPL and UVA on collagen/elastin and MMPs/TIMP-1 mRNA expression
From the mRNA level of MMPs/TIMP-1 related to that of GAPDH, a modulation tendency similar to the immunohistochemical MMP changes was observed. Because the baseline mRNA level of the control skin was assigned a value of 1, there was a significant increase in mRNA levels of collagen I in IPL-irradiated skin (3.20 ± 0.21 fold, p < 0.05), but there was no significant difference in collagen I mRNA levels between UVA-exposed skin and the control (1.02 ± 0.13 fold, p > 0.05) (Fig. 3). Collagen III and elastin mRNA levels in IPL-irradiated (1.24 ± 0.35 fold, 1.13 ± 0.21 fold) and UVA-irradiated skin (1.07 ± 0.25 fold, 0.97 ± 0.16 fold) showed no significant difference as compared with the control (p > 0.05, p > 0.05).
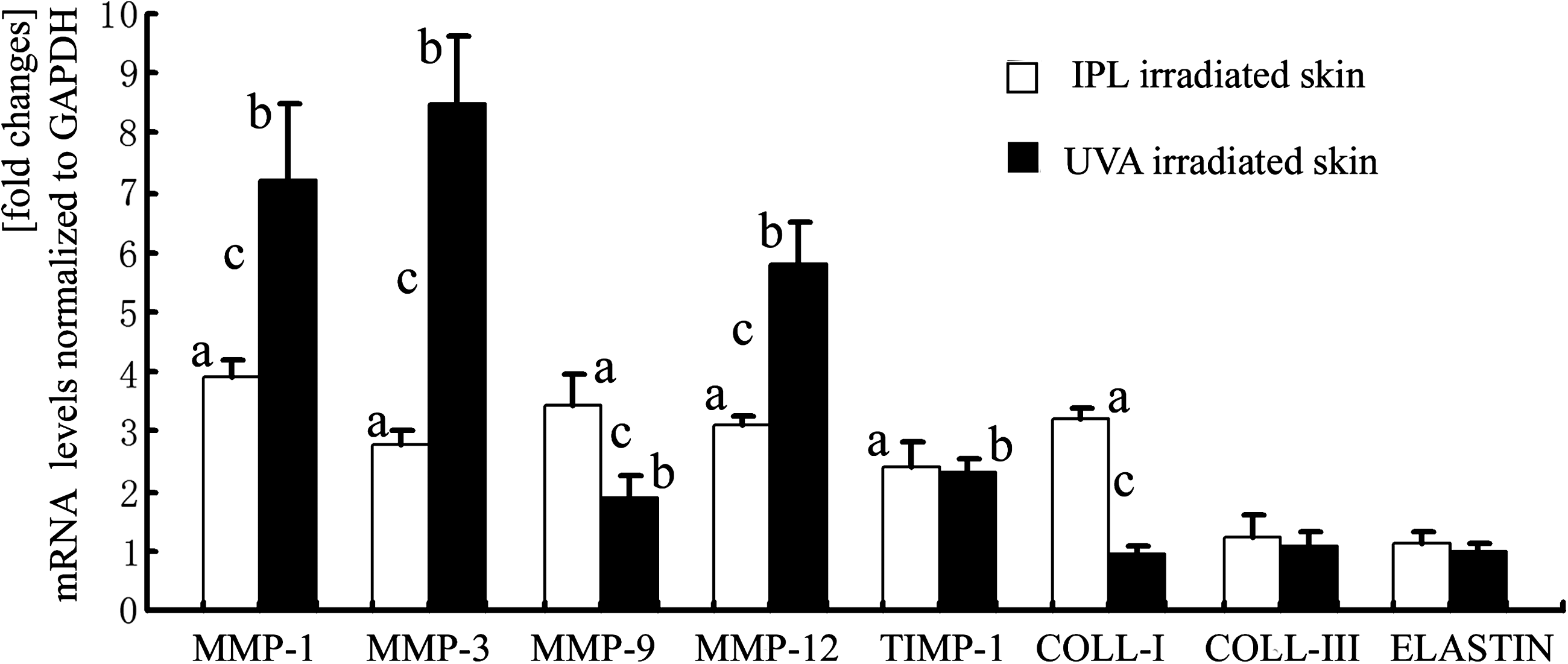
MMPs/TIMP-1, collagen and elastin mRNA levels in IPL- and UVA-irradiated skin. MMPs/TIMP-1, collagen and elastin mRNA levels were normalized against glyceraldehyde-3-phosphate dehydrogenase (GAPDH) expression. Baseline mRNA levels of control skin were assigned a value of 1, and fold changes above baseline was presented as mean ± standard deviation. a p < 0.05 IPL-irradiated skin versus normal control skin; b p < 0.05 UVA exposed-skin versus normal control skin; c p < 0.05 UVA-exposed skin versus IPL-irradiated skin.
There were significant MMP-1, −3, and −12 mRNA increases in IPL-irradiated skin (3.91 ± 0.29, 2.80 ± 0.24, 3.1 ± 0.14 fold) (p < 0.05, p < 0.05, p < 0.05). In UVA-exposed skin, MMP-1, -3, and -12 mRNA levels were significantly increased (7.23 ± 1.27, 8.51 ± 1.13, 5.80 ± 0.69 fold) (p < 0.01, p < 0.01, p < 0.01). Notably, IPL-irradiated skin led to a significant increase in MMP-9 mRNA level (3.44 ± 0.52 fold), more remarkable than that in UVA-exposed skin (1.92 ± 0.35 fold). Compared with that of the control skin, TIMP-1 mRNA levels significantly increased in both UVA-irradiated (2.42 ± 0.41 fold) and IPL-irradiated skin (2.31 ± 0.26 fold), while there was no significant difference in the TIMP-1 mRNA levels between UVA- and IPL-irradiated skin (p > 0.05) (Fig. 3).
Discussion
To gain further insight into the effects of IPL and UVA radiation on MMPs/TIMP-1 expression and ECM metabolism, their expression patterns were studied by histochemistry, immunohistochemistry, image analysis, and qRT-PCR.
As a nonablative approach to photoaging, IPL causes controlled thermal damage to the connective tissue that induces local skin regeneration, which is the basis of the skin photorejuvenation phenomenon. 11 Moreover, it is known that skin regeneration is characterized by a dynamic balance between ECM synthesis and destruction. Scant investigation has been focused on the effects of IPL on MMP expression, an important modulator in ECM synthesis and destruction. Wang et al. 15,16 reported up-regulation of MMP-1 and TIMP-1 protein levels in IPL-treated rat skin and assumed that up-regulation of MMPs induced by IPL may play a role in collagen regeneration. Other studies have also reported increased MMP-1 and TIMP-2 mRNA levels in low-level laser irradiated porcine aortic smooth muscle cells and carbon dioxide laser treated human skin. 18,19 In this study, general elevation of MMP-1, -3, -9, and -12 and TIMP-1 associated with collagen up-regulation was observed in IPL-irradiated skin, agreeing with these results. All these findings demonstrated that photorejuvenation treatments such as IPL irradiation are often accompanied by MMPs/TIMP-1 increase, which may result in a dynamic repair process.
Studies concerning the relation of UV radiation and MMP expression have been widely reported. In this study, MMP-1, -3, -9, and -12 and TIMP-1 expression levels were significantly increased in UVA-exposed skin, which is consistent with previous studies. 1,20 It seems paradoxical that IPL and UVA induced similar MMPs/TIMP-1 elevation but opposite clinicopathologic changes: photoaging and photorejuvenation.
Different MMPs have different substrate specificity for dermal components. 4,5 For example, collagenase-1 initially clears intact collagen I. Stromelysin-1 (MMP-3) cleaves dermal fibrillar collagens (I, III, and V) and participates in the activation of proMMP-1 and proMMP-9. MMP-12 was effective for degradation of elastic fibers. It has been reported that there were increased partially degraded collagen (high molecular weight collagen fragments) in photoaged skin compared with sun-protected skin. 21 The partially degraded collagen produced by MMP-1 inhibits collagen synthesis. Gelatinases (MMP-9) is needed to “clear away” the partially degraded collagen produced by MMP-1. Therefore, MMP-1, -3, and -12 could play a destructive role, whereas MMP-9 may play a constructive one in ECM metabolism. Compared with the remarkable elevation of MMP-1, -3, and -12 in UVA-exposed skin, lower MMP-1, -3, and -12 but higher MMP-9 levels were found in IPL-irradiated skin, indicating different MMP expression patterns in IPL- and UVA-irradiated skin. This may be a clue to explain why similar MMP expression patterns, whereas different histological changes (collagen I increased in IPL-irradiated skin but elastic fiber degraded in UVA-exposed skin) occurred. TIMP-1 has been suggested to play a protective role in collagen metabolism. 22 Our results showed a induction of TIMP-1 in IPL-irradiated skin similar to that in UVA-exposed skin, suggesting that TIMP-1 may play a less important role in the photorejuvenation effects of IPL.
One thing to be noted is that MMPs are mainly distributed in the epidermis, whereas collagen deposition occurs in the dermis in IPL-treated skin. Histologically, epidermis and dermis are connected by the basement membrane, which can be degraded by gelatinases (MMP-9), which may facilitate the transmission of MMPs. 23 Therefore, there could be an epidermis–dermis interaction and the connective tissue could be influenced by dermal MMPs as well as epidermal MMPs.
In addition, IPL differs from UVA in that IPL sources emit a broad band of 400–1200 nm, whereas UVA has a wavelength of 320–400 nm. Since longer wavelength generally contributes to deeper tissue penetration, IPL may have a more intensified biological effect, leading to acute thermal damage in deeper dermis. In contrast, chronic UVA exposure induces inflammation in the upper dermis, which could result in ECM degradation. 22,24
Conclusion
Our findings demonstrated that IPL and UVA promoted the production of MMP-1, -3, -9, and -12 and TIMP-1 in human skin, with some differences in the expression patterns (remarkable increase of MMP-1, -3, and -12 in UVA-exposed skin, while lower MMP-1, -3, and -12 but higher MMP-9 levels in IPL-irradiated skin). Collagen I fibers increased in IPL-irradiated skin but elastic fibers degraded in UVA-exposed skin. The different expression of MMPs in IPL-irradiated skin compared with UVA-exposed skin may provide a clue to the photorejuvenation effects of IPL.
Footnotes
Acknowledgments
This study was supported by Natural Science Foundation of China (30872269).
Author Disclosure Statement
No conflicting financial interests exist.
Wei Liu and Weijie Gu contributed equally to this work.